Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
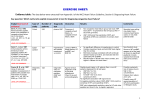
National Public Health Service Brain natriuretic peptide Rapid review of the evidence for targeted brain natriuretic peptide testing in the detection of cardiac failure in primary care populations Author: Dr M Webb, Public Health Practitioner Date: October 2008 Version: 2 Status: Final Intended Audience: Monmouth Local Health Board; Cardiac networks Purpose and Summary of Document: Brain natriuretic peptide (BNP) assays for ruling out heart failure may be more effective and cost effective if targeted at certain ‘risk’ groups. The present document summarises the evidence on effectiveness and cost effectiveness of targeted BNP testing for three groups in which the patients have different risk factors and where clinical suspicion would vary. Publication/Distribution: ? Version 2 Author Dr Mary Webb Date: October 2008 Page 1 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide Contents Page Number EXECUTIVE SUMMARY 1. BACKGROUND 2. AIMS 3. RESEARCH QUESTIONS 4. METHODS 4.1 Identifying existing and ongoing research 4.1i Literature searching 5. RESULTS 5.1 BNP levels in cardiac and non cardiac diseases 5.2 Targeted diagnosis of heart failure in primary care populations 5.3 Cut-off values and risk scores 5.4 Economic aspects 6 CONCLUSIONS 7 REFERENCES Appendix 1 Main search strategy Appendix 2 High level search strategy Appendix 3 Evidence levels and quality grading 4 4 4 5 5 5 6 6 7 9 12 13 15 19 19 20 Copyright of this draft © 2008 National Public Health Service for Wales All rights reserved Any unauthorised copying without prior permission will constitute an infringement of copyright. Version 2 Author Dr Mary Webb Date: October 2008 Page 2 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide Glossary ACS AUC BNP NT-pro BNP CE CI DOR ECG HF HTA LVSD MI QALY SOB Version 2 Author Dr Mary Webb Acute coronary syndrome Area under the curve Brain natriuretic peptide N terminal pro brain natriuretic peptide Cost effectiveness Confidence interval Diagnostic odds ratio Electrocardiogram Heart failure Health technology assessment Left ventricular systolic dysfunction Myocardial infarction Quality adjusted life year Shortness of breath Date: October 2008 Page 3 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide Executive summary There is increasing interest in the use of brain natriuretic peptides (BNP) to improve the diagnosis of heart failure (HF) in primary care and to reduce inappropriate referrals to secondary care. Clinical guidelines recommend the use of BNP assays in conjunction with other diagnostic tests in primary care, but uptake in primary care has been slow. Recently the practical application of BNP tests in primary care has been questioned. The cardiac networks in Wales have considered in detail the use of BNP in primary care and have considered the suggestion made by some cardiologists that BNP assays for ruling out HF are more effective and cost effective if targeted at certain ‘risk’ groups. The National Public Health Service was asked to perform a rapid review of the literature to assess the evidence on effectiveness and cost effectiveness of targeted BNP testing for three groups in which the patients have different risk factors and where clinical suspicion would vary. Validated methods to maximise retrieval of Level 1 and Level 2 literature were used. There was a lack of good quality evidence to answer the research questions and most of the published studies were performed in secondary care. Two good quality systematic reviews had been recently published and these were used to inform the present evidence review. Supplementary relevant evidence, not included in these two reviews, was also appraised. The published literature clearly illustrated the wide variation of BNP levels in both cardiac and non-cardiac disease and with age and gender. The lack of defined cut-off BNP values appeared to be contributing to the inconsistent evidence for the effectiveness of BNP testing. Considerable efforts are being made to clarify the issue of cut-off values and there was data indicating that with a level of <100pg/ml that shortness of breath was unlikely to be due to significant heart failure. The combination of risk scores with BNP testing may be an effective approach. The cost effectiveness studies were also inconclusive, but a good quality systematic review with a comprehensive economic analysis, indicated that diminishing returns could occur with BNP testing being used in primary care and that the use of such assays should be limited to patients in whom the cause of shortness of breath is very doubtful. There was some data to suggest that hand held/portable echocardiography may be potentially cost effective. Version 2 Author Dr Mary Webb Date: October 2008 Page 4 of 20 Status: Final Intended audience National Public Health Service 1. Brain natriuretic peptide Background In primary care the burden of heart failure (HF) is exacerbated by problems with inaccurate diagnosis that may result in inappropriate referrals for echocardiography. Echocardiography is generally recognised as the ‘gold standard’ test.1 2, but in Wales, as in some other countries, the demand for out-patient and in-patient echocardiography, both for HF and other cardiac conditions already exceeds the capacity of current services.3 Some guidelines suggest that brain natriuretic peptides (BNP) and N terminal pro brain natriuretic peptide (NT-proBNP) and electrocardiography (ECG) can be used as diagnostic tools to support general practitioners in their assessment of patients with suspected heart failure and possible reduce the demand for echocardiography. 1 4 Concern has been expressed however, that there is a lack of good evidence that the use in primary care of BNP measurement, as a filter for echocardiography, significantly reduces the number of referrals for echocardiograms 5 6 and other international guidelines do not recommend routine BNP testing. 7 The cardiac networks in Wales are considering the use of BNP to diagnose HF in primary care and an Expert Group has produced several key documents. 8 Recently the SE Wales Cardiac Network has suggested that BNP testing may be more effective if it could be targeted at different risk groups and has identified three groups of patients with different risk factors and where clinical suspicion would vary. 2. 