Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
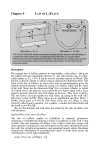
European Heart Journal – Cardiovascular Imaging (2016) 17, 633–634 doi:10.1093/ehjci/jew060 EDITORIAL Global myocardial function, regional myocardial function, and the Daemon of Laplace Jens-Uwe Voigt* Department of Cardiology, University Hospital Gasthuisberg, Catholic University Leuven, Herestraat 49, Leuven 3000, Belgium Online publish-ahead-of-print 13 April 2016 Pierre-Simon Laplace, the famous 18th century French mathematician, physicist, and astronomer, expressed in his book ‘Essai philosophique sur des Probabilités’ his deterministic view on the world with the idea that if a hypothetical intellect would be aware of all laws of nature and the exact condition of all its components at a certain point in time, any past or future state of the universe could be calculated from that.1 This intellect became later popular as ‘Daemon of Laplace’, and the idea was challenged by both philosophers and physicists. Not only that in final consequence such a deterministic world spirit would exclude the existence of a free will, it also causes a logical problem as this intelligence would be part of the system and had to calculate itself. Finally, modern quantum mechanics tells us that both location and velocity of a particle cannot be measured at the same time. Determining the regional work performed by the ventricular myocardium leaves us with a less philosophic problem on a smaller scale, but with a comparable intellectual challenge. And also here Laplace was involved in laying the foundations. In a joint work with Lavoisier, they confirmed in 1780 that oxygen consumption of an animal has an energetic equivalent in the body heat that can melt the ice inside a calorimeter.2 The same principle is nowadays applied when myocardial blood flow and its oxygen extraction are invasively measured as caloric equivalent of the energy consumption of the heart which then can be expressed in J (Joule), Nm (Newton meter), or Ws (Watt second). On the other side, we can measure the work of the heart which is performed towards the body. This ‘external work’ is usually described by the pressure–volume loops of the chambers,3 as the product of pressure (N/m2) and volume (m3) equals work (Nm). However, there is a considerable gap between the consumed energy and the performed external work which is explained by the ‘potential work’ which is needed to build up the static pressure in the chamber4 and by the energy demand of the basic cell metabolism. Both ‘external work’ and ‘potential work’, but not the basic metabolism of the cells, can be determined from invasive haemodynamic measurements that are displayed in a pressure–volume diagram (Figure 1). In ventricular dyssynchrony, myocardial contraction is uncoordinated, and the performed myocardial work is partially wasted by the walls stretching each other. To study such a complicated condition, the assessment of regional myocardial energetics is needed. If pressure is replaced by the local force created by the myocyte (N) and volume is substituted by the length change of this myocyte (m), the resulting force– length loop shows the locally performed work (Nm). However, we are here in a deterministic dilemma. While the assessment of length would be even possible by non-invasive imaging, the direct measurement of local force or wall stress is impossible in vivo without the destruction and, consequently, functional alteration of the tissue. The Daemon of Laplace is back. Many attempts have been made to estimate the forces inside the ventricular wall. While some authors make complex assumptions on a global force distribution modulated by regional deformation behaviour,5 others use simply the invasively measured LV cavity pressure as substitute. In the current publication by Vecera and colleagues, not even that is done. The LV pressure curve shape is only estimated based on the cuff measurement of the systolic blood pressure and cardiac time intervals.6 Earlier work from the same group had shown that this approach has a negligible error compared with the use of invasive LV pressure measurements.7 This new concept of a fully non-invasive assessment of regional myocardial work was now tested for the first time in the clinical setting of patients undergoing cardiac resynchronization therapy (CRT). The authors confirmed earlier observations from animal experiments8 that dyssynchronous hearts waste a lot of energy in the early activated wall (Figure 2). They also demonstrated convincingly that the wasted work is reduced with resynchronization. In this pilot study with only 21 patients, the value of the ‘wasted work ratio’ for predicting CRT response was limited, and the additional consideration of myocardial scar extend proved to be indispensable. However, the concept remains intriguing, and the results from larger, potentially multicentric patient studies can be expected with interest. It can be discussed that the proposed concept estimates only the ‘external work’ performed by the local myocardium. It ignores the basic metabolism of the cells and the potential work that has to be performed and might therefore exaggerate differences between walls compared with true measurements of metabolism, e.g. by myocardial PET scans with Acetate or FDG tracers. Further, both potential work The opinions expressed in this article are not necessarily those of the Editors of EHJCI, the European Heart Rhythm Association or the European Society of Cardiology. * Corresponding author. Tel: +32 16 349016. E-mail: [email protected]; [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2016. For permissions please email: [email protected]. 