Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
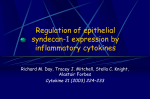
TNF-a and myocardial depression in endotoxemic rats: temporal discordance of an obligatory relationship XIANZHONG MENG, LIHUA AO, DANIEL R. MELDRUM, BRIAN S. CAIN, BRIAN D. SHAMES, CRAIG H. SELZMAN, ANIRBAN BANERJEE, AND ALDEN H. HARKEN Department of Surgery, University of Colorado Health Sciences Center, Denver, Colorado 80262 endotoxin; cardiac contractility; cycloheximide; dexamethasone; tumor necrosis factor binding protein; tumor necrosis factor-a ENDOTOXIN (lipopolysaccharide, LPS) depresses myocar- dial contractility in laboratory animals (8, 11, 18, 20, 27, 28) and humans (29, 34) and is responsible for cardiac dysfunction associated with sepsis (29). However, the mechanism by which LPS causes cardiac dysfunction remains obscure. Previous studies have suggested that sepsis-induced myocardial depression was mediated by secondary factors (14, 15, 30). Indeed, LPS stimulates monocytes and macrophages and thereby elicits a cascade of proinflammatory cytokines. Perhaps the proximal effectors of the cytokine cascade include tumor necrosis factor-a (TNF-a) and interleukin-1. Dysregulated TNF-a production is critical for the development of septic shock (36, 37). TNF-a has reThe costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. R502 cently been demonstrated to be responsible for the in vitro depression of cardiac myocyte contractility by human septic shock serum (12). Furthermore, TNF-a has been shown to depress the contractility of isolated cardiac myocytes (10, 39) and in vivo instrumented hearts (22, 23, 26). However, exogenous TNF-a appears to induce immediate depression in vitro (5, 25) and delayed depression in vivo (22). The temporal relationship between endogenous TNF-a and myocardial depression in endotoxemia remains to be determined. Furthermore, the role of endogenous TNF-a in endotoxemic myocardial depression appears to be controversial. Pretreatment with a TNF-a-neutralizing antibody has been reported to fail to prevent myocardial contractile dysfunction in a rabbit endotoxemic shock model (24). Using low-dose LPS, we created a rat model of endotoxemia not complicated by shock (18). We sought to examine the influence of suppression of TNF-a production and neutralization of TNF-a in this model to determine the role of TNF-a in endotoxemic myocardial depression. Myocardial tissue produces TNF-a after a systemic exposure to LPS (9, 19). Inhibition of protein synthesis could be sufficient to abolish LPS-induced myocardial TNF-a production. We have previously reported that dexamethasone (Dex) suppresses LPS-induced increase in circulating and myocardial TNF-a levels (19), and Brady and colleagues have demonstrated that pretreatment with glucocorticoids prevents LPS-induced contractile dysfunction of guinea pig cardiac myocytes (4). It is intriguing to examine whether inhibition of protein synthesis with cycloheximide (CHX) or immunosuppression with Dex prevents the contractile dysfunction of intact heart in this rat model of endotoxemia without shock. Soluble TNF receptors (also termed TNF binding proteins, TNFBP) and antibodies to TNF-a can neutralize TNF-a and eliminate TNF-a bioactivities (10, 21, 38). In animal models of sepsis or endotoxemia, TNFBP and antibodies to TNF-a can prevent shock (1, 37) or mortality (1, 3, 16, 21, 38). TNFBP has also been shown to abolish the in vitro negative inotropic properties of TNF-a in cardiac myocytes (10). The influence of TNFBP on in vivo endotoxemic myocardial depression remains to be determined. The purposes of this study were 1) to delineate the temporal relationship of LPS-induced increase in circulating and myocardial TNF-a with myocardial depression, 2) to examine the influences of protein synthesis inhibition and immunosuppression on LPS-induced TNF-a production and myocardial depression, and 3) to examine the influence of neutralization of TNF-a with TNFBP on endotoxemic myocardial depression. 0363-6119/98 $5.00 Copyright r 1998 the American Physiological Society Downloaded from http://ajpregu.physiology.org/ by 10.220.33.3 on June 15, 2017 Meng, Xianzhong, Lihua Ao, Daniel R. Meldrum, Brian S. Cain, Brian D. Shames, Craig H. Selzman, Anirban Banerjee, and Alden H. Harken. TNF-a and myocardial depression in endotoxemic rats: temporal discordance of an obligatory relationship. Am. J. Physiol. 275 (Regulatory Integrative Comp. Physiol. 44): R502–R508, 1998.