Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Artificial heart valve wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Heart failure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Jatene procedure wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
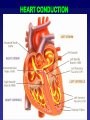
HEART Part 2 A&P Instructor Terry Wiseth HEART CONDUCTION Throughout the heart are clumps of specialized cardiac muscle tissue whose fibers contain only a few myofibrils Initiate and distribute cardiac impulses throughout the myocardium 2 HEART CONDUCTION intrinsic ability to generate and conduct nerve impulses conducts impulse for proper contraction sequence of heart 3 HEART CONDUCTION intrinsic ability to generate and conduct nerve impulses conducts impulse for proper contraction sequence of heart 4 HEART CONDUCTION intrinsic ability to generate and conduct nerve impulses conducts impulse for proper contraction sequence of heart 5 SINOATRIAL NODE Cell area located on the posterior part of the right atrial wall, adjacent to the junction of the superior vena cava and the right atrium “Pacemaker” signals atria to contract 6 SINOATRIAL NODE depolarization of the SA node is the first step of the cardiac cycle does not produce enough energy to be recorded by the EEG cells in the SA node transmit impulses six times faster than do ordinary cell-to-cell interconnections 7 SINOATRIAL NODE The SA node sets the heart rate at 95 beats per minute 60 beats per minute is intrinsic to the atria alone 20 - 40 beats per minute is intrinsic to the ventricles alone 8 HEART CONDUCTION SINOATRIAL NODE Acetycholine released by parasympathetic system of ANS slows SA node to 72 beats per minute Other hormones affect heart rate by influencing SA node 10 ECTOPIC PACEMAKER Site other than SA node develops an abnormal self-excitability Produces extra beats Irregularly pace the heart for short periods of time Nicotine and caffeine can trigger these events 11 ATRIOVENTRICULAR NODE made up of another cluster of specialized cardiac conduction system cells forms a pathway for impulse conduction that bridges between the atria and ventricles delays impulse for atria to finish contraction 12 HEART CONDUCTION ATRIOVENTRICULAR NODE Depolarization of the AV node is relatively slow due to the intrinsic characteristics of its cells This causes a delay in the transmission of the depolarization wave to the ventricles transmission of the wave through the AV node is relatively weak considered silent on the electrocardiogram 14 ATRIOVENTRICULAR NODE damaged AV node ventricles contract intrinsically slower may require an artificial pacemaker 15 BUNDLE OF HIS a compact tract of cardiac conduction system fibers also called the AV bundle route for signals to leave the AV node 16 BUNDLE OF HIS tract down the interventricular septum The right and left branches spread the electrical impulse to the right and left ventricles 17 PURKINJE FIBERS conduction system fibers which form a rapid conduction network within the myocardium located at the ends of the bundle branches 18 PURKINJE FIBERS responsible for propagating the depolarization wave to all cardiac muscle cells The QRS Complex of the electrocardiogram represents the ventricular depolarization of contraction 19 HEART CONDUCTION CONDUCTION SA node AV node bundle of His Purkinje fibers CONDUCTION Contraction begins at the heart apex and progresses upwards milking action of ventricular contraction and the spiral arrangement of the ventricular muscle fibers twist and wring out the blood 22 HEART CONDUCTION CONTROL OF CONTRACTION brain is able to affect heart rate via 1) parasympathetic nerve impulses heart-slowing 2) sympathetic nerve impulses increase heart rate 24 CONTROL OF CONTRACTION Click to View Baroreceptor control of heart rate CARDIAC RHYTHM normal resting 70-80 beats/min Systole Contraction Diastole Expansion 26 VENTRICULAR DIASTOLE during ventricular diastole cusps hang loosely into ventricular chamber 27 VENTRICULAR SYSTOLE during (at start of ) ventricular systole the resulting increased blood pressure developing in the ventricle forces the flaps up together shutting the AV valves 28 VENTRICULAR SYSTOLE semilunar valves forced open 29 VENTRICULAR DIASTOLE semilunar valves closed from back flow pressure of aortic and pulmonary trunks 30 HEART SOUNDS Lubb - dupp sounds are due to