Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
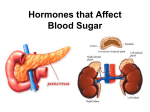
• Chapter 19 The Peripheral Endocrine Glands Peripheral Endocrine Glands • Thyroid gland controls basal metabolic rate. • Adrenal glands maintain salt balance, involved in nutrient metabolism and stress adaptation. • Endocrine pancreas important in nutrient metabolism and glucose homeostasis. • Parathyroid glands important in Ca2+ metabolism. Thyroid Gland • Contains two types of endocrine secretory cells: • • follicular cells produce tetraiodothyronine (T4 or thyroxine) and tri-iodothyronine (T3) C cells produce Ca2+-regulating hormone calcitonin. Thyroid Hormone Synthesis • Basic ingredients: • amino acid tyrosine synthesized in sufficient amounts by body • iodine obtained from dietary intake • Thyroid hormone is synthesized and stored on the thyroglobulin molecule. • • Thyroid hormones remain in colloid until they are split off and secreted. Usually enough thyroid hormone stored to supply body’s needs for several months. Thyroid follicular cell Blood Colloid Golgi complex Endoplasmic reticulum 2 Na+ 9b MIT DIT 8 MIT DIT 4b Tg MIT 5a 3 Na+ (Iodinase action) Lysosome K+ K+ Tg 4a 1 4 MIT DIT 7 I– 6a 1 MIT + 1 DIT 5b DIT 6b 2 DITs 9a Thyroid follicle Tyrosine-containing thyroglobulin is exported from follicular cells into colloid by exocytosis. – – Iodine from blood pumped into colloid. Within colloid iodine attaches to tyrosine. Process forms MIT and DIT. Coupling of MIT and DIT forms thyroid hormones. MIT coupled to DIT produces T3 DIT coupled to DIT produces T4 Fig. 19-2, p. 688 Stress Cold in infants • Regulated negative-feedback between hypothalamic TRH, anterior pituitary TSH, and thyroid gland T3 and T4. • Main determinant of basal metabolic rate. Influences synthesis and degradation of carbohydrate, fat, and protein. Increases responsiveness to catecholamines. Increases heart rate and force of contraction. Essential for normal growth. Plays crucial role in normal development of nervous system. Hypothalamus Thyrotropin-releasing hormone (TRH) • Anterior pituitary • Thyroid-stimulating hormone (TSH) Thyroid gland • • • Thyroid hormone (T3 and T4) Metabolic rate and heat production; enhancement of growth and CNS development; enhancement of sympathetic activity Fig. 19-3, p. 689 Hypothyroidism • Causes: • • • • • primary due to failure of thyroid gland secondary due to deficiency of TRH, TSH inadequate dietary supply of iodine Treatment: • taking replacement thyroid hormone • providing dietary iodine for deficiency Symptoms: – reduced BMR, poor cold tolerance, excessive weight gain, fatigue, decreased cardiac output, slow reflexes and slow mental responsiveness – myxedema from accumulation of water-retaining carbohydrate molecules – in infants causes cretinism characterized by dwarfism and mental retardation Hyperthyroidism Causes: • • • Grave’s Disease when body produces thyroid-stimulating immunoglobulins (TSI) secondary to excess TRH or TSH Treatment: • removal of over-secreting thyroid lobes • administration of radioactive iodine • use of antithyroid drugs Symptoms: – increased BMR, poor heat tolerance, excessive weight loss, skeletal muscle loss, increased cardiac output, excessive degree of mental alertness leading to agitation/anxiousness – Exophthalmos (bulging) eyes – Goiter: enlarged thyroid gland develops when the thyroid gland is overstimulated Adrenal Glands • • Located above each kidney Composed of two endocrine organs: – • adrenal cortex • outer portion • secretes steroid hormones – adrenal medulla • inner portion secretes catecholamines Consists of three layers: • • • • zona glomerulosa, outer layer zona fasciculata, middle layer zona reticularis, inner layer Secretes hormones called “corticoids” • • • mineralocorticoids glucocorticoids sex hormones Capsule Zona glomerulosa Zona fasciculata Adrenal medulla Adrenal cortex Adrenal Mineralocorticoids gland (aldosterone) Glucocorticoids (cortisol) and sex hormones (dehydroepiandrosterone) Catecholamines (epinephrine and norepinephrine) (a) Location and gross structure of adrenal glands Cortex Zona