Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
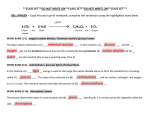
2996 pressure natriuresis response may exist in hypertension. Both mechanisms would blunt pressure natriuresis and may be important in the pathogenesis of hypertension. It is now important to extend these exciting preliminary observations to studies of tubules in the human condition. References 1. Noel J, Pouyssegur J. Hormonal regulation, pharmacology, and membrane sorting of vertebrate N a + / H + exchanger isoforms. Am J Physiol 1995; 268:C283-296 2. Orlowski J, Kandasamy RA, Shull GE. Molecular cloning of putative members of the Na/H exchanger gene family. J Biol Chem 1992; 267:9331-9339 3. Aronson PS. Ion exchangers mediating NaCl transport in the proximal tubule. Wien Klin Wochenschr 1997; 109: 435-440 4. Rosskopf D, Dusing R, Siffert W. Membrane sodium-proton exchange and primary hypertension. Hypertension 1993; 21: 607-617 5. Ng LL, Fennell DA, Dudley C. Kinetics of the human leucocyte Na + -H + antiport in essential hypertension. / Hypertens 1990; 8: 533-537 6. Davies JE, Ng LL, Ameen M, Syme PD, Aronson JK. Evidence for altered N a + / H + antiport activity in skeletal muscle cells and vascular smooth muscle cells of the spontaneously hypertensive rat. ClinSci 1991; 80: 509-516 7. Rosskopf D, Fromter E, Siffert W. Hypertensive sodium-proton exchanger phenotype persists in immortalized lymphoblasts from essential hypertensive patients. A cell culture model for human hypertension. J Clin Invest 1993; 92: 2553-2559 8. Ng LL, Sweeney FP, Siczkowski M, Davies JE, Quinn PA, Krolewski B, Krolewski AS. N a + / H + antiporter phenotype, abundance and phosphorylation of immortalized lymphoblasts from humans with hypertension. Hypertension 1995; 25: 971-977 9. Sweeney FP, Quinn PA, Ng LL. Enhanced Mitogen-activated protein kinase activity and phosphorylation of the N a + / H + exchanger isoform 1 of human lymphoblasts in hypertension. Metabolism 1997; 46: 297-302 Nephrol Dial Transplant (1998) 13: Editorial Comments 10. Siffert W, Rosskopf D, Moritz A et al. Enhanced G protein activation in immortalized lymphoblasts from patients with essential hypertension. J Clin Invest 1995; 96: 759-766 11. Siffert W, Rosskopf D, Siffert G et al. Association of a human G-protein beta3 subunit variant with hypertension. Nat Genet 1998; 18: 45-48 12. de la Sierra A, Coca A, Pare JC, Sanchez M, Vails V, UrbanoMarquez A. Erythrocyte ion fluxes in essential hypertensive patients with left ventricular hypertrophy. Circulation 1993; 88: 1628-1633 13. Ng LL, Simmons D, Frighi V, Garrido MC, Bomford J, Hockaday TDR. Leucocyte N a + / H + antiport activity in Type 1 insulin dependent diabetic patients with nephropathy. Diabetologia 1990; 33: 371-377 14. Takahashi E, Abe J, Berk BC. Angiotensin II stimulates p90" k in vascular smooth muscle cells. A potential N a + - H + exchanger kinase. Circ Res 1997; 81: 268-273 15. Good DW, George T, Watts III BA. Basolateral membrane N a + / H + exchange enhances HC0 3 " absorption in rat medullary thick ascending limb: Evidence for functional coupling between basolateral and apical membrane N a + / H + exchangers. Proc Natl Acad Sci USA 1995; 92: 12525-12529 16. Kuro M, Hanaoka K, Hiroi Y et al. Salt-sensitive hypertension in transgenic mice overexpressing Na + -proton exchanger. Circ Res 1995; 76: 148-153 17. Kawabe K, Watanabe TX, Shiono K, Sokabe H. Influence on blood pressure of renal isografts between spontaneously hypertensive and normotensive rats, utilizing the Fj hybrids. Jpn Heart J 1978; 19: 886-894 18. Guyton AD, Manning RD Jr, Hall JE, Norman R, Young DB, Pan YJ. The pathogenic role of the kidney. J Cardiovasc Pharm 1984; 6: S151-S161 19. Orosz DE, Hopfer U. Pathyphysiological consequences of changes in the coupling ratio of Na, K-ATPase for renal sodium reabsorption and its implications for hypertension. Hypertension 1996; 27: 219-227 20. Kelly MP, Quinn PA, Davies JE, Ng LL. Activity and expression of N a + / H + exchanger isoforms 1 and 3 in kidney proximal tubules of hypertensive rats. Circulation Res 1997; 80: 853-860 21. Zhang Y, Mircheff AK, Hensley CB et al. Rapid redistribution and inhibition of renal sodium transporters during acute pressure natriuresis. Am J Physiol 1996; 270: F1004-F1014 Nephrol Dial Transplant (1998) 13: 2996-2999 Glucose production by the human kidney—its importance has been underestimated Michael Stumvoll Medizinische Universitatsklinik, Abteilung fur Endokrinologie u n d Stoffwechsel, Tubingen, G e r m a n y Introduction In the post-absorptive state, glucose must be continuously