Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Electrocardiography wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Cardiac surgery wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
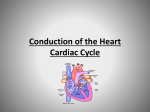
“Lub Lub Lub Dub” Goes the Heart- Atrial Fibrillation Your heart doesn’t just contract every second (or so) for your entire life without any help; there are a pattern of electrical impulses that allow this amazing organ to do so. Both of these impulses stem from a different electrical ‘node’; the sinoatrial node (SAN) and the atrioventricular node (AVN). These two nodes stimulate the contraction of the four chambers of the heart and do so in such a way that the optimum amount of blood enters and leaves the heart during each cardiac cycle/’Lub Dub’. The Cardiac Cycle: 1. In the first stage of the cardiac cycle the heart is relaxed and so all its valves are open. This allows the atria of the heart to fill with blood from the vena cava (left atrium) and the pulmonary veins (right atrium), as well as allowing small amounts of this blood to enter the ventricles through the heart’s two atrioventricular valves. 2. After the atria have filled with blood, the SAN sends out an electrical impulse across the atria, causing them to contract, before it is stopped by a layer of non-conducting tissue as it stimulates the AVN. 3. When the AVN is stimulated, after a short delay which allows blood from the atria to enter the ventricles, it too sends out an electrical impulse, through the Bundle of His, down the interventricular septum, to the apex of the heart and up the subendocaridial branches (a.k.a the purkinje fibres) causing the ventricles to contract from the bottom, up. This upwards contraction in the ventricles in very important, as it means the blood is forced towards the semilunar valves at the top of each ventricle forcing them to open. 4. The heart then relaxes once again before the cycle restarts. Aiden McGowan Atrial fibrillation is a condition that affects 6 million people in Europe alone; many of whom are unaware of the condition. However, there are many different types of atrial fibrillation which are defined depending on the degree to which it affects a person; some of these types are: Long-standing persistent atrial fibrillation, which is diagnosed when a patient has had atrial fibrillation for a year or longer, continuously. Permanent atrial fibrillation, which is diagnosed when the patient’s heart is constantly in atrial fibrillation. Persistent atrial fibrillation, in which each episode of atrial fibrillation suffered by a patient/person last for 7days or longer. Paroxysmal atrial fibrillation, which is where episodes are frequent but usually stops within 48 hours if untreated. A-Fib is the irregular contractions of the two smaller chambers of the heart, the (left and right) atria which is caused by the random firing of many triggers from the SAN which essentially fight to get through the AVN. Due to these contractions being irregular and erratic, the overall rhythm of the heart is disturbed as the atria are not in sync with the other two, larger chambers of the heart; the ventricles. Your heart uses multiple electrical impulses as pacemakers to ensure it beats rhythmically, these impulses stem from different electrical nodes, the sinoatrial node (SAN) and the atrioventricular node(AVN).These two nodes stimulate the contraction of the four chambers of the heart and do so in such a way that the optimum amount of blood enters and leaves the heart during each cardiac cycle, or ‘beat’. What Does This Mean for Sufferers? Due to the atria not contracting in time with the ventricles, less blood enters the atria at the beginning of the cardiac cycle when the heart should be at rest, because it rarely is. This means less blood is then pumped to the ventricles, leading to a large overall reduction in cardiac output; this is a problem. Cardiac output is the term given to the volume of blood that leaves the heart every minute and is found using the equation: Stroke volume (the amount of blood pumped by each ventricle in a single beat) * Heart Rate (BPM). Having a low cardiac output not only means that less blood is reaching respiring tissues, but it also means, due to less blood leaving the left side of the heart, that the little blood that does reach these tissues is very low in oxygen saturation, so even less oxygen is available to the tissues. Tiredness, dizziness and fainting are all symptoms of this poor circulation and lower oxygen saturation of the blood, because the brain is one of the organs that receive less oxygen. People who suffer from atrial fibrillation will often feel their heart ‘flutter’ (heart palpitations), obviously due to the atria’s rapid contractions. Aiden McGowan What Causes Atrial Fibrillation? The causes of atrial fibrillation are still mostly unknown to doctors and researchers; however it is thought that a genetic component may be present. Atrial fibrillation can be cause by the electrical pathways in the heart altering, causing the many impulses to ‘fight’ for a passage through the AVN; this is usually the cause in older people. Treatment/Management of Atrial Fibrillation Once you have been found to suffer with atrial fibrillation, there are a few treatment options available, depending on many factors. These factors include the type of A-Fib you suffer from as well as your age, your overall health and whether an underlying cause can be identified. If an underlying cause of your a-Fib can be identified, you may only require treatment for that in order to stop it. For example, if you are found to have an overactive thyroid, you may only be treated for that, via medication, in order to stop your atrial fibrillation. On the other hand, if no cause can be found by your doctors, a number of treatment options are available, ranging from medicines to reduce your risk of stroke (as this risk is heightened by A-Fib), to medicines that control atrial fibrillation directly and even cardioversion (receiving electric shocks in order to reset the heart’s overall rhythm). More invasive treatments, such as removing or terminating faulty electrical pathways from the atria of the heart, are also used; this particular procedure is known as ‘catheter ablation’. Sources: www.nhs.co.uk www.stopafib.org Aiden McGowan