vibrations in the heart tissues created as the blood flow is suddenly increased or slowed with the contraction and relaxation of the heart chambers created with the opening and closing of the valves 31 HEART SOUNDS closing of valves causes vibrations in heart wall “lubb-dupp” sound of heartbeat “lubb” S1 lower, louder closing of AV valves start of ventricular systole “dupp” S2 softer, sharper closing of semilunar valves end of ventricular systole 32 ELECTROCARDIGRAM Comprehensive image of the hearts electrical activity supplies a composite recording of all action potentials produced by nodal and muscle cells three principle deflections P wave QRS complex T wave 33 EKG COMPONENTS EKG COMPONENTS P WAVE Signal from the SA node spreads through the atria atrial systole 36 QRS COMPLEX Firing of SA node ventricular systole 37 S-T SEGMENT Following ventricular contraction and the QRS complex is a brief period of low electrical activity On the electrocardiogram this appears as the S-T segment 38 T WAVE Ventricular repolarization is represented by the T-wave on the electrocardiogram The T-wave deflection is also in the same direction of the largest deflection of the QRS complex 39 EKG SUMMARY depolarization repolarization READING EKG Important to note the size of the deflection waves at certain time intervals 41 ENLARGEMENT OF P-WAVE Indicates enlargement of the atria atrial stenosis mitral valve narrows blood backs into the left atrium and there is an expansion of the atrial wall 42 LENGTHENED P-R INTERVAL Occurs because the heart tissue, covered by the P-Q interval, namely the atria and AV node is scarred or inflamed Impulse, as a result, travels at a slower rate and the interval is lengthened Atherosclerotic disease Rheumatic fever 43 ENLARGED Q-WAVES AND R-WAVES Enlarged R wave generally indicates enlarged ventricles Enlarged Q-wave may indicate a myocardial infarction 44 S-T SEGMENT Elevated S-T segment acute myocardial infarction Depressed S-T segment heart muscle receives insufficient oxygen 45 T-WAVE Flat when the heart muscle is receiving insufficient oxygen May be elevated during hyperkalemia High levels of potassium in bloodstream 46 CARDIAC CYCLE 1) Ventricular filling 2) Atrial systole 3) Isovolumetric ventricular contraction 4) Rapid ventricular ejection 5) Isovolumetric ventricular relaxation 47 1) VENTRICULAR FILLING AV valves open due to low ventricular pressure blood passively enters the ventricles P wave starts 48 2) ATRIAL SYSTOLE SA node fires contraction of the atrium stops the pulmonary venous and systemic inflow atrial contraction completes the filling of the ventricles pressure in the ventricles increases closing the AV valves phase is indicated by the P wave 49 3) ISOVOLUMETRIC CONTRACTION ventricular contraction causes the pressure to rise in the ventricles AV valves close blood is not ejected from the ventricles atria relax heart sound S1 phase is indicated by the QRS complex 50 4) VENTRICULAR EJECTION the pressure in the ventricles exceed the pulmonary and systemic pressures causing the semilunar valves to open ventricle continues to contract rapidly ejecting blood to the aorta and pulmonary trunk 51 4) VENTRICULAR EJECTION Ventricle contains 130 ml blood EDV (End Diastolic Volume) ventricles eject 54% (ejection fraction) of the EDV during contraction blood remaining behind is called ESV (End Systolic Volume) during rigorous exercise 90% may be ejected ejection fraction is an important measure of cardiac health 52 5) ISOVOLUMETRIC RELAXATION Ventricles expand causing pressure to drop semilunar valves close as the ventricular pressure falls below the systemic and pulmonary diastolic level 53 5) ISOVOLUMETRIC RELAXATION ventricular pressures continue to fall until it is slightly below atrial pressure AV valves open blood begins to fill the ventricles phase is indicated by the T wave heart sound S2 54 CARDIAC CYCLE VOLUME CHANGES Ventricles pump as much blood as they receive both ventricles eject the same volume of blood ESV (leftover) 60 ml atrial diastole +30 ml atrial systole +40 ml total EDV 130 ml stroke volume -70 ml ESV 60 ml 56 VOLUME CHANGES If RV pumped more than LV could handle on return causes hypertension and edema in the lungs fluid swells the lungs impairing gas exchange 57 VOLUME CHANGES If LV pumped more blood than RV can handle on return results in hypertension