delivered into the circulation in order to meet energy requirements of tissues, such as brain and red blood cells, which use only glucose as their fuel. Only liver and kidney are able to release glucose into the circulation because other tissues lack glucose6-phosphatase. Release of glucose into the circulation Correspondence and offprint requests to: Dr Michael Stumvoll, Medizinische Universitatsklinik, Otfried-Mtiller-Str. 10, D-72076 Tubingen, Germany. occurs by two processes: gluconeogenesis, the de novo synthesis of glucose from non-glucose precursors; and glycogenolysis, the breakdown of glycogen, a carbohydrate polymer formed directly from glucose or indirectly via gluconeogenesis. Both processes contribute about equally to the glucose delivered into the systemic circulation [1]. It has long been recognized that on a gram-for-gram tissue basis, the gluconeogenic capacity of the kidney exceeds that of the liver [2]. Nevertheless, based on net balance experiments finding no significant difference in arterial and renal-vein glucose concentrations in the basal state [3], the human kidney has until 2997 Nephrol Dial Transplant (1998) 13: Editorial Comments recently been regarded as contributing insignificantly to post-absorptive glucose production. Methodological considerations This traditional textbook view of the human kidney releasing insignificant amounts of glucose was based on net balance data of glucose, i.e. the mathematical product of arteriorenal venous difference of glucose concentrations (obtained through a sampling catheter in a renal vein) and renal blood flow. The net balance approach, however, does not take into consideration simultaneous release and uptake of glucose by the kidney. Thus, by merely representing the difference between uptake and release of a substrate, net balance measurements cannot evaluate the contribution of an organ to the entry and removal of a substrate from the systemic circulation. For example, with classically employed isotope dilution determination of systemic glucose flux, entry of glucose into the circulation is quantified by the dilution of the plasma glucose tracer concentration by unlabelled glucose released into the circulation. If the kidney were to take up and release glucose at equal rates, there would be no arteriorenal venous glucose difference, and net glucose balance would be zero. Nevertheless, release of unlabelled glucose into the circulation by the kidney would dilute the plasma glucose tracer concentration and contribute to the isotopic estimation of glucose entry into the circulation. Therefore a combination of net balance and isotopic techniques with measurement of substrate as well as tracer concentrations is necessary to assess individually the uptake and release of glucose by the kidney [4]. that the human kidney should account for approximately half of all gluconeogenesis and thus be as important a gluconeogenic organ as the liver. If the human kidney were a gluconeogenic organ comparable to the liver, it should play an important role in glucose homeostasis under a variety of conditions, e.g. hypoglycaemia, fasting, renal failure, diabetes mellitus and acidosis. Hormonal regulation of renal glucose release Administration of insulin to normal volunteers [6] and type I diabetics withdrawn from insulin [7] suppressed renal glucose release, which is in agreement with animal and in vitro data. Glucagon does not stimulate renal gluconeogenesis in vitro and infusion of glucagon designed to increase plasma glucagon concentrations threefold in normal volunteers had no effect on renal glucose production measured isotopically while doubling hepatic glucose production [8]. In isolated renal cortical tissue catecholamines have been shown to stimulate gluconeogenesis. In a recent study in healthy humans, designed to measure renal glucose production isotopically, adrenaline acutely increased systemic glucose production by 60%, hepatic glucose release by 50%o and renal glucose production by 100%o [5]. It is of note that in this study, infusion of adrenaline, which resulted in circulating concentrations of adrenaline similar to those observed during hypoglycaemia, caused a sustained increase in renal glucose release that by 3 h accounted for essentially all of the increased appearance of glucose in the circulation. Other factors shown to influence renal glucose release are summarized in Table 1. Uptake and release by the human kidney Renal gluconeogenic substrates An appropriate combination of renal net balance and isotopic tracer techniques was recently used in