Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Rheumatic fever wikipedia , lookup
Echocardiography wikipedia , lookup
Jatene procedure wikipedia , lookup
Artificial heart valve wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Aortic stenosis wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
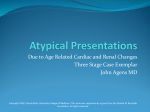
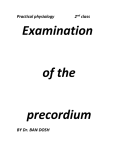
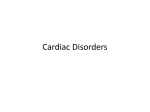
Adult Heart Murmurs Or, Between the Lubs and the Dubs Paul D. Simmons, MD, FAAFP Faculty Physician St. Mary’s Family Medicine Residency Program Grand Junction, Colorado Learning Objectives At the end of this presentation, you should be able to: 1. Distinguish innocent and abnormal heart murmurs in patients and classify them as systolic, diastolic or continuous. 2. Formulate a differential diagnosis of specific cardiac sounds and explain the pathology of heart murmurs to patients. 3. Evaluate diagnostic factors in patients with suspected heart murmurs using cost-effective cardiac testing. Question 1 Who invented the stethoscope? A. William Osler B. Robert Koch C. Rene Laennec D. Edward Jenner E. Moses Maimonides Question 2 Which of the following murmurs would be heard during diastole? A. Aortic stenosis (AS) B. Pulmonic stenosis (PS) C. Tricuspid regurgitation (TR) D. Mitral stenosis (MS) E. Mitral regurgitation (MR) Question 3 You are examining a 30 year old woman, a new patient to your practice. You do not have medical records for her yet, but she states she has no history of a murmur. On auscultation, you hear a murmur. Which of the following would NOT be suggestive of a benign, functional murmur? A. Systolic murmur of short duration (i.e., not holosystolic) B. Intensity less than or equal to 2/6 C. Early to mid-systolic D. Decreased intensity when the patient stands or Valsalvas E. Diastolic murmur Why Should We Care? “Auscultation has a reported sensitivity of 70% and a specificity of 98% for detection of valvular heart disease.” Orient JM (2010). Sapira’s Art & Science of Bedside Diagnosis, 4th edition. Philadelphia, PA: Wolters Kluwer Health. Image public domain, copyright expired, WikiCommons Image from Wikicommons user CFCF, Creative Commons AS / PS MR / TR MVP Image from Wikicommons user CFCF, Creative Commons AR / PR MS / TS Image from Wikicommons user CFCF, Creative Commons Another Way to Remember Valve Stenosis Regurgitation Aortic Systolic “Manly” Diastolic HOOOT Dub Lub hoot Systolic “Manly” Diastolic HOOOT Dub Lub hoot Diastolic Systolic “Blowing” Lub hoot Hoot Dub Diastolic Systolic “Blowing” Lub hoot Hoot Dub Pulmonic Tricuspid Mitral Valve Stenosis Regurgitation Aortic Systolic “Manly” Diastolic HOOOT Dub Heard at A, carotid Lub hoot Systolic “Manly” Diastolic HOOOT Dub Heard at P, no carotid Lub hoot Diastolic Systolic “Blowing” Lub hoot Holosystolic, T area, no rad Hoot Dub Diastolic Systolic “Blowing” Lub hoot Holosystolic, M area, axilla Hoot Dub Pulmonic Tricuspid Mitral Valve Stenosis Regurgitation Aortic Systolic “Manly” Diastolic HOOOT Dub Heard at A, carotid Lub hoot Heard at LLSB, decrescendo Systolic “Manly” Diastolic HOOOT Dub Heard at P, no carotid Lub hoot Heard at LUSB, decrescendo Diastolic Systolic “Blowing” Pulmonic Tricuspid Lub K-hoot Hooot Dub Opening snap, heard at T area, Holosystolic, T area, no presystolic “rumble” Mitral Diastolic Systolic “Blowing” Lub K-hoot Opening snap, heard at M area, presystolic “rumble” Hooot Dub Holosystolic, M area, axilla Phonocardiograms AS may have ejection “click” at onset of murmur A “continuous” murmur… Image from Wikicommons user Madhero88, creative commons license Systolic Murmur Pathophysiology Flow across an obstruction: AS, PS or idiopathic hypertrophic subaortic stenosis Increased flow across a normal valve: ASD – not from flow across the defect, but rather from increased ejection volume Regurgitation from high pressure to low pressure: MR, TR or VSD Diastolic Murmur Pathophysiology Generally, diastolic murmurs are softer and lower pitch because of lower pressure during diastole Regurgitant flow across an aortic or pulmonic (semilunar) valve Abnormal flow across tricuspid or mitral valves, or “rumble” from increased volume across a normal A-V valve How Good Are Murmurs at Detecting Valve Disease? From McGee S. (2012), p. 361 “Typical” murmur + LR - LR Aortic stenosis 5.9 0.1 Sev aortic stenosis 3.6 0.06 Mitral regurg 5.4 0.3 Tricuspid regurg 14.6 VSD 24.9 MVP 12.1 AR 9.9 PR 17.4 0.3 Maneuvers and Murmurs Inspiration: decreases intrathoracic pressure, increases venous return to the R heart, and thus increasing TR murmur (Carvallo sign) Valsalva: increases intrathoracic pressure, decreases venous return to the heart, decreases MVP murmur due to decreased afterload Squat-to-stand: decreased venous return, moving mitral leaflet closer to the septum, and increases IHSS murmur and MVP murmur Stand-to-squat: increases venous return, so softens IHSS murmur Continuous Murmurs - “Continuous” murmurs aren’t necessarily continuous, but they don’t obey systolic / diastolic boundaries. - Partial DDx of continuous murmurs: note that most of these are external to the heart itself - Patent ductus arteriosus L to R shunt from ASD A-V fistula Coarctation of the aorta Partial obstruction of the pulmonary artery by PE Venous hum “Mammary souffle” of pregnancy Question 4 You are seeing a 62 year old man with an apparently new systolic murmur. Which of the following would NOT be an indication for immediate echocardiography? A. Systolic murmur with new chest pain and dyspnea B. Asymptomatic patient with a 2/6 systolic murmur C. Asymptomatic patient with a 4/6 systolic murmur D. Asymptomatic patient with a 2/6 systolic murmur and decreased carotid upstroke E. All of the above are indications for echocardiography When to Get an Echo • Any murmur with cardiac symptoms • Asymptomatic patients with a diastolic murmur • Asymptomatic with a loud (3+/6) systolic murmur • Systolic murmur with other abnormal cardiovascular findings (e.g., systolic click, decreased carotid upstroke) Figure 3 from Shipton B, Wahba H. (2001), AFP 63 (11): 2201 ff. From Choosing Wisely: Cardiology Don’t perform echocardiography as routine follow-up for mild, asymptomatic native valve disease in adult patients with no change in signs or symptoms. http://www.choosingwisely.org/doctor-patient-lists/american-college-of-cardiology/ Question 5 You are examining a 72 year old woman with a history of COPD, ischemic and hypertensive cardiomyopathy, and DVT without PE. You hear an extra heart sound beyond S1 and S2. Which of the following statements is TRUE? A. S3 and S4 are best heard with the patient supine while holding a deep breath. B. S3 is caused by the atrial jet hitting a volume-overloaded ventricle. C. S4 is caused by sudden tensing of mitral valve chordae tendinae. D. S3 is always abnormal. E. All of the above are true. Some Pearls About S3 and S4 • S3 and S4 are heard best in the L lateral decubitus position, and both are more “felt” with the eardrums than heard – very low frequency • S3 is caused by atrial filling into a volume overloaded ventricle • S4 is caused by atrial jet hitting a stiff, hypertrophic ventricle (pressure overload) • S3 can be normal in children Excellent Physical Exam Resources McGee S. (2012). Evidence-Based Physical Diagnosis, 3rd edition. Orient JM. (2010). Sapira’s Art & Science of Bedside Diagnosis, 4th edition. Stanford Medicine 25 Website: stanfordmedicine25.stanford.edu Heart Sounds & Murmurs app (Android) Heart Murmur Pro (iOS, $2.99) References Orient JM. (2010). Sapira’s Art & Science of Bedside Diagnosis, 4th ed. Philadelphia, PA: Wolters Kluwer Health. McGee S. (2012). Evidence-Based Physical Diagnosis, 3rd ed. (Chapter 41 – Heart Murmurs, General Principles, p. 351ff.) Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorayja P, Sundt TM 3rd, Thomas JD. (2014). AHA/ACC Guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology / American Heart Association task force on practice guidelines. J Am Coll Cardiol 2014; 63(22):e57ff. Mineo K, Cummings J, Josephson R, Nanda NC. (2001). Acquired left ventricular outflow tract obstruction during acute myocardial infarction: Diagnosis of a new cardiac murmur. Am J Geriatr Cardiol., 10(5): 283-5. Thank you! Email: [email protected] Twitter: @pauldsimmons