3. Aims To determine the evidence for the effectiveness and cost-effectiveness of differential application of BNP testing for cardiac failure in primary care populations presenting with clinically identified high, medium and low risk symptoms. To identify additional information for BNP cut-off points in each of the risk groups and any data on portable echocardiography as an alternative or adjunct to the diagnosis of heart failure. Research question The aims in Section 2 were converted to structured questions for searching using the Population, Intervention, Comparison and Outcome (PICO) 9 format Populations: High risk - Patients with shortness of breath (SOB) and a history of myocardial infarction and other coronary heart diseases who would ‘always’ require full assessment with echocardiography. Intermediate risk - Patients with SOB and hypertension with abnormalities on ECG. Lower risk - Patients with SOB and no known heart failure risk factors Version 2 Author Dr Mary Webb Date: October 2008 Page 5 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide Intervention – BNP assay in primary care. Comparators – standard clinical assessment; ECG Outcome – reduction in inappropriate referrals for echocardiography and/or secondary care. 4. Methods 4.1 Identifying existing and ongoing research 4.1. 1 Literature searching Systematic searching: As per the protocol contained in The Evidence Checklist 10 a scoping search was initially performed to identify major papers on published evidence and refine the final search strategy. For the present overview, search terms contained in the search strategies were used from published reviews and they were kept broad to maximise retrieval of references. The basic search strategy is shown in Appendix 1. The amount and type of literature on BNP testing necessitated the use of a pragmatic approach to searching for evidence in order to achieve production of the review, within the very short timescale for delivery. It is clear that there had to be a balance between timeliness and rigour and high quality evidence and systematic reviews, metaanalyses, health technology assessments and clinical guidelines were identified first. It should be emphasised therefore that this review is not a systematic review of primary studies but is the result of searches for best evidence. High level searching: It is well known that the classical databases for medical literature, such as Medline, do not adequately index all relevant literature. The reviewer used validated methods that involved the use of meta-search engines and other databases for ‘high level’ searching to quickly identify relevant evidence. (Appendix 2) For critical appraisal, the tables recommended for use in the National Institute for Health and Clinical Excellence Guideline Development Methods manual 11 were modified to accept the type of studies identified for the use of BNP testing in the diagnosis of HF. The data relevant to the research question was entered into an evidence table. The quality of the evidence was graded using the NICE hierarchy of evidence and the quality checklists. Evidence was rejected if graded as poor quality, apart from where it was of Level 1 type (see Appendix 3 for explanation of evidence grading system) and was highly relevant to the questions. Due to practical limitations a single reviewer performed the final selection, critical appraisal and data extraction. Inclusion Criteria Version 2 Author Dr Mary Webb Date: October 2008 Page 6 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide Adults presenting to primary care with symptoms described in the three risk groups in Section 3. Search period January 2000 – May 2008 Papers in English, German, French or Spanish Interventions relating to the use of BNP testing in patient populations with differing symptoms presenting to primary care with the possible diagnosis of HF. Randomised controlled trials (RCT) Systematic reviews Meta-analyses Guidelines Observational studies (where higher quality evidence was not available) 5. Results The scoping search revealed two recent high quality health technology assessments (HTAs) /systematic reviews 12 13 (Level 1-) that were of relevance and these were used extensively to inform the present report. Other pertinent evidence, not included in these HTAs was also appraised. 5.1 BNP levels in cardiac and non cardiac diseases For the effective use of BNP in patients with different symptoms suggestive of HF, the levels of BNP in different diseases are relevant. In general, all the 21 cardiac diseases considered in one HTA12 were associated with an increase in BNP and NT-pro BNP. These included diastolic dysfunction14 15, cardiac decompensation 16acute right HF 17 and cardiac pulmonary oedema. 17 Acute right HF without cardiac pulmonary decompensation was not related to BNP concentration. Patients with cardiac pulmonary oedema had higher levels of BNP than patients with obstructive lung disease. Patients with diastolic dysfunction had raised BNP levels but they were not as elevated as patients with systolic dysfunction. 14 15 . Patients with acute coronary syndrome (ACS) had elevated NT-proBNP levels, 18 but there was no difference between patients with and without ischemic heart disease, unless the patients had cardiovascular risk factors. 19 20 Acute myocardial infarction (MI)19 21, or previous MI22 23 were associated with increased levels of BNP. Stable angina was not associated with a difference in B-type natriuretic peptides in one study 19 that included hypertensive patients, but was positively associated in patients with non STelevation myocardial infarction (NSTEMI) ACS. 24 There was no difference between patients with dilated cardiomyopathy and previous MI.25 Arrhythmia 26 was associated with elevated levels of B-type natriuretic peptides; however, there was no difference between atrial fibrillation and sinus rhythm 27 valvular disease 26 and all severities of aortic stenosis 28 were positively associated with B-type natriuretic peptides levels. The effect of 11 non-cardiac diseases on B-type natriuretic peptide levels was mixed. Non-cardiac causes of dyspnoea, 29 30 31 diabetic nephropathy,32 and Version 2 Author Dr Mary Webb Date: October 2008 Page 7 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide stroke 33 were all associated with increased levels of B-type natriuretic peptides. Lung disease compared with HF34 or HF plus lung disease 35 had lower BNP and NT-proBNP levels respectively. Diabetic retinopathy 36 and cerebrovascular disease (including stroke and transient ischemic attack) 19 33 did not show association with B-type natriuretic peptide levels. Four of five studies that evaluated hypertension 37 38 39 showed a positive association with B-type natriuretic peptides; duration of hypertension was not associated with BNP levels. 