healthy, post-absorptive humans [5]. These studies showed that the human kidney simultaneously takes up and releases appreciable amounts of glucose. Renal glucose release accounted for about 25% of all glucose released into the circulation and its uptake of glucose accounted for approximately 20% of all glucose removed from the circulation. These results thus refuted textbook wisdom that the human kidney plays only a minor role in glucose homeostasis. In humans, lactate, glutamine, alanine, and glycerol are the main gluconeogenic precursors. In vitro studies have suggested lactate, pyruvate, glycerol, fructose, propionate, and certain amino acids including glutamine, glutamate, and proline as potential renal precursor candidates [9]. Studies of uptake and incorporation into glucose of potential gluconeogenic precursors by the human kidney using appropriate tracer methods have shown that lactate, glutamine and glycerol, but not alanine, a major hepatic gluconeogenic precursor accounted for over 90% of the glucose produced [10]. Renal gluconeogenesis Hypoglycaemia The normal human kidney contains negligible amounts of glycogen and kidney cells other than proximal tubules, that could theoretically store glucose, lack glucose-6-phosphatase. Thus, essentially all renal glucose release is probably due to gluconeogenesis. Gluconeogenesis accounts for about 40-50%> of systemic glucose release in postabsorptive humans. Since renal glucose release is responsible for 20-25%> of systemic glucose release under this condition, it follows logically Gluconeogenesis plays a major role in prevention and reversal of hypoglycaemia. Observations in animals that removal of liver and kidney results in more rapid and more profound hypoglycaemia than mere removal of the liver first suggested that renal glucose release is important for the prevention of hypolgycaemia and may play a role in glucose counterregulation. More recently it has been demonstrated in dogs that insulin- Nephrol Dial Transplant (1998) 13: Editorial Comments 2998 Table 1. Factors affecting renal gluconeogenesis Stimulation Inhibition Catecholamines' Glucocorticoides Aldosterone Insulin deficiency (Diabetes mellitus)* Parathyroid hormone Vitamin D Thyroxine Growth hormone Angiotensin Adrenalectomy Acid-base-balance Acidosis Alkalosis Others Prolonged fasting Exercise High-protein diet Liver failure Free fatty acids Hormones Insulin" Calcitonin Branched-chain amino acids In vitro and animal data summarized from [9] and [18]. aAvailable data in humans. induced hypoglycaemia stimulates renal glucose release while suppressing hepatic glucose release [11]. The fact that in humans adrenaline, at plasma concentrations seen during hypoglycaemia, stimulates renal glucose release [5], suggests that these findings regarding a role for the kidney in glucose counterregulation are applicable to humans. URINE TUBULE PLASMA GLUTAMINE 2NH 4 * Fasting During fasting hepatic glycogen stores become depleted and gluconeogenesis accounts for a progressively greater proportion of renal glucose release. In humans fasted for 60 h, the kidney accounts for over onethird of all glucose released into the circulation [3]. With more prolonged fasting, hepatic glucose release decreases and renal glucose release becomes even more important. 1/2 GLUCOSE 2 HC03- Fig. 1. Renal ammoniagenesis and gluconeogenesis. Diabetes mellitus Renal failure Requirements of exogenous insulin in insulindependent diabetics who develop end-stage renal failure tend to decrease. The most widely accepted explanation for this is loss of renal insulin excretion resulting in a prolonged biological half-life of the hormone [12]. Moreover, it has been observed that renal-failure patients without diabetes are prone to develop hypoglycaemia [13]. Conceivably, reduced renal gluconeogenesis may be a contributing factor to both decreased insulin requirements and increased hypoglycaemic risk in patients with and without diabetes. In addition, since the human kidney also takes up considerable amounts of glucose, loss of renal tissue could contribute to reduced glucose disposal and thus insulin resistance seen in uraemia [14]. Gluconeogenesis is considered the primary cause for increased glucose release in diabetic patients. Kidneys from experimentally diabetic animals have increased activity of gluconeogenic enzymes and increased release of glucose. Preliminary data indicate that in type I diabetic patients withdrawn overnight from insulin have increased renal glucose release [7]. These observations suggest that renal overproduction of glucose may contribute