Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
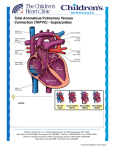
EDITORIALS are normal inhabitants. Yet, in this issue (see page 358) and the July issue5 three potentially lethal reactions were reported because of penicillin. These life-threatening reactions could not have been predicted with the use of any available pharmacologic data. However, each patient had a distinct susceptibility for a serious reaction. The reasons for the heightened susceptibility were different. In two patients there was an unusual state of immunologic reactivity. Could this have been predicted? Another patient was debilitated and had organic heart disease and was therefore susceptible to the potassium administered with the penicillin. Could this have been predicted? The answer to these questions is probably no. The magnitude of such problems, however, mandates that the question be asked repeatedly. In order to decrease the incidence of adverse drug reactions physicians must not only have intimate knowledge of drugs, but they must also have intimate knowledge of the patients in whom they are to be used. Bernurd H. Booth, M . D . Jackson,Mississippi 1 Haddinet BC, Gowdy CW, Coulter WK, et al: Drug reactions and errors in administration on a medical ward. Canad Med Ass J 97: 1450-1457, 1967 2 Honvitz N: Admissions to hospital due to drugs. Br Med J 1 :539-540, 1969 3 Seidl LC, Thornton CF, Smith JW, et al: Studies on the epidemiology of adverse drug reactions. 111. Reactions in patients on a general medical senice. Bull Hopkins Hosp 111 :299-315, 1966 4 United States Department of Health, Education and Welfare, Task Force on Prescription Drugs: Final report. Washington, D.C. Government Printing Office, 1969 5 Petsas A, Kotler MN: Electrocardiographic changes associated with penicillin anaphylaxis. Chest 64:66-69, 1W3 Obstruction to Pulmonary Venous Return Obscured by Decreased Pulmonary Blood Flow I n this issue of Chest, Muster et a1 describe two small infants with the rare combination of tetralogy of Fallot and total anomalous pulmonary venous drainage. Both patients died when surgery for increased pulmonary blood flow as palliation for the tetralogy resulted in worsening of the previously unsuspected pulmonary obstruction associated with the anomalous veins. Obstruction to pulmonary venous return ( e g , total anomalous pulmonary venous drainage, mitral stenosis and atresia, cor triatriatum) may be especially difficult to diagnose in the presence of another defect which includes pulmonic stenosis. When pulmonary blood flow is de- creased, the clinical signs of pulmonary venous obstruction may be absent, and pulmonary venous pressure may not be unduly elevated. After a systemic pulmonary-arterial shunt is established surgically, the obstruction is exaggerated and pulmonary venous pressure rises precipitously, resulting in pulmonary edema with all of its manifestations. Unfortunately, congestive heart failure is relatively common following aortic-pulmonary arterial shunts established during infancy, even in uncomplicated situations. Thus, when pulmonary congestion occurs after operation, additional undetected pulmonary venous obstruction will often not be immediately suspected. The possibility of an additional left-sided obstructive lesion, however, adds justification to the principle that patients with congestive heart failure after operation should have repeat cardiac catheterization promptly, especially if response to medical therapy is marginal. If, as in most instances, the shunt is simply too large, surgical modification of the anastomosis can be carried out as necessary. On the other hand, when an associated pulmonary venous obstructive lesion is found to be present, palliation or surgical repair of the additional defect is in order. Recently, at this institution, a patient with ventricular septa1 defect and pulmonary atresia developed pulmonary edema following a Waterston shunt. A second cardiac catheterization revealed that the mean .left atrial pressure had risen from 4 to 35 mm Hg, secondary to increased pulmonary blood flow, previously unrecognized mitral atresia, and a small patent foramen ovale. Balloon septostomy produced an excellent palliative result. Cardiac catheterization and angiography in infancy are carried out at low risk in experienced laboratories. A seriously ill baby with previously unrecognized congenital heart disease must always be studied without unnecessary delay. Similarly, as mentioned by Muster, specific hemodynamic data also must be promptly obtained in the infant whose clhical course has been poor after opration. In the modem era of the aggressive approach to the diagnosis of congenital heart disease in infancy, unusual combinations of defects may be recognized during life rather than in the pathology laboratory. Only when complete hemodynamic information is available, can rational management be instituted and a successful outcome achieved. Welton M . Gersony, M . D . * New York, N.Y. --- *Director, Division of Pediatric Cardiology, Colle e of Physicians and Surgeons, Columbia-Presbyterian ~ e s i c a lCenter. Reprint requests: Dr. Cersony, Babies Hospital Annex, Room 102,3975 Broadmy, New York City 10032 CHEST, VOL. 64, NO. 3, SEPTEMBER, 1973 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/20942/ on 05/02/2017