37 There was no difference in NT-proBNP levels between patients with peripheral vascular disease compared with patients without risk factors for cardiovascular disease. 19 5.1 CONCLUSION – The levels of BNP are variable in both cardiac and non cardiac disease and the need for characterisation of cut-off values for each clinical condition present in the different risk populations is vital. 5.2 Targeted diagnosis of heart failure in primary care populations The majority of published evidence was from studies performed in the acute or secondary care setting and there was a lack of direct high quality evidence from studies performed in primary care to answer the research questions. It proved difficult to determine the symptoms of the patients described in the published studies and therefore to assign them to the three chosen risk groups for the present review; a linked evidence approach was therefore adopted. One good quality HTA 12 included a total of seven papers (data could be abstracted from only five), that selected patients from a primary care setting. Five of these studies were cross-sectional in design 38 26 35 40 41 and one was a RCT. 42 There was one study that selected patients randomly and identified a high risk cohort group that is possibly equivalent to the intermediate risk group in the present review and one group with established HF that corresponds to the high risk group. 43 Two studies evaluated BNP with cut-off points ranging from 10 to 115 pg/ml and reported sensitivities from 66 to 92%, specificities from 18 to 88%, the area under the curve (AUC) from 0.70 to 0.88, LR+ from 1.12 to 5.7, and LR- from 0 to 0.27. Meta-analysis gave a summary DOR of 2 (95 % CI: 1 to 6). The three studies evaluating NT-proBNP with cut-off points from 67 to 338 pg/ml reported sensitivities from 67 to 100%, specificities from 18 to 84% , AUC from 0.70 to 0.93, LR+ from 1.22 to 5.7, and LR- from 0 to 0.27. Meta-analysis gave a summary diagnostic odds ratio (DOR) of 17 (95 % CI: 9 to 32) The authors suggested that the wide variation in specificity may be due to the effect of determinants such as age, obesity, other diseases (e.g., hypertension, diabetes, renal failure) or drugs (e.g., beta blockers, diuretics, angiotensin converting enzyme (ACE) inhibitor) on BNP levels. The included studies were of good quality. The Australian HTA 13 included a more recent study 44(Level 2+) not included in the American HTA 12 described above, which contained higher quality data but was not a randomised study. The evidence on the diagnostic accuracy of Version 2 Author Dr Mary Webb Date: October 2008 Page 8 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide BNP tests in primary care indicated that the test is likely to aid in the earlier identification of alternative diagnoses for those patients ‘ruled out’ from having HF and most of these alternative diagnoses (pulmonary diseases, asthma, anaemia) have established treatments. When this alternative pathology is severe enough, early identification and treatment is likely to benefit the patient. The clinical impact of the test is however unknown. The HTA13 considered evidence for NT-pro BNP assays separately and the conclusions from the results were similar to those of BNP apart from the possible indication that NT-proBNP assays may be more useful in ruling out HF more frequently in those patients presenting with dyspnoea and/or oedema of recent onset and suspected of HF. The Australian Medical Services Advisory Committee has recommended that public funding be supported for the use of BNP assays in the diagnosis of HF in the hospital emergency setting but not in the non-hospital setting. It would appear that this decision was taken because it is currently unknown what impact the introduction of the tests will have on the current echocardiography referral rate for those who test positive The good quality meta-analysis ( Level 1+) published by Battaglia in 200645 summarised the evidence on the diagnosis of HF and also compared the performance of a rapid enzyme linked immunoabsorbent assay (ELISA) with the standard radioimmunoabsorbent (RIA) test and included studies ranging from asymptomatic patients in the community to patients presenting with acute dyspnoea in emergency departments. The authors concluded that negative results of both tests accurately rule out the diagnosis if patients are at relatively low risk of chronic HF and that the use of BNP tests in low-risk patients in primary care settings could reduce demand for echocardiography and referrals of patients to specialists. The ELISA test, which allows bedside testing and provides results in a few minutes, performed somewhat better than the RIA tests, which must be sent to a laboratory, but it is more costly than RIA. The effect of introduction of such tests on patient outcomes or cost is as yet unknown. One methodological problem with this study was that it was only possible to adjust for information that was aggregated at study level since individual patient data was not available. The systematic review of Latour-Perez et al.46 (Level 1- ) concluded that BNP was less useful for ruling out left ventricular systolic dysfunction (LVSD) than it was for ruling out HF; this study is however of poor quality and the conclusions should be viewed with caution. Another study 47(Level 1- ) also looked at the diagnostic value of BNP and indicated that a BNP level of 80pg/ml is useful in diagnosing heart failure in symptomatic patients without a history of heart failure. This study also has methodological problems The findings of Fuat et al 200648 ( Level 2- ) should be viewed in the context of the systematic review of diagnostic tests (BNP, NT-proBNP and ECG) in the assessment of LVSD. 49 (Level 1- ) In this review of 32 studies BNP, NTproBNP and ECG were equivalent in terms of ruling out a diagnosis of LVSD. Although the negative predictive values of BNP and NT-proBNP are higher than ECG in the Fuat study, the precision of these estimates as measured by Version 2 Author Dr Mary Webb Date: October 2008 Page 9 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide the 95% confidence interval around the point estimates do overlap to a large extent. 