—Exogenous tumor necrosis factor-a (TNF-a) induces delayed myocardial depression in vivo but promotes rapid myocardial depression in vitro. The temporal relationship between endogenous TNF-a and endotoxemic myocardial depression is unclear, and the role of TNF-a in this myocardial disorder remains controversial. Using a rat model of endotoxemia not complicated by shock, we sought to determine 1) the temporal relationship of changes in circulating and myocardial TNF-a with myocardial depression, 2) the influences of protein synthesis inhibition or immunosuppression on TNF-a production and myocardial depression, and 3) the influence of neutralization of TNF-a on myocardial depression. Rats were treated with lipopolysaccharide (LPS, 0.5 mg/kg ip). Circulating and myocardial TNF-a increased at 1 and 2 h, whereas myocardial contractility was depressed at 4 and 6 h. Pretreatment with cycloheximide or dexamethasone abolished the increase in circulating and myocardial TNF-a and preserved myocardial contractile function. Similarly, treatment with TNF binding protein immediately after LPS prevented myocardial depression. We conclude that endogenous TNF-a mediates delayed myocardial depression in endotoxemic rats and that inhibition of TNF-a production or neutralization of TNF-a preserves myocardial contractile function in endotoxemia. TNF-a AND ENDOTOXEMIC MYOCARDIAL DEPRESSION MATERIALS AND METHODS Fig. 1. Experimental protocols. LPS, lipopolysaccharide; TNF-a, tumor necrosis factor-a; CHX, cycloheximide; Dex, dexamethasone; TNFBP, TNF binding protein. through the right atrium, and serum was prepared by centrifugation and stored at 270°C. Hearts were excised, and coronary blood vessels were flushed with 10 ml of phosphatebuffered saline (pH 7.4, 4°C) by retrograde perfusion through the aortic root. After removal of the major vessels and atria, ventricular (both left and right) tissue was frozen in liquid nitrogen and stored at 270°C. To examine the temporal relationship of cardiac contractile dysfunction with changes in TNF-a levels, a group of rats was treated with LPS (0.5 mg/kg ip) and another group with bacteriostatic normal saline (0.4 ml ip). Rats were killed 2, 4, or 6 h after the treatment. Hearts were isolated, and intrinsic contractility was assessed by the Langendorff method. Effects of protein synthesis inhibition on LPS-induced changes in circulating and myocardial TNF-a levels and cardiac contractile depression were evaluated by administration of CHX (0.5 mg/kg ip) 3 h before LPS. Serum and ventricular myocardium were collected from a group of CHXpretreated rats at 1 h after LPS treatment for TNF-a assay. Hearts were isolated from another group of CHX-pretreated rats at 6 h after LPS treatment for the assessment of contractile function. Four control rats were treated with CHX alone (0.5 mg/kg ip). Serum and ventricular myocardium were collected from two rats at 4 h (matching the time of CHX treatment in rats treated with CHX and LPS) for TNF-a assay. Hearts were isolated from two rats at 9 h (matching time of CHX treatment in rats treated with CHX and LPS) for the assessment of contractile function. The CHX dose used in this study has been demonstrated to inhibit de novo protein synthesis in rat tissues (31). Previous work demonstrated that this dose of CHX was sufficient to abolish LPS-induced myocardial resistance to ischemia/reperfusion (19). Effects of immunosuppression with glucocorticoids on LPSinduced changes in circulating and myocardial TNF-a levels and cardiac contractile depression were examined by administration of Dex (8.0 mg/kg iv) 30 min before LPS treatment. Our previous work demonstrated that Dex at this dose was effective in inhibiting LPS-induced TNF-a production (19). A group of Dex-pretreated rats was killed at 1 h after LPS treatment, and serum and ventricular myocardium were prepared for TNF-a assay. Another group of Dex-pretreated rats were killed at 6 h after LPS treatment, and hearts were isolated for the assessment of contractile function. Four control rats were treated with Dex alone (8.0 mg/kg iv). Serum and ventricular myocardium were collected from two rats at 1.5 h (matching time of Dex treatment in rats treated with Dex and LPS) for TNF-a assay. Hearts were isolated from the other two rats at 6.5 h (matching time of Dex treatment in rats treated with Dex and LPS) for the assessment of contractile function. Effects of TNFBP on LPS-induced cardiac contractile depression were examined by administration of TNFBP (40 or 80 µg/kg iv, ,7.5 or 15 nM in blood by calculation) immediately after LPS treatment. TNFBP used at a similar dose (11 nM) has been shown to completely abolish TNF-a cytotoxicity to 1591-RE 3.5 cells and contractile depression induced by TNF-a in isolated feline cardiac myocytes (10). Control rats were treated with