Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Aortic stenosis wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Echocardiography wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
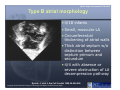
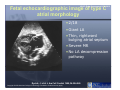
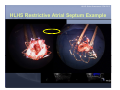
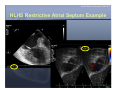
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children SCAI Fall Fellows Course 2012 Las Vegas HLHS: Echo Assessment SCAI 2012 Disclosure Information HLHS: Echocardiographic Assessment Craig E Fleishman MD, FACC, FASE As a faculty member for this program, I disclose the following relationships with industry: (GRS): Grant/Research Support (C): Consultant (SB): Speaker’s Bureau (MSH): Major Stock Holder (AB): Advisory Board (E): Employment (O):Other Financial or Material Support W.L. Gore Medical: C, Echo Core Lab HLHS: Echo Assessment SCAI 2012 HLHS HLHS: Echo Assessment SCAI 2012 HLHS •Spectrum of Malformations – 7-9% CHD diagnosed in infancy •Underdevelopment of left heart – Left atrium – Mitral Valve – Left Ventricle – Aortic Valve – Aortic Arch HLHS: Echo Assessment SCAI 2012 Left Atrium – Hypoplastic – Thick walled – Variable size of ASD • Some restriction helpful • Intact atrial septum – Look for levoatrial cardinal vein – Malalignment of atrial septum • Leftward and posterior attachment to LA free wall • Small, superior, posterior PFO HLHS: Echo Assessment SCAI 2012 Mitral Valve • Stenotic, hypoplastic, or atretic – MV annulus diameter ≤ 6 mm • May not have well defined chordae (arcade) • Papillary muscles – Closely spaced – Parachute HLHS: Echo Assessment SCAI 2012 LV • Variable hypoplasia – Does not extend to cardiac apex – LV area < 1.5 cm2 (PLAX) – Smallest with MA/AA – Larger with VSD • Hypertrophy • Echo bright areas reflect endocardial changes – Endocardial fibroelastosis HLHS: Echo Assessment SCAI 2012 Aortic Valve and Aorta • Aortic atresia (plate) or dysplastic – Larger with VSD • Hypoplastic ascending aorta – <5 mm, usually smaller – Main coronary artery – Fills retrograde from ductus arteriosus • Aorta becomes larger at 1st arch vessel, but not normal until distal to PDA • Aortic arch branching pattern • Juxtaductal posterior shelf/coarctation HLHS: Echo Assessment SCAI 2012 PDA • PDA usually large, with aorta inserting onto ductal arch • Right to left flow in systole • Left to right in diastole – Diastolic flow reversal in abdominal Ao – L to R decreased with Pulm HTN • PPHTN • Intact atrial septum HLHS: Echo Assessment SCAI 2012 Coronary Arteries •Anomalous origins are rare •Abnormalities more common with MS/AA – Single coronary – Tortuosity – Sinusoids between coronaries and LV •? left ventricular dependent coronary circulation HLHS: Echo Assessment SCAI 2012 Other areas of interest •Pulmonary stenosis or regurgitation •Right ventricular function •Tricuspid regurgitation •Left SVC •Abnormal pulmonary venous connections (6%) HLHS: Echo Assessment SCAI 2012 HLHS Intact Atrial Septum •18/316 infants over 6.5 yr period •Atrial septal morphology evaluated •Lung histopathology reviewed HLHS: Echo Assessment SCAI 2012 Type A atrial morphology • 12/18 infants • Relatively large LA • Thick septum secundum • Thin septum primum • 5/12 with leftward and posterior deviated atrial septum • All had LA decompression pathway, 3 severely obstructed Rychik, J. et al. J Am Coll Cardiol 1999;34:554-560 Copyright ©1999 American College of Cardiology Foundation. Restrictions may apply. HLHS: Echo Assessment SCAI 2012 Type B atrial morphology • 4/18 infants • Small, muscular LA • Circumferential thickening of atrial walls • Thick atrial septum w/o distinction between septum primum and secundum • 4/4 with absence or severe obstruction of LA decompression pathway Rychik, J. et al. J Am Coll Cardiol 1999;34:554-560 Copyright ©1999 American College of Cardiology Foundation. Restrictions may apply. HLHS: Echo Assessment SCAI 2012 Fetal echocardiographic image of type C atrial morphology • 2/18 • Giant LA • Thin, rightward bulging atrial septum • Severe MR • No LA decompression pathway Rychik, J. et al. J Am Coll Cardiol 1999;34:554-560 Copyright ©1999 American College of Cardiology Foundation. Restrictions may apply. HLHS: Echo Assessment SCAI 2012 HLHS Intact Atrial Septum •17/18 stage I Norwood •6/17 Early survivors – Type A atrial morphology – Unobstructed decompression pathway •3 additional late deaths after CPB •Lung pathology – Severely dilated lymphatics – Arterialization of the pulmonary veins Rychik, J. et al. J Am Coll Cardiol 1999;34:554-560 HLHS: Echo Assessment SCAI 2012 HLHS Intact Atrial Septum Example HLHS: Echo Assessment SCAI 2012 HLHS Restrictive Atrial Septum Example HLHS: Echo Assessment SCAI 2012 Time Passes •Stage I with atrial septectomy #1 – Aortic arch stent via carotid cutdown – ASD stent #1 for increased restriction •Bidirectional Glenn with atrial septectomy #2 – PA stent – ASD stent #2 for increased restriction •Presents at 20 months of age with worse cyanosis HLHS: Echo Assessment SCAI 2012 HLHS Restrictive Atrial Septum Example HLHS: Echo Assessment SCAI 2012 HLHS Restrictive Atrial Septum Example HLHS: Echo Assessment SCAI 2012 Pre-Hybrid Screening HLHS: Echo Assessment SCAI 2012 PFO/ASD HLHS: Echo Assessment SCAI 2012 HLHS Pre-Hybrid Screening • Follow path from PDA to ascending aorta – Lack of alignment can signal twisting • Retrograde flow obstruction despite unobstructed PDA can be worsened with PDA stent • Potential areas for stenoses HLHS: Echo Assessment SCAI 2012 HLHS Pre-Hybrid Screening HLHS: Echo Assessment SCAI 2012 Pre-Hybrid Screening • Stenosis at isthmus and at ascending aorta/transverse arch transition • Treated with traditional Stage I – Anatomy confirmed at surgery HLHS: Echo Assessment SCAI 2012 Pre-Hybrid Screening • Transverse arch and ascending aorta adequate • Obstruction at distal arch despite PGE and unobstructed PDA – Confirmed by color flow and CW Doppler HLHS: Echo Assessment SCAI 2012 Thank You HLHS: Echo Assessment SCAI 2012 HLHS: Echo Assessment SCAI 2012