50 The HTA from the NHS in Scotland51 (Level 2 ++) was primarily concerned with the effectiveness of different tests that can be used by GPs for an initial assessment/diagnosis of patients with signs and symptoms suggestive of HF. The assessment did not consider the use of BNP tests in patients with other diseases. The authors acknowledged that further research on audit of practice is required but indicate that BNP has potential for ruling out HF and that the estimated annual resource savings are £0.6 million to £1.4 million. These figures were however, extrapolated from a Swiss study and need verification within a UK primary care setting. 5.2 CONCLUSION - The evidence was inconsistent with regard to the effectiveness of using BNP assays in the three risk groups. It was difficult to determine the patient characteristics of the risk groups described in the published literature. It appeared that the majority of authors considered that there was not enough good quality evidence from community studies to conclusively recommend BNP testing in primary care. There was some Level 1 evidence that the targeted approach to patients with different risk factors may be clinically effective. 5.3 Cut-off values and risk scores The practical application of BNP measurement in primary care has been limited by problems in defining a cut-off threshold for effective diagnosis of HF. This has led some researchers to try and develop scoring systems in primary care that could permit the identification of patients with a poor prognosis, without relying solely on a single cut-off threshold value for BNP. In one study 52 (Level 2- ), 532 patients were followed up for 6.4 years and multivariate analysis was used to generate a prognostic scoring system that included such items as age, sex, angina, diabetes. The authors acknowledge the limitations of their study but suggest that such an approach may be useful in primary care to manage patients at different risk for HF. The cut-off scores for risk groups were 25th percentile, 411pg/ml; 50th percentile, 475pg/ml; 75th percentile, 524pg/ml. The ruling out of LVSD after MI by BNP measurement is still controversial and a recent paper from Germany suggests that evaluation of clinical information and the development of risk scores are as least as effective as NT-proBNP testing. 53 Maisel54 found that in patients referred from primary to acute care that a negative predictive value of BNP level of <100 pg/ml was the strongest feature of this peptide. Although the positive predictive value in a given patient at a cut-off of 100pg/ml is 80%, most patients with significant chronic HF as a cause of their dyspnoea will have levels of 400pg/ml. Thus, in patients presenting with levels between 100 and 400 pg/ml, one needs to exclude baseline LV dysfunction without exacerbation, pulmonary embolism, and cor pulmonale. Version 2 Author Dr Mary Webb Date: October 2008 Page 10 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide Thus it has been concluded that:55 With a cut-off of <100pg/ml: significant HF as cause of SOB can be excluded Most patients with significant HF will have a BNP> 400pg/ml BNP 100-400pg/ml: will exclude non relevant baseline LVD, pulmonary embolism & cor pulmonale. The diagram below gives an indication of the diagnostic accuracy of BNP testing to rule out SOB caused by HF. 55 Receiver-Operating-Characteristic Curve for Various cut-off levels of BNP in differentiating between SOB due to HF and SOB due to other causes. i i Taken from Reference 55. Permission to copy applied for. Version 2 Date: October 2008 Author Dr Mary Webb Page 11 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide The South West London Cardiac Network56 has interpreted the published cutoff data and recommended levels for use locally. (see Table 1) Table 1 AGE in years <60 60-75 >75 Cut-off value 50 97.9 49.9 99.3 100 95.4 48.9 98.3 250 94.4 49.1 99.7 Sensitivity % Specificity% NPV% Fuat 57 (Level 2 - ) reported on the use of NT-proBNP by general practitioners in 600 patients with suspected heart failure using a single recommended cutoff point of 150pg/ml. 396 (66%) of assays were above the limit, of which 348 patients were assessed in clinics and 84 had LVSD (14% of the total cohort). The age range for all patients was 35 to 95 with a median of 77 years and 368 (61%) were women. Of the 249 (75%) without LVSD, the majority had cardiovascular causes for a raised NT-proBNP level. Introduction of the assay increased waiting times for one-stop diagnostic clinics from 2 to 8 weeks and was not of cost benefit. The authors concluded that the optimum cut-point for use in real life primary care prior to referral for echocardiography has yet to be resolved. The preliminary results of the international collaborative study of NT-proBNP in patients referred from primary care to secondary care have some indirect relevance to the research questions in that they indicate possible cut-off values for BNP/NT-proBNP. Data was obtained from 4604 patients (2575 males, 2029 females) from 16 centres in the UK, Europe and the US. The median age was 61 years (range 18.4 to 94.4 years, interquartile range 53 to 70 years) with a disease prevalence of 14.8%. Individual AUCs ranged from 0.974 to 0.835 according to the prior probability of disease in the population studied (2.2 to 26.6%). Overall, the AUC for the pooled data was 0.898 (confidence interval 0.886-0.911). Analysing the data according to age intervals produced AUC's for ages <50, 50-75 and >75 years respectively of 0.950 (0.927-0.973); 0.909 (0.894-0.924); 0.855 (0.815-0.894). The optimised decision thresholds were respectively, 79, 102 and 225 pg/L. Using optimised age and sex specific reference limits from a previous study produced sensitivities and negative predictive values (NPV) of: Males < 60 years: sensitivity 93.9%, NPV 98.2% Females <60 years: sensitivity 90.4%, NPV 88.2%; Males > 60 years: sensitivity 91.3%, NPV 96.1%; Females > 60 years: sensitivity 88.3%, NPV 90.3%. . 