and edema in the body can lead to aneurysms, stroke, kidney failure, heart failure 58 CONGESTIVE HEART FAILURE Failure of either ventricle to eject blood effectively can be caused by: 1) myocardial infarcted weakened heart muscle 2) chronic hypertension 3) valvular insufficiency 4) congenital defects 59 CONGESTIVE HEART FAILURE Left ventricle failure pulmonary edema shortness of breath sense of suffocation Right ventricle failure systemic edema enlargement of liver swelling of fingers, ankles, feet 60 CONGESTIVE HEART FAILURE Left ventricle failure pulmonary edema shortness of breath sense of suffocation Right ventricle failure systemic edema enlargement of liver swelling of fingers, ankles, feet 61 CARDIAC OUTPUT volume pumped by each ventricle per minute CO = Heart Rate (HR) X Stroke Volume (SV) HR = 75 bpm SV = 70 ml/beat CO = 75 X 70 = 5,250 ml/min = 5.25 L/min total volume of blood is 4-6 L thus entire volume of body’s blood is pumped through each minute vigorous exercise increases CO up to 21 L/min 62 CARDIAC OUTPUT Cardiac output and peripheral resistance determine blood pressure Healthy young adult 120 mm Hg/ 80 mm Hg 63 HEART RATE Normal 72 bpm Tachycardia rate above 100 bpm stress, anxiety, drugs, disease, elevated body temperature Bradycardia HR below 60 bpm sleep, well trained athlete, low body temperature 64 STROKE VOLUME Governed by three factors 1) pre-load 2) contractility 3) after-load 65 PRE-LOAD Determined by volume of blood in ventricles stretched myocardial muscle is able to contract more forcefully thus expel more blood and increasing CO 66 CONTRACTILITY Refers to the strength of contraction for a given pre-load measures myocyte receptivity to stimulation solutions of glucagon and calcium chloride are standard emergency treatment for heart attacks digitalis acts as a cardiac stimulant to treat congestive heart failure barbiturates are negative agents which reduce myocyte response to stimulation 67 AFTER-LOAD Blood pressure in arteries outside the semilunar valve opposes the opening of semilunar valves increased after-load reduces the stroke volume 68 AFTER-LOAD arterial circulation impediments increase afterload scar tissue (lung diseases) emphysema, chronic bronchitis cor pulmonale RV failure due to obstructed pulmonary circulation Emphysema 69 HEART ABORMALITIES Cardiomyopathy The myocardium functions poorly and the heart is large and dilated MYOCARDIAL INFARCTION 71 MYOCARDIAL INFARCTION MI ,“heart attack” Within the lumen of the coronary can be seen a dark red recent coronary thrombosis The dull red color to the myocardium to the lower right of the thrombus is consistent with underlying myocardial infarction 72 MYOCARDIAL INFARCTION left ventricular wall sectioned lengthwise to reveal a recent myocardial infarction The center of the infarct contains necrotic muscle that appears yellow-tan Remaining viable myocardium is reddishbrown 73 MYOCARDIAL INFARCTION Myocardial infarction necrotic tissue 74 MYOCARDIAL INFARCTION histological acute myocardial infarction contraction band necrosis myocardial fibers are beginning to lose cross striations nuclei are not clearly visible many irregular darker pink wavy contraction bands extending across the fibers 75 ATRIAL FLUTTER Cells in the atria set off extra contractions the atria beats 400-500 beats per minute early firing can cause premature ventricular contractions (PVCs) often due to irritation of the heart by stimulants, emotional stress, or lack of sleep can lead to ventricular fibrillation 76 VENTRICULAR FIBRILLATION An arrhythmia caused by electrical signals arriving at different regions of the myocardium at widely different times squirming, uncoordinated contractions “bag of worms” no pumping of blood ischemia rapidly follows 77 CARDIAC ARREST A cessation of cardiac output ventricles may be motionless or in fibrillation 78 DEFIBRILLATION Heart is given a strong electric shock with a pair of electrodes 79 DEFIBRILLATION Depolarizes the entire myocardium and stops the fibrillation hope that the SA node will resume in sinus rhythm Atrial fibrillation Normal sinus rhythm Defibrillation shocks 80 PACEMAKER A pacing system stimulates the heart muscle with precisely timed discharges of electricity cause the heart to beat in a manner very similar to a naturally occurring heart rhythm 81 PACEMAKER The pacemaker sends tiny electrical