Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Artificial heart valve wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Echocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
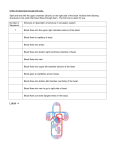
Cross-sectional Echocardiographic Diagnosis and Subclassification of Univentricular Hearts: Imaging Studies of Atrioventricular Valves, Septal Structures and Rudimentary Outflow Chambers DAVID J. SAHN, M.D., JOYCE R. HARDER, M.D., ROBERT M. FREEDOM, M.D., WALTER J. DUNCAN, M.D., RICHARD D. ROWE, M.D., HUGH D. ALLEN, M.D., LILLIAM VALDES-CRUZ, M.D., AND STANLEY J. GOLDBERG, M.D. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 SUMMARY We reviewed anatomic observations (surgical or autopsy), angiograms and echocardiograms from 44 patients with documented univentricular hearts. Thirty-three patients had univentricular heart of left ventricular type with an outflow or rudimentary chamber. Five had univentricular heart of right ventricular type, and six had univentricular heart of indeterminate types without a rudimentary chamber. Univentricular heart was correctly diagnosed by two-dimensional echocardiography in all but two of the 44 patients, including 25 of 27 double-inlet univentricular hearts, all five with absent left and all 12 with absent right atrioventricular connection. One of the two blind trabecular pouches was missed on echocardiography; the other was not seen on the angiogram but was present at autopsy. In 30 of 33 patients, univentricular heart of left ventricular type was correctly identified by imaging an anterosuperior and leftward or rightward outlet chamber, and in four of five patients with univentricular heart of right ventricular type, the anomaly was correctly identified by imaging the inferior and posterior position of the rudimentary outflow chamber near the crux of the heart. Two-dimensional echocardiography provides detailed analysis of atrioventricular connections, main chamber morphology, and rudimentary chamber size and position for noninvasive diagnosis and anatomic subclassification of univentricular hearts. IMPROVEMENTS in surgical management of congenital heart disease have made available procedures for palliation of some very complex heart malformations. The surgical septation procedures for patients with univentricular hearts are no longer widely practiced,' but the modified Fontan approach2 appears to provide satisfactory functional results in some of these patients. Planning for such procedures requires detailed and accurate delineation of atrioventricular valve structure, outflow chamber morphology, and thorough hemodynamic evaluation of patients who may be candidates for these procedures. While dispute continues over appropriate subclassification and nomenclature for these disorders, a generally acceptable subclassification of univentricular heart or single ventricle has evolved over the past 10 years.3'8 M-mode echocardiography has allowed, to some extent, noninvasive diagnosis of univentricular hearts, especially those with two atrioventricular inlets.9' 10 The accuracy of diagnosis is improved if M-mode is combined with echocardiographic contrast techniques. " II Preliminary reports and abstract reports of small series suggest that two-dimensional echocardiography has even greater potential for noninvasive delineation of univentricular heart and may provide information complementary to angiography, especially with regard to delineation of atrioventricular valve morphology and the position and size of rudimentary chambers. 1316 Improvements in resolution of two-dimensional echocardiographic systems and development of new examination planes have promised new capabilities for detailed delineation of anatomy. Accordingly, we combined and reviewed two-dimensional echocardiographic imaging data, anatomic observations, and angiographic information from a series of 44 patients. All had been examined with a predetermined two-dimensional echocardiographic imaging protocol at the University of Arizona Health Sciences Center in Tucson, Arizona, The Hospital for Sick Children in Toronto, Ontario, Canada, or at Green Lane Hospital in Auckland, New Zealand, to assess the capabilities of twodimensional echocardiography for diagnosing and subclassifying univentricular heart. Materials and Methods Anatomic Definitions The term "univentricular heart" is used in this paper interchangeably with the term "single ventricle." The term "main chamber" is used to define the large chamber receiving the major atrioventricular valve inflow. "Outlet" and "rudimentary' chamber refer to chambers receiving either no direct atrioventricular valve inflow or only a minimal commitment of an overriding valve. The term "outlet chamber" refers to rudimentary chambers giving rise to a great artery, and the term "blind trabecular pouch" was used for rudimentary chambers with no atrioventricular valve inflow and no great vessel arising from them. As defined by Anderson et al.,8 univentricular heart of left ventricular type is characterized primarily by its main chamber of left ventricular morphology and by a rudimentary chamber of right ventricular morphology arising superior to and at some distance from the crux of the heart. The external cardiac marker of the crux of From the Department of Pediatrics, University of Arizona Health Sciences Center, Tucson, Arizona, and the Cardiology Department, Hospital for Sick Children, Toronto, Ontario, Canada. Address for correspondence: David J. Sahn, M.D., Department of Pediatrics, University of Arizona Health Sciences Center, Tucson, Arizona 85724. Received September 1, 1981; revision accepted April 23, 1982. Circulation 66, No. 5, 1982. 