Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Telecommunications relay service wikipedia , lookup
Auditory processing disorder wikipedia , lookup
Lip reading wikipedia , lookup
Olivocochlear system wikipedia , lookup
Sound localization wikipedia , lookup
Hearing loss wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
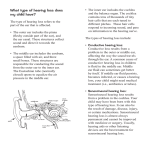
How the Ear Works The ear consists of the following three parts: the outer ear, the middle ear, and the inner ear. The outer ear consists of the “ear” as we see it as well as the ear canal. A person hears speech and other sounds as a result of sound waves entering the ear through the ear canal. The middle ear consists of the eardrum as well as three bones that are attached to the eardrum. These bones are called the malleus, incus, and stapes and are referred to as the ossicles. When sound travels through the ear canal it vibrates the eardrum. Because the ossicles are attached to the eardrum, when the eardrum vibrates they vibrate as well. The ossicles vibrate against a membrane, called the oval window that leads to the inner ear. The inner ear consists of two parts – the cochlea, which is the organ of hearing, and the semicircular canals, which are the organs of balance. The cochlea looks like a snail and is filled with fluid. When the ossicles vibrate against the oval window the vibration is transferred to the fluid. The cochlea also contains thousands of hair cells that sway back and forth as the fluid moves. The movement of the hair cells stimulates the nerve fibers of the auditory nerve and sends a signal to the brain, which allows us to hear the sound. Hearing loss can originate in any of the three main parts of the ear. Depending on which part of the ear is involved, the characteristics of the hearing loss as well as the way we treat that hearing loss is different. Types of Hearing Loss Sensorineural hearing loss Sensorineural hearing loss is caused by damage to the cochlea and/or auditory nerve. The hair cells in the cochlea, which are necessary to stimulate the auditory nerve, may be damaged or absent in a sensorineural hearing impairment. The hair cells are “tuned” to respond to specific pitches, so depending on which hair cells are damaged, a child may be able to hear certain pitches better than others. When sensorineural hearing loss occurs sounds need to be louder, especially in the pitch range where the hair cells are damaged, for a child to hear them. Because of the nature of inner ear/auditory nerve damage, people with sensorineural hearing loss often have difficulty with clarity of sound, not just loudness. Sensorineural hearing loss can not be medically repaired, so people with this type of hearing loss are good candidates for hearing aids or other hearing devices. Conductive hearing loss Conductive hearing loss is caused by a problem in the outer or middle ear which inhibits the transmission of sound to the inner ear. The hair cells and nerve fibers in the inner ear, in this case, are not damaged. A conductive hearing loss effectively acts as an earplug by diminishing the loudness of the sounds, while having little effect on clarity since the inner ear is not damaged. Middle ear infections, fluid behind the eardrums, ear wax, and certain conditions involving the ossicles can cause conductive hearing loss. Conductive hearing loss is usually medically treatable; however, in some cases of conductive hearing loss, hearing aids may be recommended. Mixed hearing loss Mixed hearing loss involves both the outer/middle ear and the inner ear. Middle ear infections are common in young children; if a child has a sensorineural hearing loss and then develops a middle ear infection which causes a conductive component to the loss, the loss is called a mixed hearing loss. A 2 conductive impairment combined with a sensorineural impairment can further diminish a child’s hearing, leaving him or her with decreased access to sounds. Regular visits to the audiologist, pediatrician, or ENT (ear, nose and throat) doctor are advisable to monitor your child’s hearing health. How we Assess Hearing in Children It is important to understand the necessity of a battery of tests for determining your child’s hearing status. The results of any one test alone are not as strong as the culmination of results of two or more tests. Appropriate measurement of the type and degree of your child’s hearing loss is paramount for providing appropriate intervention and amplification if indicated. Behavioral hearing tests When a child is willing and able, the preferred method of hearing testing is using behavioral testing. This requires the child to respond to sounds at different loudness levels and different pitches to determine the minimum levels to which he/she can attend. This testing is performed in a sound-treated booth. Your child may wear headphones, earphones, or listen to sounds through speakers placed in the testing booth. The audiologist looks for consistent responses to the sound, such as head turns from younger children or more complex play responses as the child gets older, such as dropping a block in a bucket when he/she hears a sound. By using different procedures and equipment, behavioral testing can provide information about the type (sensorineural, conductive, or mixed) and degree of the hearing loss for each ear. Results are recorded on a graph called an audiogram. Objective hearing tests For children younger than about 6 months of age, or for those who are unable to respond behaviorally for audiological evaluation, objective tests that do not require behavioral responses are used. A common test used is called otoacoustic emissions. This tests the integrity of the hair cells in the cochlea by measuring tiny echoes that the inner ear sends out in response to sounds 3 presented to the ears. This test requires the child to be quiet but not necessarily asleep and generally takes less than 5 minutes per ear. Generally, if otoacoustic emissions are present they indicate that the cochlea is functioning properly. There are rare occasions, however, when the cochlea is functioning properly but a child still does not respond to sound behaviorally. Another objective test often used to estimate hearing sensitivity is called an auditory brainstem response (ABR) test. This test requires that your child be asleep and takes 30-60 minutes to complete. Electrodes are placed on your child’s skin, which pick up the electrical activity generated from his/her auditory nerves and part of the brainstem that is involved in hearing. The audiologist examines the recorded waveforms and interprets them to determine an estimate of the degree and type of hearing loss that is present. Tympanometry Tympanometry is a test that evaluates middle ear and eardrum function. Because middle ear problems are common in young children, tympanometry should be performed routinely on your child. A rubber tip, connected to a machine called a tympanometer is held up to your child’s ear canal. The machine measures the eardrum movement in response to different tones and air pressure changes and records the results on a graph called a tympanogram. This provides information about your child’s middle ear and eardrum. 4