TNFBP alone (80 µg/kg iv). Rats were killed at 6 h after treatment, and hearts were isolated for the assessment of contractile function. TNF-a assay. Immediately before TNF-a assay was performed, myocardium was homogenized with a tissue homogenizer (Tekmar, Cincinnati, OH) in four volumes of phosphatebuffered saline (pH 7.4, 4°C). After centrifugation at 2,500 g at 4°C for 20 min, the supernatant was collected for TNF-a assay. TNF-a levels in serum and myocardium were measured using an ELISA system containing a hamster anti- Downloaded from http://ajpregu.physiology.org/ by 10.220.33.3 on June 15, 2017 Animals. Male Sprague-Dawley rats, body weight 300–325 g (Sasco, Omaha, NE), were acclimated in a quarantine room and maintained on a standard pellet diet for 2 wk before initiation of the experiments. All animal experiments were approved by the Animal Care and Research Committee of the University of Colorado Health Sciences Center. All animals received humane care in compliance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals. Chemicals and reagents. Dex was purchased from ElkinsSinn, (Cherry Hill, NJ). Human TNFBP was a generous gift from Immunex. This TNFBP is a chimeric fusion protein consisting of two molecules of human TNFBP2 linked by the Fc portion of the human IgG1 (21). This chimeric dimer of TNFBP2 has been shown to be more effective in neutralizing TNF-a than monomeric TNFBP2 or TNFBP1 (10). The TNF-a assay kit was obtained from Genzyme (Cambridge, MA). LPS (from Salmonella typhimurium), CHX, and all other chemicals were obtained from Sigma (St. Louis, MO). Experimental protocols. The rat model of endotoxemia used in this study has been previously reported (18, 20). A single sublethal dose of LPS (0.5 mg/kg ip) induces time-dependent cardiac contractile depression. The cardiac contractility is maximally depressed at 6 h after LPS exposure and completely normalized at 24 h. Mean arterial pressure is not affected in this model, although this dose of LPS causes low fever and body weight loss (18, 20). The experimental protocols are depicted in Fig. 1. To examine the effect of LPS on circulating and myocardial TNF-a levels, a group of rats was treated with LPS (dissolved in bacteriostatic normal saline, 0.5 mg/kg ip) and another group with bacteriostatic normal saline (0.4 ml ip). Rats were killed 1, 2, 4, or 6 h after the treatment. Blood was collected R503 R504 TNF-a AND ENDOTOXEMIC MYOCARDIAL DEPRESSION Fig. 2. Temporal changes in circulating (s) and myocardial (k) TNF-a levels after administration of a sublethal dose of LPS. Rats were treated with LPS (0.5 mg/kg ip), and TNF-a in serum and ventricular myocardium was determined by ELISA 1 (n 5 8 rats), 2 (n 5 6 rats), 4 (n 5 6 rats), and 6 h (n 5 5 rats) after LPS treatment. Serum and myocardial TNF-a values of saline-treated rats were used as baseline (time 0, n 5 8). Both circulating and myocardial TNF-a increased at 1 and 2 h and returned to baseline level 4 h after LPS treatment. Data are means 6 SE. * P , 0.01 vs. saline control. RESULTS Influence of protein synthesis inhibition on TNF-a and myocardial depression. Because LPS-induced peak TNF-a level was at 1 h and maximal myocardial depression was at 6 h, the influences of interventions on these parameters were determined at these two time points after LPS treatment. CHX pretreatment attenuated the increase in serum TNF-a and abolished the Temporal relationship of increase in TNF-a with myocardial depression. The temporal changes in TNF-a levels are shown in Fig. 2. Because saline injection and time post saline injection do not appear to influence circulating and myocardial TNF-a levels, data from saline-treated rats were pooled and expressed as time 0. In saline-treated rats, TNF-a was barely detectable in the serum, whereas a low level of TNF-a was detected in the myocardium. After administration of LPS, serum and myocardial TNF-a increased primarily at 1 and 2 h. The peak serum TNF-a level (9.82 6 0.82 ng/ml, P , 0.01 vs. saline control) was observed at 1 h. Myocardial TNF-a level increased fivefold at 1 h (P , 0.01 vs. saline control). By 4 h after LPS treatment, TNF-a in both serum and myocardium had returned to baseline. The temporal changes in cardiac contractility are shown in Fig. 3. We observed previously that cardiac contractility was not influenced by saline injection and time after saline injection (18, 20). Thus contractility data from saline-treated rats were pooled. LVDP was 101 6 3.4 mmHg in hearts isolated from saline-treated rats. LVDP was not depressed at 2 h after administration of LPS. However, LVDP was significantly decreased at 4 and 6 h, with