1070 2-D ECHO IN SINGLE VENTRICLE/Sahn et al. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 the heart is the atrioventricular sulcus and the internal marker of the crux is the junction between the two atrioventricular valves, that is, the central fibrous body. The main chamber in univentricular heart of left ventricular type is, in general, smoothly trabeculated. Although Van Praagh et al. 17 pointed out the variability of outlet chamber size in single ventricle of left ventricular type as a spectrum of development of the anterior septation, our working definition of left ventricular type included the majority of our anatomic angiographic and echocardiographic observations. Univentricular heart of right ventricular type is characterized by a rudimentary chamber usually closely related to the crux of the heart and by a main chamber having right ventricular morphology and a prominent moderator band or trabeculae septomarginalis. While some controversy still exists about univentricular heart of right ventricular type and possible inclusion of variants of hypoplastic left heart, all our patients in this category had two atrioventricular valves committed to the main chamber and the two with blind trabecular pouches had double-outlet main chamber. The term "6univentricular heart of indeterminate type" was applied to hearts lacking an outlet chamber either angiographically, echocardiographically or under direct observation and usually having intermediately coarse trabeculation. Van Praagh et al. 17 considered some of these hearts without outlet chambers to be single ventricles of left ventricular type, but the three hearts in this category that we examined appeared anatomically to be closer to undifferentiated in morphology. The above anatomic definitions were also used in the angiographic and echocardiographic evaluations and classification. Patient Population Forty-four patients, ages 4 days to 19 years, with angiographically, surgically or pathologically diagnosed univentricular heart, constituted the patient population. Twenty-eight patients underwent two-dimensional echocardiographic examination during admission for their first catheterization and before angiography. Sixteen underwent two-dimensional echocardiography after their most recent angiographic examination. All patients underwent angiography. In four patients, the cardiac anatomy was verified at surgery and in nine at autopsy. In four patients, the diagnosis of univentricular heart and in one patient, the diagnosis of an absent right atrioventricular connection was missed angiographically at least once. Thirty-three patients had univentricular heart of left ventricular type and a rudimentary chamber (group A). Five of these patients had an absent left atrioventricular connection, and 12 had an absent right atrioventricular connection. In four patients with univentricular heart of left ventricular type (two with absent right atrioventricular connection and two with two atrioventricular valves), the cardiac anatomy was confirmed at autopsy. In four patients, including three with univentricular heart of left ventricular type and absent right atrioven- 1071 tricular connection and one with two atrioventricular connections, the cardiac anomalies were documented at surgery. Five patients had univentricular heart of right ventricular type (group B), three with a rudimentary outflow chamber and two with a blind trabecular chamber of left ventricular type that did not give rise to a great artery. All group B patients had two atrioventricular valves. In two group B patients, univentricular heart of right ventricular type was confirmed at autopsy. Six patients (group C) had a univentricular heart of indeterminate type; no rudimentary chamber was demonstrated angiographically, by echocardiography, or in the three patients whose hearts were examined by autopsy. Two of these patients had a poorly formed common atrioventricular valve at postmortem examination and situs ambiguus. Twenty-nine of 33 patients with univentricular heart of left ventricular type had transposition of the great arteries, 16 with a left-sided anterior aorta and 13 with a right-sided anterior aorta. All patients with univentricular hearts of right ventricular or indeterminate type had transposition. Nonetheless, because two-dimensional echocardiographic methods for defining great artery relationships and for noninvasive diagnosis of transposition have been