Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Aortic stenosis wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
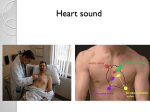
Cardiology This document is based on the handout from the “Medicine for Finals” course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations. They will complement more detailed descriptions and are not intended to be comprehensive. Topics covered in these notes • Examination • Atrial fibrillation • Mitral valve disease • Aortic valve disease • Coronary heart disease • Left ventricular failure These are the core topics of cardiology. Additional topics include: a) arrhythmias b) cardiomyopathy c) hypertensive heart disease d) the ECG There is a separate document introducing the ECG, with test-yourself examples. There are three types of cardiomyopathy- dilated (the commonest), obstructive (HOCM; causing subvalvular left ventricular outflow obstruction-differential from aortic stenosis) and restrictive (rare). Dilated cardiomyopathy would be suspected in a patient presenting with heart failure who did not have a previous history of angina or myocardial infarction. When angiograms are performed, at least 60% of such patients are found to have “silent” coronary disease (ie previously undetected) and the remainder, with normal coronary arteries, have cardiomyopathy. This may be primary or secondary (for example alcohol-related). Examination • It doesn’t matter if you miss a physical sign, so long as your technique is good • You need to look as though you have a routine, even if it is different from the examiner’s; “acceptable variation” • You need to look caring and competent • Everyone misses diastolic murmurs It is well recognised that diastolic murmurs are hard to detect, particularly with the added stress of a clinical examination. Cardiologists regularly miss diastolic murmurs too- or else arrange an echo before examining the patient so they know what they are looking for! The important point is to give yourself the best opportunity to hear them. This means lying the patient on the left hand side and listening with the bell for the low-pitched murmur of mitral stenosis. This murmur is probably the most localised of any heart sound, so “inching your way around the apex” is appropriate. Remember that to pick up low-pitched sounds the bell needs to be very lightly applied- too tight and it will convert the patient’s skin into a diaphragm. Finally, you need to sit the patient forward and listen at the end of expiration with the diaphragm applied to the left sternal edge for the high pitched early diastolic murmur of aortic regurgitation. Dr R Clarke www.askdoctorclarke.com 1 Question stop What causes the first and second heart sounds? What are the signs of endocarditis? (Hint: try to mention the ones without people’s names attached first!) What are the signs of clubbing? Heart sounds: lub dub lub dub ventricular systole Dr R Clarke www.askdoctorclarke.com diastole 2 The first and second heart sounds are caused by valve closure. The first sound is caused by closure of the mitral and tricuspid valves and the second sound by the closure of aortic and pulmonary. If heart sounds were single, they would sound “le- de…le de”. The fact that each sound is composed of two valves closing, with a slight separation between them, results in “lub dub…lub dub”). General examination • Anaemia, cyanosis, breathlessness • Hands for clubbing and splinters (the hand signs of endocarditis) • Signs of endocarditis: - 2 in the hands (clubbing and splinters) - 1 in the heart (changing murmurs) - 2 in the abdomen (splenomegaly, microscopic haematuria) - plus a few rarities (Osler, Roth, Janeway etc) Pay particular attention to the instructions. There is a no win instruction- “examine the heart”. If you start checking the hand and pulse, the examiner could say “No I said the heart”. On the other hand, if you go straight for the praecordium (anterior chest wall for apex etc), the examiner might say “Oh, don’t you bother with the pulse when you examine the heart?” If you are asked to examine the heart, you might check by saying “Normally I start with the hands and the pulse, is that what you intend me to do now?” This should make the examiner apologetic with either: “Yes, examine the cardiovascular system” or “No confine your attention to the praecordium” Stages of clubbing • Increased fluctuancy (of nail bed) • Loss of angle • Increased curvature • Drum stick appearance (expansion of terminal phalanx) Stages of Clubbing Stage 1: normal appearance and angle but increased fluctuancy of nail bed Stage 2: loss of angle between nail and nail bed Stage 3: increase curvature of nail Stage 4: expansion of terminal phalanx Drum stick appearance Dr R Clarke