Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
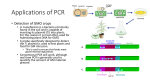
BRIEF REPORT Patients with Suspected Herpes Simplex Encephalitis: Rethinking an Initial Negative Polymerase Chain Reaction Result Ana A. Weil, Carol A. Glaser, Zahwa Amad, and Bagher Forghani Viral and Rickettsial Disease Laboratory, Division of Communicable Disease Control, California Department of Health Services, Richmond A statewide encephalitis diagnostic project of the California State Department of Health Services found that herpes simplex virus 1 DNA may not be detectable by molecular methods early in the clinical course of herpes simplex encephalitis. We describe 3 patients with herpes simplex encephalitis (HSE) whose initial PCR results were negative for herpes simplex virus 1 (HSV-1). Patient 1. A 10-year-old previously healthy white girl with chief complaints of increasing lethargy and fever was seen in the emergency department. At the time of admission, she was aphasic, inattentive, and drooling. She had swollen lips and experienced difficulty opening her mouth. Her vital signs were as follows: temperature, 39.1C; pulse rate, 126 beats/min; and respiratory rate, 24 breaths/min. She responded to her name with a nonverbal sign of acknowledgment and visually tracked her parents, but she could not follow commands. At admission, her complete blood count was within the normal range, and findings of chest and neck imaging were also normal. Three days before admission, the patient had experienced 2 episodes of vomiting, somnolence, and symptoms of an upper respiratory infection. The patient had briefly experienced disorientation and had “difficulty finding words” 1 day before admission; at that time, she was febrile and lethargic. Evaluation of the patient’s medical history disclosed no abnormal findings. Findings of a review of systems were unReceived 10 September 2001; revised 19 November 2001; electronically published 21 March 2002. Financial support: Centers for Disease Control and Prevention Emerging Infections Program (U50/CCU915546-03). Reprints or correspondence: Dr. Bagher Forghani, Viral and Rickettsial Disease Laboratory, California Dept. of Health Services, 850 Marina Bay Pkwy., Richmond, CA 94804 ([email protected]). Clinical Infectious Diseases 2002; 34:1154–7 2002 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2002/3408-0019$03.00 1154 • CID 2002:34 (15 April) • BRIEF REPORTS remarkable. The patient had experienced no recent episodes of rash, dysphasia, dysarthria, weight loss, headache, neck stiffness, or changes in vision. She was not taking any medications on a regular basis, and no significant animal exposure or foreign travel was identified. Analysis of a CSF sample obtained from lumbar puncture (LP) performed at the time of admission showed a WBC count of 90 cells/mL (75% lymphocytes, 14% monocytes, and 11% neutrophils), a protein level of 26 g/dL, and a glucose level of 73 mg/ dL (table 1). A CT scan of the head showed a small area of decreased attenuation in the left frontal lobe and associated mass effect in the left lateral lobe. Treatment with doxycycline and acyclovir was initiated. CSF samples obtained during the initial LP were found to be negative for HSV-1 by PCR performed at 3 laboratories: the hospital laboratory (targeted HSV-1 screening), a private laboratory (targeted HSV-1 screening), and the state laboratory (consensus sequence PCR testing for herpesviruses, including HSV-1) (table 2). On day 2 of hospitalization, the patient began to develop oral apraxia, and MRI showed multifocal, bilateral T2 prolongation with patchy enhancement, which was most extensive in the left temporal lobe. She had a complex partial seizure on day 3 of hospitalization. Because of temporal lobe involvement and the lack of another etiology, HSE was still suspected. On day 4 of hospitalization, a second LP was performed; analysis of the CSF sample obtained revealed a WBC count of 113 cells/mL (83% lymphocytes), a protein level of 107 g/dL, and a glucose level of 59 mg/dL (table 1). HSV-1 