the maximal depression at 6 h (59.4 6 3.1 mmHg, P , 0.01 vs. saline control). Fig. 3. Temporal changes in cardiac contractile function after administration of a sublethal dose of LPS. Rats were treated with LPS (0.5 mg/kg ip), and left ventricular developed pressure (LVDP) was assessed by the Langendorff method 2, 4, and 6 h after administration of LPS. LVDP was attenuated at 4 and 6 h but not at 2 h after LPS treatment. Data are means 6 SE. * P , 0.01 vs. saline control. Downloaded from http://ajpregu.physiology.org/ by 10.220.33.3 on June 15, 2017 mouse TNF-a antibody (cross-reaction with rat TNF-a). Recombinant murine TNF-a was used to construct a standard curve. Absorbances of standards and samples were determined spectrophotometrically at 450 nm using a microplate reader (Bio-Rad Laboratories, Hercules, CA). Results were plotted against the linear portion of the standard curve. Isolated heart perfusion and assessment of contractile function. Intrinsic cardiac contractility was determined by a modified isovolumetric Langendorff technique as described elsewhere (18–20) and expressed as left ventricular developed pressure (LVDP). At the termination of the experiments, beating hearts were rapidly excised into oxygenated KrebsHenseleit solution containing (in mmol/l) 5.5 glucose, 1.2 CaCl2, 4.7 KCl, 25 NaHCO3, 119 NaCl, 1.17 MgSO4, and 1.18 KH2PO4. Normothermic retrograde perfusion was performed with the same solution in an isovolumetric and nonrecirculating mode. The perfusion buffer was saturated with a gas mixture of 92.5% O2-7.5% CO2 to achieve a PO2 of 450 mmHg, a PCO2 of 40 mmHg, and pH of 7.4. Perfusion pressure was maintained at 70 mmHg. A latex balloon was inserted through the left atrium into the left ventricle, and the balloon was filled with water to achieve a left ventricular end-diastolic pressure (LVEDP) of 5–10 mmHg (at peak and flat portion of LVEDP-LVDP curve). Pacing wires were fixed to the right atrium, and the heart was paced at 6.0 Hz. The myocardial temperature was maintained by placing the heart in a jacketed tissue chamber that was kept at 37°C by circulating warm water. LVDP and LVEDP were continuously recorded with a computerized pressure amplifier/digitizer (Maclab 8, AD Instrument, Cupertino, CA). Statistical analysis. Data were expressed as means 6 SE. An ANOVA and a Bonferroni-Dunn post hoc test were performed. Differences were accepted as significant with P , 0.05 verified by a Bonferroni-Dunn post hoc test. TNF-a AND ENDOTOXEMIC MYOCARDIAL DEPRESSION DISCUSSION In a rat model of endotoxemia not complicated with shock, the present study demonstrated that 1) myocardial depression was preceded by a transient increase in circulating and myocardial TNF-a level, and myocardial depression occurred after TNF-a level had normalized; 2) inhibition of the increase in circulating and myocardial TNF-a by protein synthesis blockade or immunosuppression abolished LPS-induced cardiac contractile dysfunction; and 3) neutralization of TNF-a with TNFBP also preserved cardiac contractile function. We conclude that TNF-a is a major but indirect myocardial depressant factor in this model of endotoxemia and that suppression of TNF-a production or neutralization of TNF-a preserves cardiac contractile function in this model of endotoxemia. LPS induces the synthesis and release of TNF-a by monocytes and macrophages and thereby increases circulating TNF-a level (40). LPS also induces TNF-a Table 1. Effects of protein synthesis inhibition and immunosuppression on TNF-a and myocardial depression Group Serum TNF-a Myocardial TNF-a LVDP Saline LPS CHX 1 LPS Dex 1 LPS CHX Dex 0.03 6 0.02 (8) 9.82 6 0.82* (8) 0.91 6 0.72† (6) 1.06 6 0.39† (7) 0.01 6 0.01 (2) 0.02 6 0.01 (2) 0.28 6 0.04 (8) 1.43 6 0.25* (8) 0.23 6 0.06† (6) 0.07 6 0.02† (7) 0.13 6 0.05 (2) 0.39 6 0.15 (2) 101.2 6 3.4 (14) 59.4 6 3.1* (14) 94.0 6 3.5† (6) 94.3 6 2.8† (6) 98.0 6 2.9 (2) 99.6 6 3.9 (2) Values are means 6 SE; n (no. of animals) in parentheses. LPS, lipopolysaccharide; CHX, cycloheximide; Dex, dexamethasone; TNF-a, tumor necrosis factor-a; LVDP, left ventricular developed pressure. * P , 0.01 vs. saline; † P , 0.01 vs. LPS. Fig. 4. Effects of TNFBP on LPS-induced myocardial depression. Rats were treated with TNFBP (40 or 80 µg/kg iv) immediately after administration of LPS (0.5 mg/kg ip). LVDP was assessed 6 h after administration of LPS. TNFBP at either dose applied prevented LPS-induced contractile dysfunction. Data are means 6 SE. * P , 0.01 vs. saline control. production by the myocardium (9, 19). In the present study, administration of a sublethal dose of LPS induced a transient increase in circulating