well described"'20 and because most patients with univentricular hearts have transposition, great artery orientation and its evaluation were not an emphasis of this study and will not be further discussed. Echocardiographic Methods All patients were studied supine and unsedated. We used a range-focused phased-array Toshiba SSH 1OA with 2.4-MHz PS 24A-1 transducer, which has increased damping for improved axial resolution, a 3.5MHz dynamically focused phased-array ultrasonograph, a prototype developed by the General Electric Corporate Research and Development Center, or a 3.5-MHz mechanical sector scanner (Advanced Technology Laboratories, Mark III). Various echocardiographic views were used from parasternal, apical, and subcostal windows. Examinations usually started with a long-axis view in an attempt to demonstrate a right ventricular cavity. However, if two atrioventricular valves were seen within one cavity, or if single ventricle was suspected because the anterior chamber was small or absent, the transducer was immediately rotated to a short-axis view at the level of the atrioventricular valves to delineate the number of atrioventricular valves and confirm the absence of septation. Atrioventricular valve morphology was then studied in a view equivalent to the apical four-chamber view, with the transducer placed at the cardiac apex. A subcostal four-chamber view was the only adequate "fourchamber" view obtainable in eight patients who had meso- or dextrocardia (who were usually more difficult to image), although subcostal imaging was performed and apical imaging attempted in all patients. The " four-chamber" view was most useful for defining the number of atrioventricular valves, the papillary muscle CIRCULATION 1072 Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 relationships and the relationships of atrioventricular valves to inferior rudimentary chambers. Both the short-axis plane near the level of the great arteries or near the atrioventricular junction and subcostal planes were used to define the position and size of the rudimentary chamber. In performing and reviewing these studies, we attempted not only to diagnose univentricular heart, but also to subclassify atrioventricular connections, to identify the position and anatomic relationships of the rudimentary chamber and the outlet foramen, and to identify anatomic aspects of main-chamber morphology and the arrangement of papillary muscles, which we hoped would allow a complete subclassification of univentricular heart.8 Studies were not evaluated for specific associated abnorrnalities, including straddling vs overriding atrioventricular valves, great artery malpositions (transposition, double outlet), and stenosis or atresia of semilunar valves. Our difficulties in quantifying ventricular septal defect size by echo compared with surgical observations18 discouraged us from attempting to evaluate the possibility of outlet foramen stenosis. Results Diagnosis of Univentricular Heart and Atrioventricular Valve Morphology A combination of observations was used to diagnose univentricular heart. These included the number of atrioventricular valves, the position of the atrioventricular valves within the main chamber and separated from the rudimentary chamber, and failure to image a definable inlet septum between the atrioventricular valves or near the apex of the heart. Univentricular heart was correctly diagnosed by two-dimensional echocardiography in 42 of the 44 patients. Two patients misdiagnosed early in the series (1976) had double-inlet univentricular heart of left ventricular type, but with prominent posterior papillary muscle ridges that were mistaken for posterior septation and outflow chambers that were missed on the echocardiogram. In recent studies, attempts to view the ventricle from the true apex and visualize chordal attachments to the papillary muscles and improvements in our ability to identify the posterior medial muscle bundle and rudimentary chambers have avoided this confusion. Vnl 66 No 5, NOVEMBER 1982 FIGURE 1. An apical four-chamber view shows double-inlet single ventricle (SV) with left and right atrioventricular valves (RAV, LAV) as well as a papillary muscle structure (P) related most closely to the left AV valve. The atrial septum appears intact. Inf = inferior; Sup = superior; R - right; L = left. respond to what Rigby et al.2" called "absent atrioventricular connection" was defined echocardiographically by a bar of bright echoes marking the position of what appeared to be the invaginated atrioventricular groove between the atrium on the affected side and the main chamber (fig. 3A). The other, more suggestive of what Rigby et al. called "imperforate membrane,"'2 showed a bright echo between the atrium and main chamber that was thin and mobile when viewed in real time (fig. 3B). In all 12 patients in whom an absent or imperforate right-sided atrioventricular connection was identified angiographically, the anomaly was also identified by two-dimensional echocardiography, as were all five cases of absent