reticularis Medulla Connective tissue capsule Zona glomerulosa Zona fasciculata Cortex Zona reticularis Medulla (b) Layers of adrenal cortex Fig. 19-7, p. 693 Cholesterol Pregnenolone 17-Hydroxypregnenolone Progesterone 17-Hydroxyprogesterone Dehydroepiandrosterone (adrenal cortex hormone) Androstenedione Estrone Testosterone Estradiol (female sex hormone) 11-Deoxycorticosterone Deoxycortisol Androgens (male sex hormones) Corticosterone Cortisol Aldosterone Glucocorticoid (adrenal cortex hormone) Estriol Estrogens (female sex hormones) Mineralocorticoid adrenal cortex hormone) Fig. 19-8, p. 694 Adrenal Cortex • Glucocorticoids: – – – – – – • produced primarily in zona fasciculata major hormone is cortisol plays role in nutrient metabolism increase levels of blood glucose by gluconeogenesis involved in stress resistance exerts antiinflammatory and immunosuppressive effects Mineralocorticoids: • • • • • • produced by zona glomerulosa primarily aldosterone increase Na+ reabsorption and K+ secretion help maintain blood pressure homeostasis mineralocorticoids are essential for life Sex hormones: • • • • • produced in inner two layers similar to testosterone no effects in males most important is dehydroepiandosterone (DHEA) regulates sex drive and growth of axillary and pubertal hair in females Stress Diurnal rhythm Hypothalamus Corticotropin-releasing hormone (CRH) Anterior pituitary Adrenocorticotropic hormone (ACTH) Adrenal cortex Cortisol Metabolic fuels and building blocks available to help resist stress Blood glucose (by stimulating gluconeogenesis and inhibiting glucose uptake) Blood amino acids (by stimulating protein degradation) Blood fatty acids (by stimulating lipolysis) Fig. 19-9, p. 696 Cortisol Hyper/hyposecretion • • Cushing’s syndrome Causes: • • • overstimulation of adrenal cortex adrenal tumors secrete excess cortisol Signs and symptoms: • • hyperglycemia and glucosuria (adrenal diabetes) abnormal fat distributions “buffalo hump” and “moon face” Primary adrenocortical insufficiency known as Addison’s disease: –all three layers under-produce hormones –changes in blood pressure, nutrient metabolism Adrenal Medulla • • • Contains modified sympathetic postganglionic neurons. Primary stimulus for secretion is sympathetic nervous system. Releases epinephrine and norepinephrine: • • • Epinephrine 80% Norepinephrine 20% of secretion Epinephrine: • • • reinforces sympathetic system in mounting general systemic “fightor-flight” responses maintenance of arterial blood pressure increases blood glucose and blood fatty acids Endocrine Control of Fuel Metabolism • Metabolism • all the chemical reactions that occur within the cells of the body • Intermediary metabolism or fuel metabolism • includes reactions involving degradation, synthesis, and transformation of proteins, carbohydrates, and fats Tissues in Metabolism • Liver: • • primary role in maintaining normal blood glucose levels principal site for metabolic interconversions • Adipose tissue: • • primary energy storage site important in regulating blood fatty acid levels • Muscle: • • primary site of amino acid storage major energy user • Brain: • • • normally uses only glucose for energy does not store glycogen blood glucose levels must be maintained to supply energy source to brain Food intake Dietary carbohydrate Dietary protein D Absorbable units Amino acids E S T Glucose A = Anabolism = Catabolism I G Storage, structural, and functional macromolecules in cells Body proteins (structural or secretory products) Glycogen storage in liver and muscle Triglycerides in adipose tissue stores (fat) B S O R Dietary triglyceride fat I O N Fatty acids Monoglycerides P Metabolic pool in body T I O N Urea Urinary excretion (elimination from body) Amino acids Glucose Use as metabolic fuel in cells: Oxidation to CO2+H2O+ATP (energy) Fatty acids Expired (elimination from body) F Table 19-3 p704 Stressor Stress is generalized nonspecifc response of the body to any factor that overwhelms, or threatens to overwhelm, the body’s compensatory ability to maintain homeostasis. Stressor is any stimulus that causes stress response. All