Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
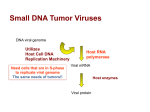
884 CONCISE COMMUNICATIONS Molecular Evidence of Simian Virus 40 Infections in Children Janet S. Butel,1 Amy S. Arrington,1 Connie Wong,1 John A. Lednicky,1 and Milton J. Finegold2 1 Division of Molecular Virology and 2Department of Pathology, Baylor College of Medicine, Houston, Texas Recent studies have detected simian virus 40 (SV40) DNA in certain human tumors and normal tissues. The significance of human infections by SV40, which was first discovered as a contaminant of poliovirus vaccines used between 1955 and 1963, remains unknown. The occurrence of SV40 infections in unselected hospitalized children was evaluated. Polymerase chain reaction and DNA sequence analyses were done on archival tissue specimens from patients positive for SV40 neutralizing antibody. SV40 DNA was identified in samples from 4 of 20 children (1 Wilms’ tumor, 3 transplanted kidney samples). Sequence variation among SV40 regulatory regions ruled out laboratory contamination of specimens. This study shows the presence of SV40 infections in pediatric patients born after 1982. Simian virus 40 (SV40) causes asymptomatic kidney infections in its natural host, the Asian macaque [1, 2], brain lesions and progressive multifocal leukoencephalopathy in immunocompromised monkeys [3–5], and tumors following experimental inoculation of neonatal hamsters [2, 6]. The virus was inadvertently introduced into millions of people by the use of SV40-contaminated vaccines between 1955 and 1963, with the major source being contaminated poliovaccines [1, 2]. There is accumulating evidence that SV40 may be associated with human tumors [2, 7, 8]. SV40-like DNA sequences have been found in ependymomas and choroid plexus tumors from pediatric patients, infectious SV40 has been isolated from a choroid plexus tumor, and SV40 DNA has been associated with osteosarcomas in adolescents [2]. Other studies have detected SV40 DNA in human pleural mesotheliomas, papillary thyroid carcinomas, normal pituitary tissue, and blood cells [2]. Sequence analysis of products amplified from four separate regions of the viral genome in several brain and bone tumors established that authentic SV40 was present in those tumors, and total nucleic acid sequencing proved that the virus isolate recovered from the choroid plexus carcinoma was a natural strain of SV40 [9]. The possibility of accidental laboratory con- tamination of samples was ruled out because DNA associated with the tumors and DNA from laboratory strains of SV40 differed in sequence both within the viral regulatory region and at the carboxy terminus of the T-antigen gene [9]. Although proof is lacking that SV40 was etiologically important in the development of those human tumors, the presence of the genomic DNA of a potent tumor virus [2, 6, 10] suggests the possibility of SV40 involvement in the genesis of some human malignancies [2]. The observed association of SV40 with tumors in young children and adolescents who were too young to have received any contaminated vaccines makes it important to address the epidemiology of SV40 infections in children. Such information will help ascertain the current frequency of infections in the pediatric population and may identify persons at risk for SV40associated disease. We studied an unselected hospital population of children in Houston. We used polymerase chain reaction (PCR) and DNA sequencing techniques to detect and identify SV40 DNA in archival tissue samples from several patients identified as having SV40 neutralization antibodies. We report here molecular evidence of SV40 infections in children born after 1982. Received 9 April 1998; revised 23 April 1999; electronically published 9 August 1999. Presented in part: 1998 Molecular Biology of Small DNA Tumor Viruses Meeting, Madison, Wisconsin, 14–19 July 1998. Human experimentation guidelines of the US Department of Health and Human Services and Baylor College of Medicine were followed in the conduct of this research. The study protocol was approved by the Institutional Review Board for Human Subject Research for Baylor College of Medicine and Affiliated Hospitals. Financial support: NIH (AI-36211, AI-07483); NASA (NCC 9-58). Reprints or correspondence: Dr. Janet S. Butel, Division of Molecular Virology, Mail Stop BCM-385, Baylor College of Medicine, One Baylor Plaza, Houston, TX 77030 ([email protected]). Materials and Methods The Journal of Infectious Diseases 1999; 180:884–7 q 1999 by the Infectious Diseases Society of America. All rights reserved. 