www.askdoctorclarke.com 3 Examination • Anaemia, cyanosis, breathlessness • Hands for clubbing and splinters • Pulse- rate, rhythm, character, volume • Collapsing pulse test • Ask for or measure blood pressure • Neck for collapsing pulse; then JVP Testing for a Collapsing Pulse JVP • Everyone finds it confusing! • The key is to think separately about the internal jugular (a pulsation) and the external jugular (a visible superficial vein) Internal jugular vein Dr R Clarke External jugular vein www.askdoctorclarke.com 4 Jugular venous pulse • Neck relaxed as internal jugular is behind sterno-mastoid which should be relaxed • Best to look from in front- you are looking for a pulsation not a visible vein • JVP usually has a “double pulsation” compared with arterial pulse- may appear to be “flickering” • If raised, check for sacral or ankle oedema The external jugular is best seen from the side, which is why many people look from the side when assessing the JVP. In fact, it is easier to see the pulsation of the internal jugular from the front. If in doubt, check both from the front and from the side- then everyone will be happy! This is probably all you need to do as a medical student or junior doctor. If you haven’t seen the JVP, it is usually reasonable to assume the central venous pressure isn’t elevated. However, some clinicians want to be sure the JVP is not high, even when they haven’t seen it, and this is where, for many of us, things start to feel confusing. If JVP not seen, 3 options to prove pressure not high • Hepato-jugular reflux- painful and many false positives and false negatives • Move patient slowly, step-by-step, into more horizontal position, noting angle at which JVP seen (laborious) • Fill and empty external jugular vein (light pressure just behind sternomastoid) The first approach involves pressing on the abdomen, which transmits pressure via the inferior vena cava to the superior vena cava. This may make the JVP become visible in the neck. Removing the abdominal pressure should then result in a return to the initial situationwith no JVP visible. The problem is that there are both false positive and false negatives with this manoeuvre and it causes significant discomfort to the patient (“The last doctor punched me in the guts and looked at my neck- I don’t understand why they do that”). The second approach is ideal for obsessionals. You move the patient into a progressively more horizontal position until the JVP becomes visible. If this is less than 45 degrees, the JVP is not elevated. This procedure involves so much wrestling with the pillow-rest that most people do not bother with it. The third approach is quick and easy and where it works can be additional good evidence that the JVP is not elevated. Light pressure with one finger behind sternomastoid at the base of the neck, will lead, after a few seconds, to filling of the external jugular vein by blood draining from the head and neck. Then the examining finger is removed and the vein should empty again. This confirms that the “manometer pressure” is not high. Compressing the vein is the equivalent of filling the manometer of a CVP device (by connecting the fluid supply to the vertical measuring tube). Removing the finger is the equivalent of turning the three-way tap to connect manometer and patient. External jugular vein • Often distended and pulsatile when internal jugular pressure raised • But false positives- may be distended if vein kinks as it pierces fascia in neck • And false negatives: not visible if low flow or situated deeply or excess fat Dr R Clarke www.askdoctorclarke.com 5 JVP: the evidence • Poor validity- correlation with right atrial pressure from cardiac catheter data • Poor reliability (McGee, S. 1998. American Heart Journal 136:10-18) • Pulsation 3cm above sternal angle in either external or internal vein is significant If anyone gives you a hard time about the JVP, it may be worth mentioning that it is one of the worst physical signs in the whole body- both in terms of reliability and validity. If it is obviously elevated, this can help, but if it is hard to assess, you may need additional evidence of heart failure from echocardiography or cardiac catheterisation. This brings us full circle and is an argument for looking once only with the patient lying relaxed at 45 degrees and to forget the three manoeuvres to prove the pressure is not high! Praecordium • Apex beat (look for scars as well as feel) • Left parasternal (for right ventricular impulse) • Aortic and pulmonary areas for thrills • Auscultation- bell and diaphragm from apex to neck • Patient on left side with bell for mitral stenosis • Patient sitting forward, at the end of expiration, with diaphragm (for aortic regurgitation) Dr