and myocardial TNF-a. TNF-a levels in both serum and myocardium increased primarily at 1 and 2 h and returned to the baseline by 4 h. These temporal changes in circulating and myocardial TNF-a levels are consistent with previous reports characterizing the time course of circulating TNF-a of LPS-treated mice (40), rats (6, 7), rabbits (24), and humans (17, 38). Myocardial contractility was not depressed 2 h after administration of LPS when circulating and myocardial TNF-a levels remained elevated. Instead, myocardial contractility was depressed at 4 h, and maximal depression appeared at 6 h. Although TNF-a has been shown to induce immediate contractile depression in cardiac muscle preparations (5) or cardiac myocytes (25) in vitro, the temporal relationship of circulating and myocardial TNF-a levels and contractile depression observed in the present study indicates that endogenous TNF-a induces delayed cardiac dysfunction in endotoxemia. LPS increases circulating and tissue TNF-a through the activation of TNF-a gene transcription and ensuing synthesis of TNF-a peptides in monocytes, macrophages, and other cell types (9, 40). LPS-induced TNF-a gene transcription is regulated primarily by transcription factor nuclear factor (NF)-kB (13, 35). Two different approaches were applied in this study to suppress TNF-a production. Glucocorticoids may inhibit TNF-a gene transcription by regulation of NF-kB (2), and the protein synthesis blockade may inhibit the Downloaded from http://ajpregu.physiology.org/ by 10.220.33.3 on June 15, 2017 increase in myocardial TNF-a 1 h after administration of LPS (Table 1). CHX alone administered 4 h before sample collection did not influence either circulating or myocardial TNF-a levels. Pretreatment of rats with CHX also abolished cardiac contractile depression at 6 h after administration of LPS (Table 1), whereas treatment of rats with CHX alone did not affect cardiac contractility. Influence of immunosuppression on TNF-a and myocardial depression. Dex pretreatment suppressed the increase in serum TNF-a and abolished the increase in myocardial TNF-a (Table 1). Pretreatment of rats with Dex also prevented LPS-induced cardiac contractile depression (Table 1). However, treatment with Dex alone did not affect circulating and myocardial TNF-a levels, nor did this treatment influence cardiac contractility. Influence of TNFBP on myocardial depression. Treatment of rats with TNFBP at either dose abolished LPS-induced cardiac contractile depression (LVDP was 94.0 6 4.2 mmHg with 40 µg/kg TNFBP and 92.0 6 4.0 mmHg with 80 µg/kg TNFBP, both P , 0.01 vs. LPS alone and P . 0.05 vs. saline control; Fig. 4). Treatment of rats with TNFBP alone at the higher dose did not influence cardiac contractility (P . 0.05 vs. saline control). R505 R506 TNF-a AND ENDOTOXEMIC MYOCARDIAL DEPRESSION myocardial depressant factor in endotoxemia because myocardial contractility was depressed when the elevated TNF-a level was no longer present. TNF-a may depress cardiac contractility through the induction of a secondary factor or secondary factors. Indeed, TNF-a can induce the expression of inducible nitric oxide synthase in the myocardium (32), and myocardial depression associated with endotoxemic shock is accompanied by an enhanced nitric oxide synthase activity and an increased nitric oxide level (4, 33). However, nitric oxide may not be an important factor in this model of endotoxemic myocardial depression because nitric oxide synthase inhibitors failed to prevent or reverse the contractile dysfunction (18). The secondary factor or factors involved remain unknown. This unresolved issue will stimulate further research to determine the more distal factor or factors in endotoxemic myocardial depression. Perspectives TNF-a has been proposed to be an important cardiodepressant factor in septic shock (12). Exogenous TNF-a causes immediate myocardial depression in vitro (5) and delayed myocardial depression in vivo (22). It has long been recognized that endotoxemic myocardial dysfunction occurs late (8, 20, 28). The temporal relationship between endogenous TNF-a and myocardial depression is important to determine whether TNF-a is a direct or indirect factor in endotoxemic myocardial depression. Suppression of TNF-a production or neutralization of TNF-a may provide further information about the role of this cytokine in endotoxemic myocardial dysfunction. Using a rat endotoxemia model, this study demonstrated that increased circulating and myocardial TNF-a levels precede myocardial contractile dysfunction and that myocardial contractile dysfunction occurs after TNF-a levels have already normalized. Myocardial