0022-1899/1999/18003-0046$02.00 Study population. Inpatients and outpatients seen at Texas Children’s Hospital (TCH) in Houston during a 6-week period in the fall of 1995 were studied. The Department of Pathology at TCH routinely keeps surplus serum for 1 week before disposal. During November and December 1995, samples from this surplus were obtained, and SV40 neutralizing antibody was detected by using a specific plaque reduction test [11]. DNA extractions from paraffin-embedded tissues. A total of 47 archival paraffin-embedded tissue samples from patients identified as having SV40 neutralizing antibody were provided under code by the pathologist. The amounts of material available for analysis varied between samples, a factor we found important in determin- JID 1999;180 (September) SV40 Infections in Children 885 Table 1. Patient tissue specimens positive for simian virus 40 (SV40) and/or human polyomavirus BK (BKV) viral DNA sequences. Age of patient (years) Patient procedure or diagnosis 7 9 10 12 12 Renal transplant Wilms’ tumor Renal transplant Renal transplant Renal transplant a Detection of viral DNA by PCR Source of tissue BKV SV40 Confirmation of viral DNA by sequence analysis Removed kidney Tumor b Kidney, needle biopsy c Kidney, needle biopsy Peritoneum (lymphocoel removed) No No No Yes Yes Yes Yes Yes Yes No Yes Yes Yes Yes Yes NOTE. PCR, polymerase chain reaction. a Bilateral nephrectomy for focal segmental glomerulosclerosis. b Sample taken 2 months after cadaveric transplant. c Sample taken 6 months after second cadaveric transplant. ing whether meaningful PCR assays would be possible. For 22 of the 47 samples, we used an extraction kit (EX-Wax; Oncor, Gaithersburg, MD) to extract DNA from a pooled set of 5 10-mm-thick sections from each sample. These specimens were digested overnight at 507C and then extracted and precipitated according to the manufacturer’s directions. Samples were reprecipitated with sodium acetate–isopropanol and washed with 80% ethanol to remove any PCR inhibitors. All of these samples yielded DNA suitable for PCR analysis. For the remaining 25 samples, DNA was extracted from 4-mm-thick specimens using conventional methods [12]. Two to 5 sections were pooled for each specimen. These samples yielded poor-quality DNA, much of which was not suitable for PCR analysis; all were negative for viral sequences. All sample processing was done in a BL3 facility free of papovaviruses and plasmids. PCR amplification and DNA sequence analysis. The suitability of each paraffin-extracted DNA sample for PCR analysis was assessed using primers AG1 and AG2, which amplify the human A g hemoglobin gene [13]. All 22 DNA samples prepared from the larger amounts of tissue by the commercial kit were suitable for PCR. To detect SV40 DNA, primer pairs SV.for3 and SV.rev (directed at the N terminus of the T-antigen gene) and RA1 and RA2 (directed at regulatory region sequences) were used [13]. Primers BK1 and BK2 [14] were used to amplify a 354-bp product from the regulatory region of human polyomavirus BK (BKV) [15]. High-stringency PCR conditions (637C) and 65 cycles of amplification were used for both SV40 and BKV primers [13]. Only 11 of 25 samples prepared by conventional methods from smaller amounts of tissue were considered adequate for PCR analysis. Those samples were tested for the presence of SV40 DNA as above, except that low-stringency PCR conditions (annealing temperature of 527C) were used. For BKV or JC virus (JCV; another human polyomavirus), DNA, we used primers J1, J2, J3, and J4 as described for paraffin-extracted samples [13] with the modification of a low-stringency annealing temperature (547C). PCR products were cloned into a TA cloning vector (Invitrogen, Carlsbad, CA). Multiple clones were screened by PCR and then sequenced by Sequenase PCR Product Sequencing Kit (Amersham Laboratories, Arlington Heights, IL) as described [13] to confirm the presence of SV40 or BKV DNA from the human tissue samples. Results SV40 neutralizing antibody in children’s sera. We obtained 337 unselected serum samples from children seen at TCH in late 1995 and tested them for SV40 neutralizing antibody using a plaque reduction assay. Twenty samples (5.9%) were positive for SV40 antibody [11]. Detection of SV40 DNA in patient tissue samples. We reasoned that identification of SV40 DNA in tissue from a person who possessed SV40 neutralizing antibody would prove the presence of SV40 infections in children. Paraffin-embedded archival tissue samples were available from SV40 antibody–positive patients and were provided under code for molecular analysis. DNA was extracted and assayed by PCR as described in Materials and Methods. Results are described for 22 samples from 13 patients. Five of 22 paraffin-embedded tissue samples yielded virusspecific amplified products by PCR. Four samples yielded SV40 DNA products, and 