634 Figure 1 Mechanical work performed by the ventricle can be assessed in the pressure– volume diagram. It consists of the ‘external work’ (EW, green area of the LV pressure volume loop) and the potential work (PW, yellow area) which is needed to build up the static pressure in the chamber. ED, ES—end-diastole, end-systole. The energy needed for the basic metabolism of the cells cannot be displayed in this way. and external work depend directly on local wall stress. This, however, is not measurable in vivo and was therefore substituted with the same LV pressure curve for all segments. Formally, the multiplication of local strain measurements with a single modelled LV pressure curve results only in weighting the systolic part of the strain curve (during high LV pressure) 10–20 times higher than the diastolic part (when LV pressure is very low). It is therefore reassuring that analysing the systolic part of the strain curve only leads to very comparable results as it had been previously shown by others.9 It must be questioned in all these approaches, however, if the assumption of a uniform wall stress distribution is appropriate for remodelled hearts of LBBB patients at all. Commonly, these patients have a dilated LV with a thinned septum while the lateral wall is hypertrophied. And here Laplace enters the stage again. He provided us with a formula that is known by every cardiologist as the ‘Law of Laplace’. It describes in simple terms the relation of the pressure inside a sphere and the stress that can be expected in the wall of the sphere for a given radius and wall thickness. Considering that the lateral wall in remodelled LBBB patient hearts is much thicker than the septum, and that it further thickens during its systolic contraction, the wasted work would appear much higher in the septum while the work performed in the lateral wall would be measured much lower than without wall thickness correction. So maybe the 18th century ‘Law of Laplace’ could help to overcome the daemon that still inherent in many modern approaches of assessing regional myocardial energetics. Editorial Figure 2 In dyssynchronous hearts, the ‘external work’ differs between regions. Late activated regions (A) perform a lot of external work (green area of the counter-clockwise running loop) while in early activated regions (B) part of this work is wasted due to stretching during systole (red area where the loop runs clockwise). Note that for regional work assessment, LV pressure is only a surrogate for the local force to which the myofibrils are exposed. This force depends on wall thickness and curvature. Black arrow, direction of loop. Conflict of interest: None declared. References 1. Laplace P-S. Essai philosophique sur les probabilités. Paris: Courcier; 1814. 2. Lavoisier AL, Laplace P-S. Mémoire sur la caleur. Mémoires de mathématique et de physique, tires des registres de l’Académie royale des sciences, année 1780. pp 355 –408. 3. Khalafbeigui F, Suga H, Sagawa K. Left ventricular systolic pressure-volume area correlates with oxygen consumption. Am J Physiol 1979;237:H566 – 9. 4. Suga H. Total mechanical energy of a ventricle model and cardiac oxygen consumption. Am J Physiol 1979;236:H498 –505. 5. Delhaas T, Arts T, Prinzen FW, Reneman RS. Regional fibre stress-fibre strain area as an estimate of regional blood flow and oxygen demand in the canine heart. J Physiol 1994;477(Pt3):481–96. 6. Vecera J, Penicka M, Eriksen M, Russell K, Bartunek J, Vanderheyden M et al. Wasted septal work in left ventricular dyssynchrony: a novel principle to predict response to cardiac resynchronization therapy. Eur Heart J Cardiovasc Imaging 2016; 17:624 – 32. 7. Russell K, Eriksen M, Aaberge L, Wilhelmsen N, Skulstad H, Remme EW et al. A novel clinical method for quantification of regional left ventricular pressurestrain loop area: a non-invasive index of myocardial work. Eur Heart J 2012;33: 724 – 33. 8. Prinzen FW, Hunter WC, Wyman BT, McVeigh ER. Mapping of regional myocardial strain and work during ventricular pacing: experimental study using magnetic resonance imaging tagging. J Am Coll Cardiol 1999;33:1735 –42. 9. De Boeck BW, Teske AJ, Meine M, Leenders GE, Cramer MJ, Prinzen FW et al. Septal rebound stretch reflects the functional substrate to cardiac resynchronization therapy and predicts volumetric and neurohormonal response. Eur J Heart Fail 2009;11: 863 –71.