5.3 CONCLUSION - There was a lack of consistency in the literature on the cut-off levels for BNP to diagnose HF and other diseases in primary care and it was acknowledged that this is limiting the use of BNP in the community. There was data suggesting that a cut-off value of <100pg/ml Version 2 Author Dr Mary Webb Date: October 2008 Page 12 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide could exclude significant HF as a cause of SOB, which may have relevance to the ‘low risk’ group. The combination of BNP assays with risk scores may have clinical potential. One problem with the published studies was that they often considered patients already triaged to secondary care and therefore may not include all patients presenting to primary care. 5.4 Economic aspects There have been few economic evaluations of BNP testing in primary care. The extent of the effectiveness in terms of quality adjusted life years (QALYs) depends on the extent to which BNP tests hasten the correct definitive diagnosis, as well as on the influence of a correct diagnosis on the disease outcome. The cost effectiveness (CE) rests on the value of the additional information made available by the assays in terms of health gain and resource savings compared with the cost of the tests. In the Australian HTA 13 one analysis was largely based on symptomatic patients i.e. those presenting with SOB and/or oedema of recent onset and suspected of HF. In the absence of any RCT in primary care with health outcome as the primary outcome, it was impossible to estimate an incremental CE ratio based on life years saved or QALYs in this setting. One way sensitivity analysis indicated that diminishing marginal returns could arise if the testing is extended to GP populations that have a high probability of HF. Such diminished returns could also arise if testing is performed on increasing proportions of patients with minor levels of symptoms without clinically important pathology. It is therefore very important that the test is only ordered for patients with dyspnoea and/or oedema of recent onset in whom there is genuine uncertainty about whether the symptoms are caused by HF or an alternative pathology. The HTA report from Scotland51 included an economic analysis, which suggested that if GPs’ decisions to refer patients for echocardiography, made without the assistance of BNP testing, had a specificity better than 50%, the addition of BNP would add to cost, but that the cost of £500 per additional true positive detected might be acceptable. This report has been criticised because it does not present an explicit underlying economic model and contains a number of flaws. For example, it uses the number of true-positive cases detected alone as the diagnostic effectiveness measure and the interpretation of its results depend upon how much the decision makers would be willing to pay for each additional true-positive result – a parameter unlikely to be known. Moreover, the analysis does not take all patient groups to a definitive diagnosis: real-life strategies would incur subsequent costs, when patients who, for example, had false-negative test results returned to primary care with unresolved symptoms requiring further investigation. 58 Goode et al.59 suggested that preliminary screening of high-risk primary-care patients using electrocardiogram QRS width or NT-proBNP alone was insufficiently precise to be clinically useful. However, including NT-proBNP and QRS width in a logistic regression model, together with evidence of prior myocardial infarction and symptoms of breathlessness or peripheral oedema gave significant reductions in the number of false positive referrals and the Version 2 Author Dr Mary Webb Date: October 2008 Page 13 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide cost per diagnosis of clinically significant left ventricular systolic dysfunction. Furthermore, Lim and colleagues60 found that while initial NT-proBNP estimation may be cost-effective in detecting any causes of heart failure, portable echocardiography remains the most cost effective strategy to assess patients with heart failure from the community. Galasko et al. 61 in a UK community study compared the effectiveness and cost effectiveness of ECG, NT-proBNP and hand held echocardiography (HE) with traditional echocardiography (TE) in screening for LVSD. The study, which has some selection bias, found that ECG, NT-proBNP and HE pre-screening prior to TE all produced considerable cost savings compared with TE screening alone. The authors suggest that because interpretation of ECGs is sometimes difficult in primary care that natriuretic peptide driven screening may be preferable. The modelling study reported by Scott et al 58 used a deterministic costconsequences analysis to compare alternative diagnostic strategies such as ECGs interpreted by hospital consultants with BNP testing. The authors concluded that the model demonstrates that for the base-case scenario, an initial diagnostic strategy of BNP was superior to ECG in terms of diagnosis of symptomatic heart failure in patients presenting to primary care, despite more initial false negatives and higher costs. The editorial accompanying the article 5 questioned whether the results of published economic studies are generalisable to primary care because there are differences in performance (and ease of use by GPs) of a point-of-care BNP assay versus a laboratorybased BNP or NT-proBNP assay; different decision cut-off points between the studies, assay cost differences and importantly the fact that in all these studies the ECG was read by experienced secondary care clinicians rather than GPs. These factors may significantly alter the cost-consequence assumptions being made. Furthermore, the studies looked at patients already triaged to secondary care and may not include all patients presenting to primary care. Thus before BNP/NT-proBNP is recommended, a prospective controlled trial in primary care of the use of both point-of-care and laboratory assays that take all patients with suspected heart failure to a definitive diagnosis is required. 5.4 CONCLUSION - The cost effectiveness data on the use of BNP in primary care was inconclusive and little published data was found that was directly relevant to the three risk groups. One good quality systematic review concluded that in order to prevent diminishing economic returns that BNP testing should be limited to patients with recent onset dyspnoea and/or oedema, where it is uncertain if the symptoms are caused by HF. There is data that is suggestive that hand held/portable echocardiography may be cost effective. 