2 samples had BKV DNA products; 1 sample, a biopsy from a transplanted kidney in a renal transplant patient, was positive for both viruses (table 1). The viral DNA-positive samples were from 4 renal transplant patients and a cancer patient (Wilms’ tumor). The viral DNA-negative samples included kidney biopsies taken at different times from the same patients who had a DNA-positive sample. The identity of each viral PCR product was confirmed by cloning and sequence analysis of multiple clones. The artificial SalI site present in the SV40-positive control [16] was absent from the viral sequences in patient tissues, ruling out sample contamination with the plasmid template. SV40 regulatory region sequences. The sequences of the different SV40 regulatory regions detected are diagrammed in figure 1. Archetypal versions having no duplications in the 72bp enhancer region have been recovered from infected monkeys and associated with human tumors, whereas nonarchetypal versions having some duplication in the enhancer are found less commonly in infected monkeys but very frequently as laboratory strains [4, 9]. Both archetypal and nonarchetypal structures were amplified from transplant patients (1 patient had an archetypal version, 1 had a nonarchetypal version, and another had a mixture). Nucleotide changes distinguished the tissueassociated viral DNAs from laboratory strains of SV40, ruling out laboratory contamination of specimens. Polymorphisms (C/T) at nt 5209 and nt 145 have been observed among monkey 886 Butel et al. JID 1999;180 (September) Figure 1. DNA sequence profiles of simian virus 40 (SV40) regulatory regions detected in human kidney transplant recipients. Box labeled ori represents the viral origin of DNA replication region, which spans nucleotides 5195–31; box labeled “21-bp repeats” represents the G/C-rich region between nucleotides 40 and 103; box labeled 72 represents the 72-bp sequence within the enhancer region that is duplicated in some laboratory-adapted strains (e.g., reference strain SV40-776). Nucleotide numbers are based on that of SV40-776. Shown are laboratory-adapted strain SV40-776 (GenBank accession no. J02400) and viral sequences associated with transplanted human kidneys (clone designations are on right). Both HuKi-1 (GenBank accession no. AF135792) and HuKi-2 (GenBank accession no. AF141292) were detected in the same patient; HuKi-3 (GenBank accession no. AF141290) and HuKi-4 (GenBank accession no. AF141291) were each found in different patients. Polymorphisms (C/T) at positions 5209 and 145 have been identified in previous studies. Noteworthy variations are duplication in the ori (HuKi-2) and nt substitutions (CrA) at position 5237 in both HuKi-2 and HuKi-3 and (GrA) at position 55 in HuKi-4. and human isolates of SV40 [4, 9]; amplified sequences from the transplant patients all contained a C at position 5209 and either a T or C at position 145. One unusual polynucleotide difference was detected in HuKi-2: within T-antigen binding site 1 (nt 5185–5208) [10] of the viral origin of DNA replication region (ori) (nt 5195–31), a duplication occurred, resulting in the addition of another T-antigen binding site. In both HuKi2 and HuKi-3 (recovered from 2 different patients), we observed a novel base change at nt 5237 that resulted in a loss of a restriction endonuclease (SfiI) site but did not affect the two immediately adjacent T-antigen binding sites. This particular change has not been previously detected in any viral isolate. JID 1999;180 (September) SV40 Infections in Children 887 The precise positioning of the nucleotide change and the fact that it was found in 2 independent samples argues against it being a PCR artifact. One unique substitution was observed in the 21-bp repeat region relative to SV40-776: clone HuKi-4 contained a change of G to A at position 55. To our knowledge, this nucleotide polymorphism has not been reported previously for naturally occurring SV40. This study showed (by use of molecular assays) that SV40 infections occur in children. Viral DNA sequences were detected in transplanted kidney tissue. The presence of SV40 in schoolage children makes it important to determine the source(s) of viral infection and means of transmission. Because of the potential, but still unproved, link of SV40 to childhood cancers, the development of methods to prevent such infections should be considered. Discussion Acknowledgment We describe the presence of SV40 DNA in archival tissue samples from 4 children born after 1982 who had SV40 antibodies. Molecular approaches involving PCR assays coupled with sequence analyses were used. The nucleic acid sequence studies ruled out the possibility of accidental laboratory contamination of patient