left atrioventricular con- Atrioventricular Valve Imaging The two-dimensional echocardiogram correctly predicted 25 of the 27 patients with double-inlet main chamber. In the two early patients, as mentioned above, the univentricular heart was erroneously diagnosed as a huge ventricular septal defect; nonetheless, in each of these two patients, two atrioventricular valves were visualized. Figure 1 shows an apical image of a univentricular heart with two atrioventricular valves. The short-axis view (fig. 2) was also used to define the two atrioventricular valve orifices. Our twodimensional echocardiographic images suggested two types of absent connection. The first, which may cor- FIGURE 2. Short-axis view shows two atrioventricular valves (a right-sided atrioventricular valve [R. AV], and a left-sided atrioventricular valve [L. AV]) within a single ventricular cavity (SV). A portion of the posterior medial muscle bundle (pmm) is seen between the two atrioventricular valve orifices. ANT anterior; POST posterior; R right; L - left. = = 2-D ECHO IN SINGLE VENTRICLE/Sahn et al. nection (fig. 3C). In two patients with univentricular heart of right ventricular type, slight overriding of an atrioventricular valve toward the rudimentary chamber was seen echocardiographically; in one, this finding was verified at autopsy. A common atrioventricular valve with poor separation of leaflet components into two atrioventricular valves (most evident in real time) was diagnosed echocardiographically in two group C patients with univentricular heart of indeterminate type and confirmed pathologically in both. In two of the four patients in whom univentricular heart was not diagnosed from an angiogram. the diag- 1073 nosis could be made on review of the same angiogram after study of the two-dimensional echocardiogram. In the other two, the diagnosis was correctly made on a subsequent angiographic study before two-dimensional echocardiography was available at the institution where the patient was receiving cardiac care. In one patient, the diagnosis of an absent right atrioventricular connection was missed angiographically, correctly made on two-dimensional echocardiography, and confirmed pathologically. Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Imaging of Rudimentary Chambers and Subclassification of Main Chambers Thirty-four of 36 rudimentary chambers giving rise to a great artery were identified by two-dimensional echocardiography in short-axis and subcostal views. Thirty-one of 33 superiorly oriented rudimentary chambers in group A patients, with univentricular heart of left ventricular type, were imaged. The two rudimentary chambers that were missed were in the same two patients in whom univentricular heart was not diagnosed echocardiographically. In our recent patients, the suggestion of univentricular heart has prompted an exhaustive search for the rudimentary chamber. All three rudimentary chambers of left ventricular type giving rise to a great artery in group B patients were identified echocardiographically. Group A A superiorly located outlet chamber was imaged in 31 of 33 group A patients and fulfilled the major criterion for subclassification as univentricular heart of left ventricular type. Twenty-seven of these 31 outlet chambers were imaged in the short-axis view and 24 were imaged in subcostal views. Echocardiograms of the rudimentary chambers in these patients showed details of the trabecular septum between the inferior portion of the rudimentary chamber and the main chamber, the outlet foramen between the main chamber and the rudimentary chamber, and the conal or outlet septum between the great arteries (figs. 4 and 5). Echocardiographic demonstration of the outlet foraFIGURE 3. (A) A bright bar of invaginated atrioventricular sulcus tissue or atrioventricular ridge (abs. c.) sits between the atrium and the small rudimentary chamber (RC) in this patient with a single ventricle with one patent left atrioventricular valve (L. AV). The absent right atrioventricular connection partially overrides the rudimentary chamber and is also related to the main chamber. The access into the rudimentary chamber between the absent connection and the septum (S) has also been imaged. (B) In this patient, the imperforate atrioventricular valve (imp.) lies between the right atrium (RA) and the single ventricular cavity (SV). The bright echoes of the imperforate connection were thin and mobile in real time. An atrial septal defect (asd) is visible between the atria. LV = left atrioventricular valve; LA = left atrium. (C) in this patient, an absent left atrioventricular connection (abs. c.) with invaginated atrioventricular sulcus tissue lies between the left atrium (LA) and the single ventricle (SV). The right atrium (RA) is large. The view is in a subcostal orientation. Other abbreviations as in figure 1. CIRCULATION 1 074 VOL 66, No 5, NOVEMBER 1982 Ant Inf -Sup FIGURE 4. A long-axis view shows the posterior origin of the pulmonary artery (PA) and the anterior location and inferior extension of the outlet