was detected by PCR performed at both the state laboratory and the hospital laboratory. Patient 2. A 37-year-old man presented with fever, memory loss, photophobia, and disorientation. MRI revealed lateral temporal lobe enhancement. Examination of a CSF sample obtained from an initial LP performed at the time of admission revealed pleocytosis and a slightly increased protein level (table 1). This sample was found to be negative for HSV-1 on the basis of PCR performed at the state laboratory and at an outside laboratory. Seven days later, a CSF sample obtained during a second LP was found to be positive for HSV-1 by PCR done at the state laboratory and at a different outside laboratory (table 2). Patient 3. A 78-year-old woman had onset of HSE that was characterized by fever and altered mental status that rapidly progressed to seizures and coma. Because clinical deterioration and significant temporal lobe edema were seen on MRI, she underwent a temporal lobectomy. Her first CSF sample, which was obtained at the time of admission, showed pleocytosis and Table 1. Clinical and laboratory characteristics of patients with herpes simplex encephalitis who had an initial negative PCR result. Age in years, Patient sex Race WBCs/mL (% differential) Clinical findings Imaging method and finding(s) At LP 1 At LP 2 MRI: edema of left temporal lobe 90 (75% L, 11% N) 113 (83% L, 13% M, 4% N) 1 10, M W Fever, lethargy, disorientation aphasia, seizure 2 37, M W Fever, headache, disorientation CT: normal; MRI: lateral temporal memory loss, confusion lobe enhancement 330 (100% L) 3 78, F W Fever, lethargy disorientation, seizures, coma 720 (50% L, 49% M) NOTE. CT: hemorrhage, edema of right temporal lobe; MRI: edema 1356 (100% L) 624 (84% L, 9% M, 7% N) Protein level, mg/dL Glucose level, mg/dL Serum IgG index Acute ConvalesAt LP 1 At LP 2 At LP 1 At LP 2 phase cent phase 26 107 73 59 1.39 16.9 85 131 53 53 6.57 20.7 132 253 69 49 5.05 17.0 L, lymphocytes; LP 1, first lumbar puncture; LP 2, second lumbar puncture; M, monocytes; N, neutrophils; W, white. For each patient, the LP 1 was performed at the time of admission. Table 2. Results of PCR analysis of CSF samples obtained from patients who had an initial negative PCR result. Patient No. of days between onset of CNS symptoms and LP 1 HSV PCR result (laboratory a where PCR was performed ) for sample from LP 1 LP 2 No. of days between LP 1 and LP 2 1 3 Negative (A, B, D) Positive (A, D) 4 2 2 Negative (A, C) Positive (A, B) 7 3 1 Negative (A) Positive (A, B) 4 NOTE. HSV, herpes simplex virus; LP 1, first lumbar puncture; LP 2, second lumbar puncture. a A, laboratory A (i.e., the California State Health Department Viral and Rickettsial Disease Laboratory; uses consensus-sequence PCR for herpesviruses and reports a detection rate of ⭐100 copies/mL); B, laboratory B (i.e., a private laboratory other than the hospital laboratory; uses targeted HSV-1 PCR and reports a detection rate of ⭐10 HSV-1 copies/mL); C, laboratory C (i.e., a private laboratory other than the hospital laboratory; uses targeted HSV-1 PCR and reports a detection rate of ⭐100 HSV-1 copies/mL); D, laboratory D (i.e., the hospital laboratory; uses targeted HSV-1 PCR and reports a detection rate of ⭐14 HSV-1 particles /mL). an increased protein level; this sample was found to be negative for HSV-1 by PCR performed at the state laboratory (table 1). A second CSF sample, which was obtained during LP performed 4 days later, tested positive for HSV-1 by PCR performed at the state laboratory and at an outside laboratory (table 2). Discussion. HSV has been established as a common cause of acute, necrotizing encephalitis that may present at any age. With an estimated frequency of 1 case in 250,000–500,000 people per year, HSE is the most common cause of sporadic encephalitis in the United States [1]. Without receiving prompt antiviral therapy, up to 70% of patients with HSE can die [2]. For this reason, rapid and accurate diagnostic procedures are essential for management of the disease. PCR analysis of CSF samples