impulses to start a heartbeat The electrode is designed to relay information (sense) about your heart's own electrical activity to the pacemaker and to deliver electrical impulses (paces) only when the heart needs them 82 PACEMAKER DYNAMIC CARDIOMYOPLASTY involves harvesting the the Latissimus Dorsi the muscle is wrapped around the surface of the heart the nerve to the muscle is stimulated (with a specialized pacemaker device) allowing the muscle to contract improves the ejection of blood from the heart lessens the symptoms of heart failure 84 DYNAMIC CARDIOMYOPLASTY DYNAMIC CARDIOMYOPLASTY HYPERTENSION The left ventricle is markedly thickened in this patient with severe hypertension that was untreated for many years hypertension creates a greater pressure load on the heart to induce the hypertrophy 87 AORTIC TEAR a sudden deceleration injury in a vehicular accident can produce a tear in the aorta tear is just distal to the great vessels the tear leads to sudden loss of blood and shock It is widely believed that Princess Diana died from an aortic tear brought on by a sudden deceleration 88 AORTIC TEAR AORTIC TEAR BACTERIAL INFECTION Endocarditis blue bacterial colonies on the lower left extending into the pink connective tissue of the valve valves are relatively avascular high dose antibiotic therapy is needed to eradicate the infection 91 BACTERIAL INFECTION patient with infective endocarditis and blood culture positive for Staphylococcus aureus small linear subungual splinter hemorrhage 92 HEART TUMOR heart of a two year old child who died suddenly at autopsy, a large firm, white tumor mass was found filling much of the left ventricle tumors of the heart are rare 93 HEART TUMOR PULMONARY THROMBOEMBOLUS Blood clots formed elsewhere in the body can dislodge and move through the larger blood vessels and heart and become lodged in the smaller pulmonary circuit blood vessels causing a blockage or bursting of the blood vessel HEART LUNG MACHINE HEART LUNG MACHINE FEET BLUE BLOOD TO PUMP RED BLOOD TO BODY HEAD ATRIAL SEPTAL DEFECT A defect involving both the atrial and the ventricular septums allows blood to pass freely between the two ventricles and the atriums 98 ATRIAL SEPTAL DEFECT The valve apparatus at the junction between atriums and ventricles is "shared" effectively only one valve instead of the normal two Blood flow and pressure in the lung circulation is substantially increased 99 ATRIAL SEPTAL DEFECT often results in early onset of symptoms with: breathlessness poor feeding slow weight gain defect is very common in babies with Down syndrome 100 VENTRICULAR SEPTAL DEFECT FOSSA OVALIS depression in interatrial septum opening which exists in fetal heart foramen ovale RA RV 102 HEART CHANGES AT BIRTH At birth, the first breath inflates the lungs lowers the resistance to blood flow thus increases the volume of blood flowing through them thereby increasing the amount of blood returning from the pulmonary trunk to the heart all of which results in increased pressure in the left atrium 103 FETAL CIRCULATION FETAL CIRCULATION HEART CHANGES AT BIRTH increased pressure in the left atrium forces the flap covering the foramen ovale against the interatrial septum blocking off communication between the right and left atrium 106 HEART CHANGES AT BIRTH closure of the ductus arteriosus takes place almost immediately after birth due to muscular contraction mediated by, bradykinin released from the lungs after the newborn's first breath 107 HEART CHANGES AT BIRTH In some instances, the ductus arteriosus does not obliterate within the first few days leaving a left to right shunt 108 HEART CHANGES AT BIRTH There are two shortcuts; normally, both of them close up at birth or shortly thereafter ductus arteriosus a small blood vessel connecting the pulmonary artery and aorta foramen ovale a small hole between the left and right atria 109 DUCTUS ARTERIOSUS BEFORE AND AFTER HEART CHANGES AT BIRTH Openings and blood vessels close at birth and if they do not two conditions may result: Patent Ductus Arteriosus (PDA) Patent Foramen Ovale (PFO) 111 PATENT DUCTUS ARTERIOSUS HEART CHANGES AT BIRTH Either of these conditions can cause fatigue difficult or rapid breathing failure to grow normally chronic respiratory infections Large openings can lead to heart failure and death 113 DUCTUS ARTERIOSUS REPAIR END HEART Part 2