contractile dysfunction is abolished by inhibition of circulating and myocardial TNF-a. Neutralization of TNF-a with TNFBP also preserves myocardial contractile function. It appears that TNF-a is a major but indirect myocardial depressant factor in this model of endotoxemia. Further investigations using different endotoxemia models with insight into downstream factors may help to determine the role of TNF-a in myocardial depression related to trauma and sepsis and the molecular mechanisms of the action of TNF-a. The temporal discordance between TNF-a production and myocardial contractile dysfunction suggests that a therapeutic window may exist for the prevention of cardiac dysfunction, particularly in surgical cases of trauma or sepsis, through suppression of TNF-a production or neutralization of this cytokine. The authors are grateful to Drs. Charles A. Dinarello and Verlyn M. Peterson for constructive discussions. This work was supported in part by National Heart, Lung, and Blood Institute Grants HL-44186 and HL-43696 and National Institute of General Medical Sciences Grants GM-08315 and GM-49222. Address for reprint requests: X. Meng, Dept. of Surgery, Box C-320, Univ. of Colorado Health Sciences Center, 4200 East 9th Ave., Denver, CO 80262. Received 14 January 1998; accepted in final form 22 April 1998. Downloaded from http://ajpregu.physiology.org/ by 10.220.33.3 on June 15, 2017 synthesis of TNF-a peptides. Indeed, pretreatment with either Dex or CHX abolished the peak increase in myocardial TNF-a and greatly blunted the peak increase in circulating TNF-a in endotoxemic rats. As a result, pretreatment with either of these agents prevented the maximal myocardial depression at 6 h after administration of LPS. Thus inhibition of TNF-a production by immunosuppression or protein synthesis blockade preserves myocardial contractile function in endotoxemic rats. It should be noted, however, that circulating TNF-a remained slightly elevated after immunosuppression or protein synthesis inhibition whereas the increase in myocardial TNF-a was completely abolished. It is possible that the elevated level of myocardial TNF-a is the primary contributor to contractile depression. Although the sources of circulating TNF-a may be less sensitive to inhibition than those of myocardial TNF-a, a low level of circulating TNF-a alone is not sufficient to depress myocardial contractility. TNFBP functions to bind free TNF-a and thereby attenuates TNF-a cytotoxicity in vitro and in vivo (38). The form of TNFBP used in this study has been shown to abolish TNF-a cytotoxicity to 1591-RE 3.5 cells and the negative inotropic properties of TNF-a in cultured cardiac myocytes (10). To further examine the role of TNF-a in this model of endotoxemic myocardial depression, TNFBP, at two doses comparable to that used previously in vitro (10), was applied to rats immediately after administration of LPS. The maximal myocardial depression was abolished by TNFBP at either dose. Taken together, the results of this study indicate that endogenous TNF-a may be a major factor mediating the delayed myocardial depression in this model of endotoxemia. Our findings appear to differ from the report by Nishikawa and colleagues (24), which demonstrated that pretreatment with antiserum against TNF-a does not prevent cardiac dysfunction in a rabbit endotoxemic shock model. The disparate findings may be due to the use of different animal models and the exact TNF-neutralizing agents used in these two separate studies. In the present study, TNFBP was applied to a rat model of endotoxemia without shock whereas the study by Nishikawa and colleagues (24) examined the influence of antiserum against TNF-a on a rabbit endotoxemic shock model. Perhaps TNFBP is more effective than antiserum in preventing endotoxemic cardiac contractile dysfunction. It is also possible that some confounding factors are present in a shock model but not in a nonshock model. Furthermore, the difference in the timing of TNF-neutralizing agent administration may account for the difference between our findings and the previous study. In the present study, TNFBP was administered immediately after injection of LPS while antiserum against TNF-a was administered 1 h before injection of LPS in the study by Nishikawa and colleagues (24). TNF-a may exert its immediate negative inotropic effect on myocardium by activation of the neutral sphingomyelinase (25) or the constitutive nitric oxide synthase (5). However, TNF-a is unlikely to be a direct TNF-a AND ENDOTOXEMIC MYOCARDIAL DEPRESSION REFERENCES 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. cardiac contractile dysfunction in a rat model of endotoxemia without shock. Shock 7: 111–118, 1997. Meng, X., L. Ao, J. M. Brown, D. R. Meldrum, B. C. Sheridan, B. S. Cain, A. Banerjee, and A. H. Harken. LPS induces late cardiac functional protection against ischemia independent of cardiac and circulating TNF-a. Am. J. Physiol. 