is recommended as the standard method for diagnosing HSE [1]. Compared with brain biopsy, which was the previous diagnostic standard, PCR is preferred because of its high sensitivity and specificity as well as its noninvasive nature. The sensitivity and specificity of PCR for the detection of HSV-1 have been documented as 91% and 92%, respectively, in patients with biopsy-proven disease [1]. PCR has been documented as a useful method for diagnosing HSE early in the course of infection [3]. However, there have been reports of individuals with HSE for whom a CSF sample obtained early in the course of disease was negative for HSV1 by PCR but for whom CSF samples obtained a few days later were found to be positive by PCR [4–6]. In a prospective study of 27 adult patients with acute viral encephalitis, 10 patients had HSE diagnosed by PCR analysis of CSF samples. For 2 of these patients, the CSF samples obtained at admission were found to be negative for HSV-1 DNA, but samples obtained 4 and 7 days later had positive test results [4]. In a retrospective study of 22 patients with HSV-1 encephalitis, 1 patient had a negative PCR result for a CSF sample obtained on the third day after the onset of disease but had a positive PCR result for 1156 • CID 2002:34 (15 April) • BRIEF REPORTS a CSF sample obtained from an LP performed 5 days later [5]. There are 2 additional studies in which patients with HSE whose initial PCR results were negative for HSV-1 early in the course of infection were found to be positive for HSV-1 when a CSF sample obtained subsequently was tested [6, 7]. The California Encephalitis Project (CEP) performs diagnostic tests on samples obtained from immunocompetent, previously healthy patients with encephalitis who are 16 months of age. Although the state laboratory tests CSF samples for HSV1 DNA by use of a consensus-sequence PCR test, the CEP strongly encourages that all patient samples also be analyzed by PCR for targeted HSV-1 at another laboratory. Therefore, the majority of patients enrolled in the CEP have a minimum of 2 HSV-1 PCR analyses performed on CSF samples obtained from an initial LP. As of 15 December 2000, the CSF samples of 291 patients with encephalitis who were enrolled in the CEP had undergone PCR for the detection of HSV-1. A commercial PCR kit (Argene-Biosoft) was used for testing for herpesviruses. This kit uses consensus primers (stair primers), that are capable of amplifying HSV-1, HSV-2, cytomegalovirus, Epstein-Barr virus, varicella-zoster virus, and human herpesvirus 6 in a single reaction [8]. For serologic testing, an antibody assay for the detection of HSV IgG is performed on paired serum samples by use of an EIA, and an index value is determined for each sample [9]. A total of 11 (3.8%) of 291 patients in the CEP had PCR results that were positive for HSV-1. Three (27%) of these 11 patients had negative results of initial PCR testing for HSV-1 in CSF samples obtained at the time of admission; these 3 patients later had positive PCR results for CSF samples obtained at 4, 7, and 4 days after the first LP. These patients had serologic test results that supported the diagnoses of HSE and clinical courses consistent with HSE (table 1). For all 3 patients, the first CSF sample was obtained at the time of treatment initiation (table 2). It has been speculated that an increase in the HSV- 1 DNA level occurs during the first few days of administration of antiviral therapy, which may be responsible for this finding [10]. HSE typically evolves over several days and is associated with progressive deterioration of consciousness. The 3 patients that we describe had CNS symptoms for only 1–3 days before admission. This would suggest that these 3 patients presented relatively early during the clinical course of HSE, and they may have had a very low number of copies of the target HSV-1 DNA present in their initial CSF sample. Conventional PCR methods for detection of HSV-1 were used by the different laboratories involved in evaluation of these patients; the methods had comparable