actions coordinated by the hypothalamus. Hypothalamus CRH Sympathetic nervous system Posterior Pituitary Anterior pituitary Vasopressin ACTH Conserve salt and H2O to expand the plasma volume; help sustain blood pressure when acute loss of plasma volume occurs Vasopressin and angiotensin II cause arteriolar vasoconstriction to increase blood pressure Adrenal cortex Adrenal medulla Epinephrine Cortisol Prepare body for “fight or flight” Arteriolar smooth muscle Mobilize energy stores and metabolic building blocks for use as needed Glucagon-secreting cells Insulin-secreting cells Endocrine pancreas Vasoconstriction Blood flow through kidneys Glucagon Renin Angiotensin Aldosterone Insulin Fig. 1 Table 19-2 p702 Factors that increase blood glucose Factors that decrease blood glucose Transport of glucose into cells: ––For utilization for energy production ––For storage • as glycogen through glycogenesis • as triglycerides Glucose absorption from digestive tract Blood glucose Hepatic glucose production: ––Through glycogenolysis of stored glycogen ––Through gluconeogenesis Urinary excretion of glucose (occurs only abnormally, when blood glucose level becomes so high it exceeds the reabsorptive capacity of kidney tubules during urine formation) KEY = Factors subject to hormonal control to maintain blood glucose level Fig. 19-16, p. 710 Insulin and glucagon Insulin Anabolic hormone • Lowers blood concentration of glucose, fatty acids, and amino acids by promoting cellular uptake. • Enhances their conversion into glycogen, triglycerides, and proteins. • Secretion is increased during absorptive state. • Primary stimulus for secretion is increase in blood glucose concentration. Glucagon • Catabolic hormone • Secreted during postabsorptive state in response to a fall in blood glucose. • Mobilizes energy-rich molecules from their stores. • Increases blood glucose levels. • In general opposes the actions of insulin. Gastrointestinal hormones (incretins) Blood amino acid concentration Blood amino acid concentration Major control Food intake Parasympathetic stimulation Islet cells Sympathetic stimulation (and epinephrine) Insulin secretion Blood glucose Blood fatty acids Blood amino acids Protein synthesis Fuel storage Fig. 19-18, p. 713 Diabetes Mellitus • Most common of all endocrine disorders. • Results in elevated blood glucose levels. • Two major types: • type I diabetes characterized by lack of insulin secretion. • type II diabetes characterized by reduced sensitivity of insulin’s target cells. Endocrine Control of Calcium Metabolism • Plasma Ca2+ must be closely regulated to prevent changes in neuromuscular excitability. • Role in other essential activities: • • • • excitation-contraction coupling in cardiac and smooth muscle stimulus-secretion coupling maintenance of tight junctions clotting of blood • Three hormones regulate plasma concentration of Ca2+ (and PO43-) • • • parathyroid hormone (PTH) calcitonin vitamin D PTH/Vitamin D/Calcitonin PTH • • • Vitamin D Secreted by parathyroid • glands. Primary regulator of Ca2+ • Actions: • promotes Ca2+ movement from bone fluid into the • plasma • enhances Ca2+ reabsorption by • kidneys • facilitates activation of vitamin D Stimulates Ca2+ and PO43absorption from intestine. Calcitonin • Produced by the C cells of the thyroid gland. • Secreted in response to Can be synthesized from an increase in plasma cholesterol derivative Ca2+ when exposed to sunlight. • Lowers plasma Ca2+ by inhibiting activity of Supplemented by dietary bone osteoclasts. intake. • Calcitonin is Must be activated first by unimportant except liver and then by kidneys during the rare before it can affect the condition of intestines. hypercalcemia. Plasma Ca2+ Plasma Ca2+ Parathyroid glands Thyroid C cells PTH Plasma Ca2+ Calcitonin Plasma Ca2+ Fig. 19-26, p. 729 Precursor in skin (7-dehydrocholesterol) Dietary vitamin D Sunlight Vitamin D3 Hydroxyl group (OH) Liver enzymes 25-OH-vitamin D3 Hydroxyl group PTH Plasma Ca2+ Kidney enzymes Plasma PO43− 1,25-(OH)2-vitamin D3 (active vitamin D) Promotes intestinal absorption of Ca2+ and PO43− Fig. 19-27, p. 730