R Clarke www.askdoctorclarke.com 6 Case 1: irregularly irregular pulse • What are the main two possible explanations and how would you distinguish them? • What are the causes of atrial fibrillation? • How would you assess whether atrial fibrillation is well controlled? • Why is there sometimes a difference between the pulse rate taken at the wrist and the apex? • In a patient with atrial fibrillation taking warfarin, what level of INR would you aim for? • What level would you aim for if the patient had a prosthetic valve? • What does INR stand for? Atrial fibrillation • Loss of atrial contraction reduces cardiac output- often triggers heart failure • Relative stagnation within atria gives high risk of thrombo-embolism • Fast ventricular rate may occur; loss of diastolic filling time worsens heart failure • Digoxin and verapamil slow rate by increasing delay at a-v node Dr R Clarke www.askdoctorclarke.com 7 Atrial fibrillation is probably the commonest case in clinical exams at undergraduate level. The other cause of an irregularly irregular pulse is the presence of multiple ventricular ectopic beats. This can be distinguished without an ECG because multiple ectopics should be abolished by exercise, making the pulse become regular, whereas exercise simply increases the rate in atrial fibrillation. With an ectopic ventricular focus, beats are transmitted to the ventricle only occasionally when the refractory period allows. Increasing the sinus node rate by exercising the patient will make it less likely that the ectopic focus can “drive the ventricle” Case 2: Mitral stenosis • Malar flush • Atrial fibrillation • JVP not raised • Apex beat not displaced • Apex beat tapping in quality Mitral stenosis: LUB de de • Loud first heart sound (high left atrial pressure keeps valve open until late in diastole; systole then slams it shut) • Opening snap (high pitched sound just after second heart sound- best heard at lower left sternal edge with diaphragm) LUB D e De LU B De v e n tr ic u la r s y s to le De d ia s to le Now add a mid-diastolic murmur: LUB de derrr • LUB de-derrr • Rumbling low pitched and mid-diastolic if mild stenosis • If more severe, murmur may extend later into diastole Dr R Clarke www.askdoctorclarke.com 8 L u b D e D e rrrr LU B De D e rrrr v e n tric u la r s ys to le d ia s to le Mitral stenosis: the problem • If severe, the murmur may become the dominant sound and the ear plays tricks on you! • So instead of hearing “LUB de derrr” • You hear “DurrB de de” • Particularly likely if atrial fibrillation • Try to time the murmur with the carotid pulse E a r p la y s tric k s : D u rrB d e d e D u rrrrB De De v e n tric u la r s ys to le Dr R Clarke D u rrrrB d ia s to le www.askdoctorclarke.com 9 Mitral Stenosis: x-ray appearance Aortic knuckle Pulmonary vessels Prominent left atrium Left ventricle (not enlarged in pure stenosis) Case 3: Mitral regurgitation • More likely to be in sinus rhythm • Much commoner (eg post myocardial infarction) • Quiet first heart sound • Pansystolic murmur • Radiates LOUDLY to axilla • Second heart sound not heard separately M itral regurgitation: “burrr” no g ap betw e en m urm ur and H S 2 lu b de H S 1 q uiet P ans ysto lic m urm ur Dr R Clarke www.askdoctorclarke.com diastole 10 Case 4: Aortic regurgitation • Collapsing pulse (Corrigan’s pulse) • Collapsing pulse in the neck (Corrigan’s sign) • JVP not raised • Apex beat displaced • Diastolic murmur follows second sound Aortic regurgitation: lub taaarr taaar lub ventricular systole diastole Causes of aortic regurgitation • Rheumatic heart disease • Luetic heart disease (tertiary syphilis weakens aortic wall, causing dilatation) • Endocarditis • Connective tissue disease (Marfans’ etc) Dr R Clarke www.askdoctorclarke.com 11 Case 5: Aortic stenosis • Slow rising pulse • Low volume pulse with low pulse pressure • JVP not elevated • Apex beat forceful but not displaced (pressure overload) • Ejection systolic murmur Aortic stenosis audible gap between mumur and HS2 lub dub second sound quiet with severe stenosis ventricular systole diastole Coronary heart disease • Draw a diagram showing the main blood supply to the myocardium Dr R Clarke www.askdoctorclarke.com 12 Left main stem Circumflex Right coronary artery Left anterior descending Myocardial infarction Left main stem Left anterior descending Left circumflex Right coronary Large anterior Anteroseptal Anterolateral Inferior V1-V6 V1-V4 1, aVL, V4-6 2, 3, aVF Pump problems Bradyarrhythmias Case 6: Angina vs MI • Pain less severe and lasts less than 20 minutes • Relieved by nitrates • No sweating, nausea, vomiting • May get nitrate headache and hypotension • No fear of impending doom (poor predictive value) Complications of MI • Sudden death