6. Conclusions The rapid review of the evidence did not find conclusive high quality evidence on the effectiveness or cost effectiveness of BNP assays in Version 2 Author Dr Mary Webb Date: October 2008 Page 14 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide the targeted diagnosis of HF in primary care and further research is required. There was evidence that was suggestive that the targeted approach in different risk groups may have potential clinically, but at present there appears to be a lack of good data from primary care and future research is required. The mixed results of the pilot studies, being performed within the UK, reported by the NHS Heart Improvement Programme2 confirmed this view. There was a lack of consistency on what BNP cut-off values should be used, but some data suggested that a value of < 100pg/ml will exclude SOB caused by significant HF. The potential use of risk scores is currently being investigated by researchers in the field. High quality cost effectiveness data was lacking, but one good quality systematic review indicated that in order to prevent diminishing returns BNP testing should only be used in patients where there is doubt over the cause of the SOB. There was some data that hand held/portable echocardiography may be of use in screening patients in primary care in combination with ECG and NT-proBNP. Version 2 Author Dr Mary Webb Date: October 2008 Page 15 of 20 Status: Final Intended audience National Public Health Service 7. Brain natriuretic peptide References 1 National Institute for Health and Clinical Excellence. Chronic heart failure: management of chronic heart failure in adults in primary and secondary care. CG5. London: NICE; 2008. Available at: http://www.nice.org.uk/CG5 [Accessed 1st Oct 2008] 2 Armstrong-Klein S. Brain-type natriuretic peptide (BNP). An information resource for cardiac networks. NHS Heart Improvement Programme 2007. Available at: http://www.heart.nhs.uk/BNP/bnp_resource_v2.pdf [Accessed 30th Sep 2008] 3 Harries J. The potential role of BNP testing in SE Wales regional heart failure services. National Public Health Service 2008. [unpublished document] 4 European Society of Cardiology. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. ESC; 2008. Available at: http://www.escardio.org/guidelines-surveys/escguidelines/Pages/acute-chronic-heart-failure.aspx. [Accessed 30th Sept 2008] 5 Fuat A. Cost-effectiveness and use of natriuretic peptides in clinical practice – do we have enough evidence yet? British Journal Cardiology 2008;15:179. 6 Cheshire and Merseyside Cardiac Network and CHD Collaborative. Diagnosing heart failure. C&MCN 2004. Available at: http://www.cmcn.nhs.uk/document_uploads/Reports/Diagnosing%20Heart%20Failure%20Report.pdf. [Accessed 1st Oct 2008] 7 National Heart Foundation of Australia and The Cardiac Society of Australia and New Zealand. Guidelines for the prevention, detection and management of chronic heart failure in Australia. 2006. Australia, National Heart Foundation of Australia [Internet]. Available at: http://www.heartfoundation.org.au/document/NHF/CHF_2006_Guidelines_NHFACSANZ_WEB_PDF-1.2MB.pdf . [Accessed 2nd Oct 2008] 8 Cardiac Networks Co-ordinating Group. Recommendations on the role of brain-type natriuretic peptides as a diagnostic test in patients suspected of having heart failure. CNCG 2008. Available at: http://howis.wales.nhs.uk/sites3/home.cfm?orgid=338. [Accessed 30th Sep 2008] 9 Sackett DL; Richardson WS; Rosenberg W et al. Evidence based medicine: how to practice and teach EBM. Edinburgh: Churchill Livingstone; 1995. 10 National Public Health Service. Evidence checklist. Available at: http://www.nphs.wales.nhs.uk. [Accessed 10th May 2008] 11 National Institute for Health and Clinical Excellence. The guidelines manual. NICE 2007. Available at: http://www.nice.org.uk/niceMedia/pdf/GuidelinesManualAllChapters.pdf. [ Accessed 30th Sep 2008] 12 Balion C; Santaguida P; Hill S et al. Testing for BNP and NT-proBNP in the diagnosis andp of Heart failure. Evidence Report/Technology Assessment No. 142. (Prepared by the McMaster University Evidence-based Practice Center under Contract No. 290-02-0020). AHRQ Publication No. 06-E014. Rockville, MD: Agency for Healthcare Research and Quality. 2006 . Available at: http://www.ahrq.gov/downloads/pub/evidence/pdf/bnp/bnp.pdf. Accessed [29th Sep 2008] 13 Medical Services Advisory Committee. B-type natriuretic peptide assays in the diagnosis of heart failure. MSAC 2007. Available at: http://www.msac.gov.au/internet/msac/publishing.nsf/Content/msac%20completed%20assessments%2 01081%20-%201100. [ Accessed Sep 29th 2008] 14 Bettencourt P; Ferreira A; Dias P et al. Evaluation of brain natriuretic peptide in the diagnosis of heart failure Cardiology 2000; 93: 19. Cited in Ref 12. Abstract read. 15 Bayes-Genis A; Santalo-Bel M; Zapico-Muniz E et al. N-terminal probrain natriuretic peptide (NTproBNP) in the emergency diagnosis and in-hospital monitoring of patients with dyspnoea and ventricular dysfunction European Journal Heart Failure 2004; 15: 301. Cited in Ref 12. Abstract read. 16 Taniguchi R; Sato Y; Yamada T et al. Combined measurements of cardiac troponin T and N-terminal pro-brain natriuretic peptide in patients with heart failure Circulation Journal 2004; 68: 1160. Cited in Ref 12. Abstract read. 17 Ray P; Arthaud M; Lefort Y et al. Usefulness of B-type natriuretic peptide in elderly patients with acute dyspnea Intensive Care Medicine 2004; 30: 2230. Cited in Ref 12. Abstract read. 18 Schnabel R; Rupprecht HJ; Lackner KJ et al. Analysis of N-terminal-pro-brain natriuretic peptide and C-reactive protein for risk stratification in stable and unstable coronary artery disease: results from the AtheroGene study European Heart Journal 2005; 26: 241. Cited in Ref 12. Abstract read. Version 2 Author Dr Mary Webb Date: October 2008 Page 16 of 20 Status: Final Intended audience National Public Health Service 19 Brain natriuretic peptide Olsen MH; Wachtell K; Tuxen C et al. N-terminal pro-brain natriuretic peptide predicts cardiovascular events in patients with hypertension and left ventricular hypertrophy: a LIFE study Journal Hypertension 2004; 22: 1597. Cited in Ref 12. Abstract read. 20 Koglin J; Pehlivanli S; Schwaiblmair M et al. Role of brain natriuretic peptide in risk stratification of patients with congestive heart failure Journal American College Cardiology 200138: 1934. Cited in Ref 12. Abstract read. 