chamber (OC) beneath the aortic valve (Ao). The outletforamen (OF) is visible between the trabecular septum (TRAB SEPT) and the anterior wall of the pulmonary artery. SV = single ventricle; Ant - anterior; Post - posterior; Inf = inferior; Sup = superior. LONG AXIS Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 men superior to the crux of the heart above the atrioventricular valves and high on the cardiac silhouette in either a leftward anterior (16 of 17 patients correctly identified) or rightward anterior ( 15 of 16 patients correctly identified) location was a major criterion for identifying univentricular heart of left ventricular type.8 One left anterior and one right anterior outlet chamber were not seen on the echocardiogram. A second criterion used to diagnose univentricular hearts of left ventricular type was echocardiographic demonstration of the prominent posterior medial muscle bundle between the two atrioventricular valve orifices in patients with double-inlet left ventricle (fig. 2). This muscle bundle often forms a prominent ridge between the two atrioventricular valves in pathologic specimens, and was imaged in 23 of the 31 correctly diagnosed univentricular hearts of left ventricular type. becular pouches both had a double-outlet main chamber. Our method allowed correct diagnosis in four of the five group B patients. In the final patient, no outlet chamber was visualized, a blind trabecular pouch was missed on two-dimensional echocardiography, and the patient was erroneously classified as having univentricular heart of indeterminate type. In another patient in this group, the blind trabecular pouch had been imaged echocardiographically, even though it was missed angiographically, and was confirmed at autopsy. The inferior localization of blind trabecular pouches in group B patients is illustrated in figure 6. In three of the four patients in whom we correctly diagnosed univentricular heart of right ventricular type using the echocardiographic criterion of rudimentary chamber location,8 a moderator band-like structure near the apex of the major cavity (fig. 7) partially supported the papillary muscle apparatus. Group B The major criterion for diagnosing univentricular heart of right ventricular type was echocardiographic demonstration of an inferiorly placed rudimentary chamber located on the diaphragmatic or on the posterior cardiac surface near an atrioventricular valve and the crux of the heart. All patients in this group had two atrioventricular valves; the two patients with blind tra- Group C Univentricular heart of indeterminate type was diagnosed in all six patients by exclusion, in that neither rudimentary chambers nor blind trabecular pouches were found. One false-positive diagnosis of univentricular heart of indeterminate type was made in the patient with right ventricular type single ventricle in FIGURE 5. A short-axis image shows the leftward superior position of an imaged outlet chamber (OC). SV single ventricle. Other abbreviations as in figure 1. 2-D ECHO IN SINGLE VENTRICLE/Sahn et al. whom the blind trabecular pouch was missed echocardiographically. A prominent anterior ridge, sometimes called a trabecula septomarginalis ridge, has been found by pathologic examination,8 but was not identified by echocardiography in any of these patients. Echocardiographic Imaging of Trabecular Patterns The coarse trabecular pattern of the main chamber seen on direct anatomic inspection in univentricular hearts of right ventricular type5' 6. 8 and commonly seen in those of indeterminate type8 suggests the possibility of using high-resolution two-dimensional echocardio- Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 /f I/ A 1075 graphy to image trabeculations as an aid in subclassifying these ventricles. In seven of our patients with univentricular heart of left ventricular type, the trabecular pattern in the outlet chamber appeared significantly coarser than that in the main chamber. This appearance may be exaggerated by the small size of the rudimentary chamber. In two patients with univentricular heart of right ventricular type and in two patients with univentricular heart of indeterminate type, the trabeculations in the main chamber were prominent on the echocardiogram. However, in 14 other patients with univentricular heart of left ventricular type, complex FIGURE 6. (A)Long-axis view shows the posterior-inferior location of a blind trabecular pouch (TB) sitting below the atrioventricular groove in a patient with univentricular heart of right ventricular type. A single patent atrioventricular valve (avv) has been imaged in this plane. A = atrium; V = single ventricle. Other abbreviations as in figure 4. (B) Apex view shows the inferior location of a blind trabecular pouch (TP). The pouch is located inferior to both the left and right atrioventricular valves (L. AV, R. AV) and the AV sulcus and in a leftwardposteriorposition. The asterisk marks the communication between the pouch and the main chamber. Abbreviations as in figure 1. CIRCULATION 1076 FIGURE 7. An