273 (Heart Circ. Physiol. 42): H1894–H1902, 1997. Meng, X., J. M. Brown, L. Ao, S. K. Nordeen, W. Franklin, A. H. Harken, and A. Banerjee. Endotoxin induces cardiac heat shock protein 70 and resistance to endotoxemic myocardial dysfunction. Am. J. Physiol. 271 (Cell Physiol. 40): C1316– C1324, 1996. Mohler, K. M., D. S. Torrance, C. A. Smith, R. G. Goodwin, K. E. Stremler, V. P. Fung, H. Madani, and M. B. Widmer. Soluble tumor necrosis factor (TNF) receptors are effective therapeutic agents in lethal endotoxemia and function simultaneously as both TNF carriers and TNF antagonists. J. Immunol. 151: 1548–1561, 1993. Murray, D. R., and G. L. Freeman. Tumor necrosis factoralpha induces a biphasic effect on myocardial contractility in conscious dogs. Circ. Res. 78: 154–160, 1995. Natanson, C., P. W. Eichenholz, R. L. Danner, P. Q. Eichacker, W. D. Hoffman, G. C. Kuo, S. M. Banks, T. J. MacVittie, and J. E. Parrillo. Endotoxin and tumor necrosis factor challenge in dogs simulate the cardiovascular profile of human septic shock. J. Exp. Med. 169: 823–832, 1989. Nishikawa, Y., J. Mathison, and W. Y. W. Lew. Serum tumor necrosis factor-a does not mediate endotoxin-induced myocardial depression in rabbits. Am. J. Physiol. 270 (Heart Circ. Physiol. 39): H485–H491, 1996. Oral, H., G. W. Dorn, and D. L. Mann. Sphingosine mediates the immediate negative inotropic effects of tumor necrosis factor-a in the adult mammalian cardiac myocyte. J. Biol. Chem. 272: 4836–4842, 1997. Pagani, F. D., L. S. Baker, C. Hsi, M. Knox, M. P. Fink, and M. S. Visner. Left ventricular systolic and diastolic dysfunction after infusion of tumor necrosis factor-a in conscious dogs. J. Clin. Invest. 90: 389–398, 1992. Papadakis, E. J., and F. L. Abel. Left ventricular performance in canine endotoxin shock. Circ. Shock 24: 123–131, 1988. Parker, J. L., H. R. Adams. Development of myocardial dysfunction in endotoxin shock. Am. J. Physiol. 248 (Heart Circ. Physiol. 17): H818–H826, 1985. Parker, M. M., J. H. Shelhammer, S. L. Bacharach, M. V. Green, C. Natanson, T. M. Frederick, B. A. Damske, and J. E. Parrillo. Profound but reversible myocardial depression in patients with septic shock. Ann. Intern. Med. 100: 483–490, 1984. Parrillo, J. E., C. Burch, J. H. Shelhammer, M. M. Parker, C. Natanson, and W. Schuette. A circulating myocardial depressant substance in humans with septic shock. Septic shock patients with a reduced ejection fraction have a circulating factor that depresses in vitro myocardial performance. J. Clin. Invest. 76: 1539–1553, 1985. Rothblum, L., T. Devlin, and J. J. Chin. Regulation of mammalian protein synthesis in vivo. Protein synthesis in the rat liver and kidney after the administration of small sublethal doses of cycloheximide. Biochem. J. 156: 151–157, 1976. Schulz, R., E. Nava, and S. Moncada. Induction and potential biological relevance of a Ca21 independent nitric oxide synthase in the myocardium. Br. J. Pharmacol. 105: 575–580, 1992. Schulz, R., D. L. Panas, R. Catena, S. Moncada, P. M. Olley, and G. D. Lopaschuk. The role of nitric oxide in cardiac depression induced by interleukin-1b and tumor necrosis factor-a. Br. J. Pharmacol. 114: 27–34, 1995. Suffredini, A. F., R. E. Fromm, M. M. Parker, K. Brenner, J. A. Kovacs, R. A. Wesley, and J. E. Parrillo. The cardiovascular response of normal humans to the administration of endotoxin. N. Engl. J. Med. 321: 280–287, 1989. Sweet, M. J., and D. A. Hume. Endotoxin signal transduction in macrophages. J. Leukoc. Biol. 60: 8–26, 1996. Tracey, K. J., B. Beutler, S. F. Lowry, J. Merryweather, S. Wolpe, I. W. Milsark, R. J. Hariri, T. J. Fahey, A. Zentella, Downloaded from http://ajpregu.physiology.org/ by 10.220.33.3 on June 15, 2017 1. Ashkenazi, A., S. A. Marsters, D. J. Capon, S. M. Chamow, I. S. Figari, D. Pennica, D. V. Goeddel, M. A. Palladino, and D. H. Smith. Protection against endotoxic shock by a tumor necrosis factor receptor immunoadhesin. Proc. Natl. Acad. Sci. USA 88: 10535–10539, 1991. 2. Auphan, N., J. A. DiDonato, C. Rosette, A. Helmberg, and M. Karin. Immunosuppression by glucocorticoids: inhibition of NFkB activity through induction of IkB synthesis. Science 270: 286–290, 1995. 3. Beutler, B., I. W. Milsark, and A. C. Cerami. Passive immunization against cachectin/tumor necrosis factor protects mice from lethal effects of endotoxin. Science 229: 869–871, 1985. 