sensitivities (table 2). Nested PCR is considered more sensitive than conventional PCR because it includes a second amplification step; theoretically, the procedure is able to detect a single copy of the target HSV-1 DNA [7, 11]. Because the laboratories involved in diagnostic testing of these patients used conventional PCR, it is important to be aware of the negative results obtained under these circumstances. The initial negative PCR results that were obtained for the cases we report are not likely to have been the result of inhibitors, because the Elongase DNA polymerase (Gibco BRL) used by our laboratory is less affected by hemoglobin than is Taq DNA polymerase. In addition, the initial CSF samples all had !5 RBCs/mL, a finding that suggests that minimal hemoglobin levels were present. Finally, inhibitors generally are less problematic for PCR testing of CSF than they are for PCR testing of other body fluids or tissue extracts. Observation of initial negative PCR results for a small but notable number of patients with confirmed HSE infection indicates that a PCR result that is negative for HSV-1 early in the course of infection does not rule out the presence of HSE. Diagnosis of HSE should be based on clinical findings in combination with the results of neuroimaging and diagnostic testing. For patients for whom HSV-1 infection is still suspected (i.e., for those with temporal lobe involvement and no alternative diagnosis), a second LP and subsequent PCR testing for HSV-1 should be considered. Acknowledgments We thank George F. Brooks, Giorgio Cosentino, Cynthia Cossen, David Cottam, Fred Drach, Sabrina Gilliam, Mary Ellen Guroy, Somayeh Honarmand, David Lennette, Evelyne Lennette, Gordon Shell, James Sejvar, and Erica Steffe for their valuable assistance. References 1. Whitley RJ. Herpes simplex viruses. In: Scheld WM, Whitley RJ, Durack DT, eds. Infections of the central nervous system. 2nd ed. Philadelphia: Lippincott-Raven, 1997:73–89. 2. Whitley RJ, Soong S-J, Hirsch MS, et al. Herpes simplex encephalitis: vidarabine therapy and diagnostic problems. N Engl J Med 1981; 304: 313–8. 3. Cinque P, Cleator T, Weber, Monteyne P, Sindic CJ, van Loon AM. The role of laboratory investigation in the diagnosis and management of patients with suspected herpes simplex encephalitis: a consensus report. J Neurol Neurosurg Psychiatry 1996; 61:339–45. 4. Studahl M, Bergstrom T, Hagsberg L. Acute viral encephalitis in adults—a prospective study. Scand J Infect Dis 1998; 30:215–20. 5. Guffond T, Dewilde A, Lobert PE, Caparros-Lefebvre D, Hober D, Wattre P. Significance and clinical relevance of the detection of herpes simplex virus DNA by the polymerase chain reaction in cerebrospinal fluid from patients with presumed encephalitis. Clin Infect Dis 1994;18: 744–9. 6. Koskiniemi M, Piiparinen H, Mannonen L, Rantalaiho T, Vaheri A. Herpes encephalitis is a disease of middle aged and elderly people: polymerase chain reaction for detection of herpes simplex virus in the CSF of 516 patients with encephalitis. J Neurol Neurosurg Psychiatry 1996; 60:174–8. 7. Aurelius E, Johansson B, Skoldenberg B, Staland A, Forsgren M. Rapid diagnosis of herpes simplex encephalitis by nested polymerase chain reaction assay of cerebrospinal fluid. Lancet 1991; 337:189–92. 8. Minjolle S, Michelet C, Jusselin I, Joannes M, Cartier F, Colimon R. Amplification of the six major human herpesviruses from cerebrospinal fluid by a single PCR. J Clin Microbiol 1999; 37:950–3. 9. Forghani B. Enzyme immunoassay systems. In: Lennette EH, ed. Laboratory diagnosis of viral infections. 2nd ed. New York: Marcel Dekker, 1992:105–25. 10. Roos KL. Pearls and pitfalls in the diagnosis and management of central nervous system infectious diseases. Semin Neurol 1998; 18:185–96. 11. Persing DH. In vitro nucleic acid amplification techniques. In: Persing DH, Smith TF, Tenover FC, White TJ, eds. Diagnostic molecular microbiology—principle and application. Washington, DC: American Society for Microbiology, 1993:51–87. BRIEF REPORTS • CID 2002:34 (15 April) • 1157