apicalfour-chamber view of single ventricle (SV) with two atrioventricular valve inlets (RAV, LAV). The suspensory apparatus of the LAV is related to a prominent horizontal muscular structure (MB) lying across the ventricular cavity. This structure corresponded to a moderator band structure at autopsy in a single ventricle of right ventricular type. Other abbreviations as in figure 4. a Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 trabecular folding and arcades of papillary muscles seen echocardiographically were easily confused with coarse trabeculation. Discussion The results of our study suggest that two-dimensional echocardiography is extremely useful for noninvasive diagnosis of univentricular heart. In most patients, it can accurately evaluate atrioventricular connections as well as the morphology of the main chamber and the outlet chamber. In these complicated patients who require evaluation of pulmonary vascular resistance, cardiac function and any complex associated malformations of venous inflow or great artery outflow before surgical decisions can be made, it is unlikely that twodimensional echocardiography can obviate the need for a cardiac catheterization. Accurate diagnosis of univentricular heart by two-dimensional echocardiography does aid in planning a hemodynamic study, and localization of outlet chambers aids in planning angiographic evaluation.6 22 Tlwo-dimensional Echocardiographic Evaluation of Univentricular Hearts We recommend the following method for two-dimensional echocardiographic evaluation of univentricular hearts. The two-dimensional echocardiographic examination should consist of attempting to define, in as many views as possible, the number of atrioventricular valves and the atrioventricular valve relationships. Definition of chordal structure helps to distinguish papillary muscle structures from true septation; shortaxis views at the level of the ventricle and apical "four-chamber" views are most useful for evaluating atrioventricular valves. VOL 66, No 5, NOVEMBER 1982 Rudimentary chambers and their septation (trabecular septum separating the rudimentary chamber from the main chamber, and conoventricular septum between the two great arteries) should be imaged. The examination technique consists of searching high on the cardiac silhouette in short-axis and subcostal planes. Also, the examiner should search the atrioventricular groove on the posterior or diaphragmatic surface of the heart for a rudimentary outflow chamber of left ventricular type or a blind trabecular pouch of left ventricular type at the crux of the heart in patients with univentricular heart of right ventricular type. The great arteries can be distinguished by two-dimensional echocardiography by defining the characteristic bifurcation of the imaged pulmonary artery, 18-20 and determining whether the arteries arise parallel to one another, as in transposition of the great arteries'8 or whether the pulmonary artery spirals normally around the aorta. Morphology in Univentricular Hearts Although we had few patients with univentricular heart of right ventricular or indeterminate type, we reached tentative conclusions regarding their identification. A superior outlet or rudimentary chamber that is high on the cardiac silhouette and not closely related to the atrioventricular valves or to the crux of the heart suggests univentricular heart of left ventricular type. These features were demonstrated echocardiographically in 31 of 33 patients in our series. Echocardiographic identification of the posterior medial muscle bundle is less reliable and less easily achieved, but also suggests univentricular heart of left ventricular type. A posterior or inferior rudimentary chamber that extends to the crux of the heart and has a low communication to the main chamber near the atrioventricular valves suggests univentricular heart of right ventricular type. Imaging of a moderator band-like structure supporting the papillary muscle apparatus was less useful for detecting univentricular heart of right ventricular type. If no outlet chamber is visualized, the examiner should verify a double-outlet main chamber or search for a missed blind trabecular pouch. All univentricular hearts of indeterminate type and some of right ventricular type have a double-outlet main chamber. The echocardiographic diagnosis of univentricular heart of indeterminate type remains a diagnosis of exclusion and requires identification of double-outlet main chamber and reassurance that a blind trabecular pouch has not been missed. Although some of these hearts without rudimentary chambers may appear to have a left ventricular morphology, 17 we believe that the echocardiogram can establish the absence of a rudimentary chamber. In this series, pathologically examined hearts that did not have a rudimentary chamber appeared closest to indeterminate in type. In conclusion, two-dimensional echocardiography can be used to define the anatomic features of univentricular heart and can aid in subclassifying univentricular heart and clarifying atrioventricular valve connec- 2-D ECHO IN SINGLE VENTRICLE/Sahn et al. tions and relationships. Our experience agrees with that of Huhta and co-workers23 and that of Rigby et al.21 Two-dimensional echocardiography is valuable not only in diagnosing these complicated disorders before catheterization, but also in clarifying aspects of anatomy that may not be clearly defined by angiographic study. 