21 Panteghini M; Cuccia C; Bonetti G et al. Rapid determination of brain natriuretic peptide in patients with acute myocardial infarction Clin Chem Lab Med 2003; 41: 164. Cited in Ref 12. Abstract read. 22 Lindahl B; Lindback J; Jernberg T et al. Serial analyses of N-terminal pro-B-type natriuretic peptide in patients with non-ST-segment elevation acute coronary syndromes A Fragmin and fast Revascularisation during InStability in coronary artery disease (FRISC)-II substudy Journal American College Cardiology 2005; 45: 533. Cited in Ref 12. Abstract read. 23 Schnabel R; Rupprecht HJ; Lackner KJ et al. Analysis of N-terminal-pro-brain natriuretic peptide and C-reactive protein for risk stratification in stable and unstable coronary artery disease: results from the AtheroGene study Eur Heart J 2005; 26: 241. Cited in Ref 12. Abstract read. 24 Ray P; Arthaud M; Lefort Y et al. Usefulness of B-type natriuretic peptide in elderly patients with acute dyspnea Intensive Care Medicine 2004; 30: 2230. Cited in Ref 12. Abstract read. 25 Hamada Y; Tanaka N; Murata K et al. Significance of predischarge BNP on one-year outcome in decompensated heart failure-comparative study with echo-Doppler indexes Journal Cardiac Failure 2005; 11: 43. Cited in Ref 12. Abstract read. 26 Nielsen LS; Svanegaard J; Klitgaard NA et al. N-terminal pro-brain natriuretic peptide for discriminating between cardiac and non-cardiac dyspnoea Eur J Heart Fail 2004; 6: 63. Cited in Ref 12. 27 Dias P; Rodrigues RA; Queiros MC et al. Prognosis in patients with heart failure and preserved left ventricular systolic function Revue Portuguese Cardiology 2001; 20: 1223. Cited in Ref 12. Abstract read. 28 Weber M; Arnold M; Rau M et al. Relation of N-terminal pro-B-type natriuretic peptide to severity of valvular aortic stenosis Am J Cardiol 2004; 94: 740. Cited in Ref 12. Abstract read. 29 Bayes-Genis A; Santalo-Bel M; Zapico-Muniz E et al. N-terminal probrain natriuretic peptide (NTproBNP) in the emergency diagnosis and in-hospital monitoring of patients with dyspnoea and ventricular dysfunction Eur J Heart Fail 2004; 6: 301. Cited in Ref 12. Abstract read. 30 Logeart D; Saudubray C; Beyne P et al. Comparative value of Doppler echocardiography and B-type natriuretic peptide assay in the etiologic diagnosis of acute dyspnea Journal American College Cardiology 2002; 40: 1794. Cited in Ref 12. Abstract read. 31 Maisel AS; Krishnaswamy P; Nowak RM et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure.summary for patients in Journal Family Practice. 2002 Oct;51(10):816; PMID: 12401145] NEJM 2002; 347: 1617. Cited in Ref 12. 32 Tarnow L; Hildebrandt P; Hansen BV et al. Plasma N-terminal pro-brain natriuretic peptide as an independent predictor of mortality in diabetic nephropathy Diabetologia 2005; 48: 149. Cited in Ref 12. Abstract read. 33 James SK; Lindahl B; Siegbahn A et al. N-terminal pro-brain natriuretic peptide and other risk markers for the separate prediction of mortality and subsequent myocardial infarction in patients with unstable coronary artery disease: a Global Utilization of Strategies To Open occluded arteries (GUSTO)-IV substudy Circulation 2003;108: 275. Cited in Ref 12. Abstract read. 34 Dao Q; Krishnaswamy P; Kazanegra R et al. Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent-care setting Journal American College Cardiology 2001;37: 379. Cited in Ref 12. Abstract read. 35 Landray MJ; Lehman R; Arnold I. Measuring brain natriuretic peptide in suspected left ventricular systolic dysfunction in general practice: cross-sectional study BMJ 2000. Apr 8. 320: (7240) 985-6. Cited in Ref 12. Abstract read. 36 Redfield MM; Rodeheffer JJ; Jacobsen SJ et al. Plasma brain natriuretic peptide to detect preclinical ventricular systolic or diastolic dysfunction: a community-based study Circulation 2004;109: 3176. Cited in Ref 12. Abstract read. 37 Suzuki M; Hamada M; Yamamoto K et al. Brain natriuretic peptide as a risk marker for incident hypertensive cardiovascular events Hypertens Res 2002; 25:669. Cited in Ref 12. Abstract read 38 Bettencourt P; Ferreira A; Sousa T et al. Brain natriuretic peptide as a marker of cardiac involvement in hypertension Int J Cardiol 1999; 69: 169. 39 Richards AM; Nicholls MG; Troughton RW et al. Antecedent hypertension and heart failure after myocardial infarction Journal American College Cardiology 2002; 39: 1182. Version 2 Date: October 2008 Status: Final Author Dr Mary Webb Page 17 of 20 Intended audience National Public Health Service 40 Brain natriuretic peptide Alehagen U; Eriksson H; Nylander E et al. Heart failure in the elderly: Characteristics of a Swedish primary health care population Heartdrug 2002; 2: 211. Cited in Ref 12. Abstract read. 41 Gustafsson F; Badskjaer J; Hansen FS et al. Value of N-terminal proBNP in the diagnosis of left ventricular systolic dysfunction in primary care patients referred for echocardiography Heartdrug 2003. 3: (3) 141-6 Cited in Ref 12. Abstract read. 42 Wright SP; Doughty RN; Pearl A et al. Plasma amino-terminal pro-brain natriuretic peptide and accuracy of heart-failure diagnosis in primary care: a randomized, controlled trial Journal American College Cardiology 2003; 42: 1793. 43 Hobbs FD; Davis RC; Roalfe AK et al. Reliability of N-terminal proBNP assay in diagnosis of left ventricular systolic dysfunction within representative and high risk populations Heart 2004; 90: 866. 44 Zaphiriou A, Robb S, Murray-Thomas T et al. The diagnostic accuracy of plasma BNP and NTproBNP in patients referred from primary care with suspected heart failure: results of the UK natriuretic peptide study. Eur J Heart Fail 2005;7:537–41. 45 Battaglia M; Pewsner D; Juni P et al. Accuracy of B-type natriuretic peptide tests to exclude congestive heart failure. Arch Intern Med 2006; 166:1073. 46 Latour-Perez J; Coves-Orts F J; Abad-Terrado C et al. Accuracy of B-type natriuretic peptide levels in the diagnosis of left ventricular dysfunction and heart failure: a systematic review. Eur J Heart Fail 2006; 8: 390. 47 Carderelli R; Lumicao TG. B-type natriuretic peptide: a review of its diagnostic, prognostic, and therapeutic monitoring value in heart failure for primary care physicians. Journal American Board Family Practitioners 2003; 16:327. 48 Fuat A, Murphy JJ, Hungin APS et al. The diagnostic accuracy and utility of natriuretic peptides in a community population of patients with suspected heart failure, using near patient and laboratory assay methods. Br J Gen Pract 2006;56:327. 