on PRAED Street • P- pump failure • R- rupture of papillary muscle or septum • A- aneurysm and arrhythmias • E- embolism • D- Dressler’s syndrome Dr R Clarke www.askdoctorclarke.com 13 Investigations • Temperature chart (often slight fever day 2) • FBC, U+E (exclude anaemia; avoid low K+- arrhythmogenic) • Blood glucose; lipids (within 24hours as levels fall thereafter) • Cardiac enzymes- CPK, AST, LDH (false positives with injury, alcohol, exercise) • Troponins- myofibrillar proteins which link actin and myosin. More specific than CPK for myocardial injury. Elevated early after 6 hours, peak 24hours; remain elevated for 2 weeks; good for diagnosis of missed infarct; not for re-infarction) • CXR- for cardiac size and evidence left ventricular failure • Serial ECGs- may be normal initially, ST elevation, then q waves if transmural, later t wave inversion Acute Myocardial Infarction st elevation q waves imply a full thickness transmural infarct; without them: subendocardial Treatment options: "MORE GAS" M Morphine or diamorphine with metoclopramide IV O Oxygen- high flow unless COPD R Reassurance E Explanation G A S GTN Aspirin Streptokinase (unless contraindication- local or generalised bleeding risk, allergic problems etc) What are the signs of left ventricular failure? • Apart from basal crackles?... Dr R Clarke www.askdoctorclarke.com 14 Case 7: Acute LVF: on inspection • Patient looks acutely unwell- pale and grey • Cold clammy peripheries ? cyanosis • Frothy blood stained sputum in sputum pot • Orthopnoeic using accessory muscles • May have wheeze (cardiac asthma) Third heart sound: lub de dub lub de dub diastole ventricular systole Acute LVF • Sinus tachycardia or atrial fibrillation • Systolic hypotension • Signs of cardiomegaly (displaced apex, signs of valve disease) • Third and fourth heart sounds • Right sided or bilateral pleural effusions F ourth heart sound: le lub dub du b Le lub ventric ular systo le Dr R Clarke www.askdoctorclarke.com diastole 15 X-ray changes • Cardiomegaly • Upper lobe diversion • Diffuse mottling of lung fields • Prominent hilar shadows- bat’s wings • One bat’s wing= “pseudotumour of heart failure” - usually at right hilum • Small pleural effusions • Fluid in fissures Bat’s wings appearance in pulmonary oedema Treatment options • High dose oxygen • Treat significant arrhythmias • Intravenous diuretics • Intravenous diamorphine; if no improvement- • • Repeat diuretics Vasodilator eg isosorbide infusion ECG changes of hyperkalaemia • Low flat p waves • Broad bizarre qrs • Slurring into the st segment • Tall tented t waves Dr R Clarke www.askdoctorclarke.com 16 Low flat P wave Tall tented T waves Broad bizarre QRS Slurring into the ST segm ent Treatment of life threatening hyperkalaemia First arrange ECG monitor and access to resuscitation equipment Intravenous calcium gluconate (stabilises myocardium) Glucose and insulin (drives potassium into cells) Further options include: Cation exchange resins eg calcium resonium enema (takes several hours to work) Dialysis Dr R Clarke www.askdoctorclarke.com 17 Examination of the Cardiovascular System: Summary "Examine the heart" Clarify whether the examiner wants you to: • Examine the cardiovascular system or • Examine the praecodium or • Auscultate the heart. Remember There is acceptable variation in practice. Check if the examiner wants a running commentary. Introduce yourself and ask permission. Check the patient is comfortable, at 45 degrees with neck muscles relaxed. Routinely checking for radio-femoral delay is probably not justified. Reasonable to say you would check this later if hypertension or systolic murmur noted. General ?anaemic ?cyanosis ?breathless Hands For signs of endocarditis: ?clubbing ?splinter haemorrhages Pulse Check both radial pulses present (? AV fistula for dialysis) Then rate, rhythm, character, volume Collapsing pulse test while Looking at neck for visible collapsing pulse BP Ask for or measure BP JVP Look for pulsation behind sternomastoid Optional extras If JVP seen, gentle compression eliminates pulsation If not seen, light pressure at base of neck to fill external jugular; then release of pressure to demonstrate emptying (proves pressure not high) Praecordium Inspect Midline scar ?CABG ?valve replacement Intercostal scar at apex ?closed mitral valvotomy ? apex beat visible Palpate Aortic and pulmonary areas, left sternal edge and apex Auscultation All areas including neck; bell and diaphragm in each area Mitral area with bell and patient turned onto left side Aortic area and left sternal edge, using diaphragm with patient sitting forward at end of expiration Extras If appropriate, look for ankle and sacral oedema and auscultate lung bases Dr R Clarke www.askdoctorclarke.com 18