12. 13. 14. References Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 1. McGoon DC, Danielson GK, Ritter DG, Wallace RB, Maloney JD, Marcelletti C: Correction of the univentricular heart having two atrioventricular valves. J Thorac Cardiovasc Surg 74: 218, 1977 2. Gale AW, Danielson GK, McGoon DC, Mair DD: Modified Fontan operation for univentricular heart and complicated congenital lesions. J Thorac Cardiovasc Surg 78: 831, 1979 3. Lev M, Liberthson RR, Kirkpatrick JR, Eckner FAO, Arcilla RA: Single (primitive) ventricle. Circulation 39: 577, 1969 4. Van Praagh R, Ongley PA, Swan HJC: Anatomical types of single or common ventricle in man. Am J Cardiol 13: 367, 1964 5. MacCartney FJ, Partridge JB, Scott 0, Deverall PB: Common or single ventricle. An angiographic and hemodynamic study of 42 patients. Circulation 53: 543, 1976 6. Soto B, Bertranou EG, Bream PR, Souza A Jr, Bargeron LM Jr: Angiographic study of univentricular heart of right ventricular type. Circulation 60: 1325, 1979 7. Keeton BR, MacCartney FJ, Hunter S, Mortera C, Rees P, Shineboume EA, Tynan M, Wilkinson JL, Anderson RH: Univentricular heart of right ventricular type with double or common outlet. Circulation 59: 403, 1979 8. Anderson RH, Tynan M, Freedom RM, Quero-Jimenez M, MacCartney FJ, Shinebourne EA, Wilkinson JL, Becker AE: Ventricular morphology in the univentricular heart. Herz 4: 184, 1979 9. Bini RM, Bloom KR, Culham JAG, Freedom RM, Williams CM, Rowe RD: The reliability and practicality of single crystal echocardiography in the evaluation of single ventricle. Circulation 57: 269, 1978 10. Felner J, Brewer DB, Franch RH: Echocardiographic manifestations of single ventricle. Am J Cardiol 38: 80, 1976 11. Seward JB, Tajik AJ, Hagler DJ, Guiliani ER, Gau GT, Ritter DG: 15. 16. 17. 18. 19. 20. 21. 22. 23. 1077 Echocardiogram in common (single) ventricle: angiographic-anatomic correlation. Am J Cardiol 39: 217, 1977 Seward JB, Tajik AJ, Hagler DJ, Ritter DG: Contrast echocardiography in single or common ventricle. Circulation 53: 513, 1977 Picchio FM, Freedom RM, Harder JR, Moes CAF, Duncan WJ: Comprehensive assessment of atrioventricular valve morphology in single ventricle. (abstr) Am J Cardiol 45: 428, 1980 Gussenhoven WJ, de Villeneuve Jhr F, Buis-Liem TN, Becker AE: Echocardiographic criteria for univentricular hearts. (abstr #81) In Proceedings of the World Congress of Pediatric Cardiology, edited by Stone S. London, Ciba-Geigy, June 1980 Houston AB, Coleman EN: Two-dimensional echocardiography in the infant with univentricular heart and double inlet connexion. (abstr) In Proceedings of the World Congress of Pediatric Cardiology, edited by Stone S. London, June 1980 Ritter DG, Seward JB, Moodie D, Danielson GK: Univentricular heart (common ventricle): preoperative diagnosis. Hemodynamic, angiocardiographic, and echocardiographic features. Herz 4: 198, 1979 Van Praagh R, Plitt JA, Van Praagh S: Single ventricle pathology, embryology, terminology and classification. Herz 4: 113, 1979 Goldberg SJ, Allen HD, Sahn DJ: Pediatric and Adolescent Echocardiography, 2nd ed. Chicago, Year Book Medical Publishers, 1980, ch. 7, 8 Henry WL, Maron BJ, Griffith JM, Redwood DR, Epstein SE: Differential diagnosis of anomalies of the great arteries by realtime two-dimensional echocardiography. Circulation 51: 283, 1975 Bierman FZ, Williams RG: Prospective diagnosis of d-transposition of the great arteries in neonates by subxiphoid two-dimensional echocardiography. Circulation 60: 1496, 1979 Rigby ML, Anderson RH, Gibson D, Jones ODH, Joseph MC, Shineboume EA: Two-dimensional echocardiographic categorisation of the univentricular heart. Ventricular morphology, type, and mode of atrioventricular connection. Br Heart J 46: 603, 1981 Bargeron LM, Elliott LP, Soto B, Bream PR, Curry GC: Axial cineangiography in congenital heart disease. I. Concept, technical and anatomic considerations. Circulation 56: 1075, 1977 Huhta JC, Seward JB, Tajik AJ, Hagler DJ: Two-dimensional echocardiographic spectrum of univentricular heart. (abstr) Circulation 64 (suppl IV): IV- 166, 1981 Cross-sectional echocardiographic diagnosis and subclassification of univentricular hearts: imaging studies of atrioventricular valves, septal structures and rudimentary outflow chambers. D J Sahn, J R Harder, R M Freedom, W J Duncan, R D Rowe, H D Allen, L Valdes-Cruz and S J Goldberg Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017 Circulation. 1982;66:1070-1077 doi: 10.1161/01.CIR.66.5.1070 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1982 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/66/5/1070 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/