samples with SV40. The finding of genetic variation in the regulatory region of viral DNA from patients (figure 1) is not unexpected, as isolates from monkeys and humans and human tumor-associated DNA have contained nucleotide substitutions and duplications in this same region [4, 5, 9]. Two unique changes, not observed in previous studies, were detected in the viral sequences amplified from transplant patient samples. One change was a duplication of nt 5197–5220 in T-antigen binding site 1 of the ori region (HuKi-2), which added another T-antigen binding motif. As binding of T-antigen to site 1 autoregulates the expression of T-antigen, this change might affect the replicative properties of a virus strain. The second change was a nucleotide substitution at position 5237 in clones (HuKi-2, HuKi-3) recovered from 2 different patients, which resulted in the loss of a restriction enzyme site. Of interest, this nucleotide separates two T-antigen binding sites; the effect of the nucleotide change on T-antigen binding to the ori region is not known. The viral sequences detected from transplant patients showed greater genetic variation than those commonly detected in human tumors [9] and are reminiscent of the mixtures of regulatory region variants of SV40 cloned from simian immunodeficiency virus–immunocompromised monkeys [4]. This may indicate that genetic variants of SV40 are more apt to be generated or to survive in a host that lacks a robust immune response. The biologic properties of these viral variants remain to be determined. Because only very small amounts of paraffin-embedded tissue were provided for analysis, it was impressive that SV40 DNA was identified from 4 different children (table 1). The viral infection in the positive tissues must have been widespread or, by chance, the tissue fragment available contained a focus of viral replication. The latter possibility is supported by our observation that kidney biopsy specimens taken at different times (but processed in parallel) from the DNA-positive patients were negative for viral sequences by PCR. We thank Antone R. Opekun for assistance in sample collection. References 1. Shah K, Nathanson N. Human exposure to SV40: review and comment. Am J Epidemiol 1976; 103:1–12. 2. Butel JS, Lednicky JA. Cell and molecular biology of simian virus 40: implications for human infections and disease. J Natl Cancer Inst 1999; 91: 119–34. 3. Ilyinskii PO, Daniel MD, Horvath CJ, Desrosiers RC. Genetic analysis of simian virus 40 from brains and kidneys of macaque monkeys. J Virol 1992; 66:6353–60. 4. Lednicky JA, Arrington AS, Stewart AR, et al. Natural isolates of simian virus 40 from immunocompromised monkeys display extensive genetic heterogeneity: new implications for polyomavirus disease. J Virol 1998; 72:3980–90. 5. Newman JS, Baskin GB, Frisque RJ. Identification of SV40 in brain, kidney and urine of healthy and SIV-infected rhesus monkeys. J Neurovirol 1998; 4:394–406. 6. Butel JS, Tevethia SS, Melnick JL. Oncogenicity and cell transformation by papovavirus SV40: the role of the viral genome. Adv Cancer Res 1972; 15:1–55. 7. Carbone M, Rizzo P, Pass HI. Simian virus 40, poliovaccines and human tumors: a review of recent developments. Oncogene 1997; 15:1877–88. 8. Geissler E. SV40 and human brain tumors. Prog Med Virol 1990; 37:211–22. 9. Stewart AR, Lednicky JA, Butel JS. Sequence analyses of human tumor–associated SV40 DNAs and SV40 viral isolates from monkeys and humans. J Neurovirol 1998; 4:182–93. 10. Cole CN. Polyomavirinae: the viruses and their replication. In: Fields BN, Knipe DM, Howley PM, et al., eds. Fields virology. Vol 2. 3rd ed. Philadelphia: Lippincott-Raven, 1996:1997–2025. 11. Butel JS, Jafar S, Wong C, et al. Evidence of SV40 infections in hospitalized children. Hum Path, in press. 12. Bergsagel DJ, Finegold MJ, Butel JS, Kupsky WJ, Garcea RL. DNA sequences similar to those of simian virus 40 in ependymomas and choroid plexus tumors of childhood. N Engl J Med 1992; 326:988–93. 13. Lednicky JA, Stewart AR, Jenkins JJ III, Finegold MJ, Butel JS. SV40 DNA in human osteosarcomas shows sequence variation among T-antigen genes. Int J Cancer 1997; 72:791–800. 14. Markowitz RB, Thompson HC, Mueller JF, Cohen JA, Dynan WS. Incidence of BK virus and JC virus viruria in human immunodeficiency virus–infected and –uninfected subjects. J Infect Dis 1993; 167:13–20. 15. Shah KV. Polyomaviruses. In: Fields BN, Knipe DM, Howley PM, et al., eds. Fields virology. 3rd ed. Vol 2. Philadelphia: Lippincott-Raven, 1996: 2027–43. 16. Lednicky JA, Butel JS. A coupled PCR and restriction digest method for the detection and analysis of the SV40 regulatory region in infected-cell lysates and clinical samples. J Virol Methods 1997; 64:1–9.