4. Brady, A. J. B., P. A. Poole-Wilson, S. E. Harding, and J. B. Warren. Nitric oxide production within cardiac myocytes reduces their contractility in endotoxemia. Am. J. Physiol. 263 (Heart Circ. Physiol. 32): H1963–H1966, 1992. 5. Finkel, M. S., C. V. Oddis, T. D. Jacob, S. C. Watkins, B. G. Hattler, and R. L. Simmons. Negative inotropic effects of cytokines on the heart mediated by nitric oxide. Science 257: 387–389, 1992. 6. Fukata, O. B., N. Murakami, H. Kobayashi, H. Segawa, S. Muro, I. Hanaoka, Y. Naito, Y. Masui, Y. Ohmoto, H. Imura, and K. Nakao. Effects of IL-1 receptor antagonist and antiserum to TNF-a on LPS-induced plasma ACTH and corticosterone rise in rats. Am. J. Physiol. 266 (Endocrinol. Metab. 29): E986– E992, 1994. 7. Givalois, L., J. Dornand, M. Mekaouche, M. D. Solier, A. F. Bristow, G. Ixart, P. S. I. Assenmacher, and G. Barbanel. Temporal cascade of plasma level surges in ACTH, corticosterone, and cytokines in endotoxin-challenged rats. Am. J. Physiol. 266 (Regulatory Integrative Comp. Physiol. 35): R164–R170, 1994. 8. Hung, J., and W. Y. W. Lew. Temporal sequence of endotoxininduced systolic and diastolic myocardial depression in rabbits. Am. J. Physiol. 265 (Heart Circ. Physiol. 34): H810–H819, 1993. 9. Kapadia, S., J. Lee, G. Torre-Amione, H. H. Birdsall, T. S. Ma, and D. L. Mann. Tumor necrosis factor-a gene and protein expression in adult feline myocardium after endotoxin administration. J. Clin. Invest. 96: 1042–1052, 1995. 10. Kapadia, S., G. Torre-Amione, T. Yokahama, and D. L. Mann. Soluble TNF binding proteins modulate the negative inotropic properties of TNF-a in vitro. Am. J. Physiol. 268 (Heart Circ. Physiol. 37): H517–H525, 1995. 11. Keller, R. S., J. J. Jones, K. F. Kim, P. R. Myers, H. R. Adams, J. L. Parker, and L. Rubin. Endotoxin-induced myocardial dysfunction: is there a role for nitric oxide? Shock 4: 338–344, 1995. 12. Kumar, A., V. Thota, L. Dee, J. Olson, E. Uretz, and J. E. Parrillo. Tumor necrosis factor-alpha and interleukin 1-beta are responsible for the in vitro myocardial cell depression induced by human septic shock serum. J. Exp. Med. 183: 949–958, 1996. 13. Kuprash, D. V., I. A. Udalova, R. L. Turetskaya, N. R. Rice, and S. A. Nedospasov. Conserved kB element located downstream of the tumor necrosis factor a gene: distinct NF-kB binding pattern and enhancer activity in LPS activated murine macrophages. Oncogene 11: 97–106, 1995. 14. Lefer, A. M. Role of a myocardial depressant factor in the pathogenesis of circulatory shock. Federation Proc. 29: 1836– 1847, 1970. 15. Lefer, A. M., and M. J. Rovetto. Influence of a myocardial depressant factor on physiologic properties of cardiac muscle. Proc. Soc. Exp. Biol. Med. 134: 269–273, 1970. 16. Lesslauer, W., H. Tabuchi, R. Gentz, M. Brockhaus, E. J. Schlaeger, G. Grau, P. F. Piguet, P. Pointaire, P. Vassali, and H. Loetscher. Recombinant soluble tumor necrosis factor receptor proteins protect mice from lipopolysaccharide-induced lethality. Eur. J. Immunol. 21: 2883–2886, 1991. 17. Mackensen, A., C. Galanos, and R. Engelhardt. Treatment of cancer patients with endotoxin induces release of endogenous cytokines. Pathobiology 59: 264–267, 1991. 18. Meng, X., L. Ao, J. M. Brown, D. A. Fullerton, A. Banerjee, and A. H. Harken. Nitric oxide synthase is not involved in R507 R508 TNF-a AND ENDOTOXEMIC MYOCARDIAL DEPRESSION J. D. Albert, G. T. Shires, and A. Cerami. Shock and tissue injury induced by recombinant human cachectin. Science 234: 470–474, 1986. 37. Tracey, K. J., Y. Fong, D. G. Hesse, K. R. Manogue, A. T. Lee, G. C. Kuo, S. F. Lowry, and A. Cerami. Anti-cachectin/TNF monoclonal antibodies prevent septic shock during lethal bacteremia. Nature 330: 662–664, 1987. 38. Van Zee, K. J., T. Kohno, E. Fischer, C. S. Rock, L. L. Moldawer, and S. F. Lowry. Tumor necrosis factor soluble receptors circulate during experimental and clinical inflammation and can protect against excessive tumor necrosis factor- alpha in vivo and in vitro. Proc. Natl. Acad. Sci. USA 89: 4845–4849, 1992. 39. Yokoyama, T., L. Vaca, R. D. Rossen, W. Durante, P. Hazarika, and D. L. Mann. Cellular basis for the negative inotropic effects of tumor necrosis factor-a in the adult mammalian cardiac myocyte. J. Clin. Invest. 92: 2303–2312, 1993. 40. Zuckerman, S. H., J. Shellhaas, and L. D. Butler. Differential regulation of lipopolysaccharide-induced interleukin-1 and tumor necrosis factor synthesis: effects of endogenous and exogenous glucocorticoids and the role of the pituitary-adrenal axis. Eur. J. Immunol. 19: 301–305, 1989. Downloaded from http://ajpregu.physiology.org/ by 10.220.33.3 on June 15, 2017