49 Davenport C, Cheng EY, Kwok YT et al. Assessing the diagnostic test accuracy of natriuretic peptides and ECG in the diagnosis of left ventricular systolic dysfunction: a systematic review and meta-analysis. Br J Gen Pract 2006;56: 48. 50 McCowan C; Fahey T. Diagnosis and diagnostic testing in primary care. Br J Gen Pract 2006; 56:323. 51 Craig J; Bradbury I; Cummins E et al. The use of B type natriuretic peptides (BNP and NT-roBNP) in the investigation of patients with suspected heart failure. NHS Quality Improvement Scotland, 2005; Health Technology Assessment Report 6. 52 Adlam D; Silcocoks P; Sparrow N. Using BNP to develop a risk score for heart failure in primary care. Eur Heart J 2005; 26: 1086. 53 Koschak J; Scherer M; Luers C. Natriuretic peptide vs. clinical information for diagnosis of left ventricular systolic dysfunction in primary care. BMC Family Prac 2008; 9:14. Available at: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=2267193&blobtype=pdf [Accessed 1st Oct 2008] 54 Maisel A. B-Type Natriuretic peptide levels: diagnostic and prognostic in congestive heart failure. What’s next? Circulation 2002;105:2328. 55 Shribman J. BNP a reliable marker for heart failure or just an unsound political party? Presentation 2007. Available at: www.lnrcardiacnetwork.nhs.uk/. [Accessed 1st Oct 2008] 56 Wilson G.. Optimising the use of NT-proBNP testing in primary care. Formulation of a sector wide consensus on cut-off values. South West London Cardiac Network 2007. Available at: www.heart.nhs.uk/BNP/south_west_london/optimising_NT-proBNP_in_PC.ppt. [Accessed 1st Oct 2008] 57 Fuat A, Murphy JJ, Brennan G et al. Suspected heart failure in primary care – the utility of Nterminal pro B-type natriuretic peptide (NT proBNP) as a pre-screening test for secondary care referral: a real life study. Heart 2005; 91(Suppl I): A22. 58 Scott MA; Price CP; Cowie MR. Cost-consequences analysis of natriuretic peptide assays to refute symptomatic heart failure in primary care. British Journal Cardiology 2008; 15: 199. 59 Goode KM; Clarke AL; Bristow JA et al. Screening for left ventricular systolic dysfunction in high risk patients in primary care: A cost-benefit analysis. Eur J Heart Fail 2007;9:1186. 60 Lim TK, Dwivedi G, Hayat et al. Cost effectiveness of the B type natriuretic peptide, electrocardiography for the assessment of patients from the community with suspected heart failure. Echocardiography2007;24: 228. 61 Galasko GI; Barnes SC; Collinson P et al. what is the most cost-effective strategy to screen for left ventricular systolic dysfunction: natriuretic peptides, the electrocardiogram, hand-held echocardiography, traditional echocardiography, or their combination? Eur Heart J 2006; 27:193. Version 2 Date: October 2008 Status: Final Author Dr Mary Webb Page 18 of 20 Intended audience National Public Health Service Appendix 1 Brain natriuretic peptide Main search strategy The facility available on the HOWIS website to search simultaneously across multiple databases was used. Ovid Medline, Embase, Cochrane Database of Systematic Reviews, ACP Journal Club EBM reviews; Database of Abstracts of Reviews of Effects; British Nursing Index and Cinahl, were searched Search terms included subject headings and text words based on: natriuretic peptide, brain/ 2. bnp.mp. [mp=title, original title, abstract, name of substance word, subject heading word];3. nt-probnp.mp; brain-type natriuretic peptide.mp; probnp.mp; natriuretic factor; natriuretic peptide type-b.mp; type-b natriuretic peptide.mp; ventricular natriuretic peptide; heart failure.mp. [mp=title, original title, abstract, name of substance word; exp heart failure; exp myocardial infarction; exp dyspnoea; exp coronary heart disease; exp hypertension The search terms meta.ab; synthesis.ab; literature.ab; randomized.hw; published.ab; meta-analysis pt; trials.hw; controlled.hw; medline.ab; selection.ab; sources.ab; trials.ab; review.ab; review.pt; articles.ab; reviewed.ab were used to retrieve RCTs, metanalyses and systematic reviews from Medline. Appendix 2 High level search strategy Agency for Healthcare Research and Quality Chronic Care (AHRQ) Agency for Quality in Medicine (AZQ) Canadian Coordinating Office for Health Technology Assessment (CCOHTA) Centre for Health Services Research - Population and Health Sciences - University of Newcastle Centre for Reviews & Dissemination Clinical Evidence Department of Health Effective Practice & Organisation of Care Group Guidelines International Network Google Google scholar Health Evidence Bulletin Wales Health Management Information Consortium Health Technology Assessment Programme Kings Fund National Assembly for Wales National Library for Health ( NLH) – Cardiovascular Specialist Library National Guideline Clearinghouse National Institute for Health and Clinical Excellence National Public Health Service for Wales NHS Centre for Reviews and Dissemination NHS Improvement Agency Scottish Intercollegiate Guidelines Network (SIGN) SUMSearch Turning Research Into Practice (TRIP) Database UpToDate Version 2 Author Dr Mary Webb Date: October 2008 Page 19 of 20 Status: Final Intended audience National Public Health Service Brain natriuretic peptide Appendix 3 Evidence levels and quality grading (modified from NICE Guideline Methodology Manual) ref 7 Level of Evidence 1++ 1+ 12++ 2+ 2- 3 4 Type of evidence High-quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias Well-conducted meta-analyses, systematic reviews of RCTs,or RCTs with a low risk of bias Meta-analyses, systematic reviews of RCTs, or RCTs with a high risk of bias High-quality systematic reviews of case– control or cohort studies. High-quality case–control or cohort studies with a very low risk of confounding, bias, or chance and a high probability that the relationship is causal Well-conducted case–control or cohort studies with a low risk of confounding, bias, or chance and a moderate probability that the relationship is causal Case–control or cohort studies with a high risk of confounding bias, or chance and a significant risk that the relationship is not causal Non-analytic studies (for example, case reports, case series) Expert opinion, formal consensus Quality grading ++ = good quality + = fair +/- = fair to poor - = poor Version 2 Author Dr Mary Webb Date: October 2008 Page 20 of 20 Status: Final Intended audience