to fasting hyperglycaemia in type I diabetes. Acidosis Substantial net renal glucose release has originally been observed in patients with severe respiratory acidosis, providing the first evidence ever for glucose production by the human kidney [15]. It has been reported that Nephrol Dial Transplant (1998) 13: Editorial Comments during chronic acidosis, as much as 40% of glutamine, a major renal gluconeogenic precursor extracted by the kidney, could have been converted to glucose [16]. In vitro studies have demonstrated that acidosis increases renal production of glucose from glutamine or glutamate. During acidosis, animal kidneys extract increased amounts of glutamine (five times more than the gut) for generation of ammonia and bicarbonate. Thus increased renal glucose formation during acidosis is currently viewed as an outlet for the increased formation of a-ketoglutarate derived from glutamate and glutamine, thus conserving carbon [17] (Figure 1). Conclusions Recent studies in vivo using a combination of isotope and net balance techniques have corroborated earlier in vitro studies and animal experiments in providing evidence that the kidney plays an important role in normal carbohydrate homeostasis and under common pathologic situations such as in patients with diabetes mellitus and renal insufficiency. Further studies are needed to examine (i) regulation of renal glucose metabolism by substrate availability, insulin, and other hormones, and (ii) the contribution of the kidney to hypoglycaemia counterregulation and adaptive changes during fasting, acidosis, exercise, trauma, and other stresses associated with increased gluconeogenesis. References 1. Gerich JE. Control of glycaemia. Clin Endocrinol Metab 1993; 7: 551-586 2. Krebs HA. Renal gluconeogenesis. Adv Enzyme Reg 1963; 1: 385-400 2999 3. Bjorkman O, Felig P. Role of the kidney in the metabolism of fructose in 60-hour fasted humans. Diabetes 1982; 31: 516-520 4. Stumvoll M, Overkamp D, Gerich JE. A primer on tracer methods for the study of glucose metabolism in man. Diab Nutr Metab 1995; 8: 298-314 5. Stumvoll M, Welle S, Chintalapudi U, Perriello G, Gutierrez O, Gerich J. Uptake and release of glucose by the human kidney; postabsorptive rates and responses to epinephrine. J Clin Invest 1995; 96: 2528-2533 6. Meyer C, Dostou J, Nadkarni V, Gerich J. Effects of physiological hyperinsulinemia on systemic and renal glucose, glutamine, and free fatty acid metabolism. Diabetes 1998; 47 [Suppl 1 ]: 41 A 7. Mitrakou A, Plantanisiotis D, Vlachos L et al. Increased renal glucose production in insulin dependent diabetes (IDDM): contribution to systemic glucose appearance and effect of insulin repletion. Diabetes 996; 45 [Suppl. 2]: 33 A 8. Stumvoll M, Meyer C, Kreider M, Perriello G, Gerich J. Effects of glucagon on renal and hepatic glutamine gluconeogenesis in normal postabsorptive humans. Metabolism (in press) 9. Wirthensohn G, Guder WG. Renal substrate metabolism. Physiol Rev 1986; 66: 469-497 10. Meyer C, Stumvoll M, Welle S, Kreider M, Nair KS, Gerich J. Human kidney substrate utilization and gluconeogenesis. Diabetologia 1997; 40 [Suppl. 1]: A24 11. Cersosimo E, Molina PE, Abumrad N. Renal glucose production during insulin-induced hypoglycemia. Diabetes 1997; 46: 643-646 12. Duckworth WC. Insulin degradation, mechanisms, products, and significance. Endocr Rev 1988; 9: 319-345 13. Arem R. Hypoglycemia associated with renal failure. Endocrinol Metab Clin North Am 1989; 18: 103-121 14. DeFronzo R, Abnestrand A, Smith D, Hendler R, Wahren J. Insulin resistance in uremia. J Clin Invest 1981; 67: 563-568 15. Aber GM, Morris LO, Housley E. Gluconeogenesis by the human kidney. Nature 1966; 212: 1589-1590 16. Pitts RF, Pilkington LA, MacLeod MB, Leal-Pinto B. Metabolism of glutamine by the intact functioning kidney of the dog. J Clin Invest 1972; 51: 557-565 17. Alleyne GAO, Roobol A. Renal metabolic processes and acidbase changes. Med Clin North Am 1975; 59: 781-793 18. Schoolwerth AC, Smith BC, Culpepper RM. Renal gluconeogenesis. Miner Electrolyte Metab 1988; 14: 347-361 Nephrol Dial Transplant (1998) 13: 2999-3001 Methicillin-resistant Staphylococcus aureus (MRSA) infection in glomerulonephritis—a novel hazard emerging on the horizon Masaki Kobayashi 1 and Akio Koyama 2 d e p a r t m e n t of Nephrology, Tokyo Medical University Kasumigaura Hospital, Inashiki, and i n s t i t u t e of Clinical Medicine, University of Tsukuba, T s u k u b a , Ibaraki, J a p a n Introduction Infections with antibiotic-resistant bacteria have recently increased and infection by methicillin-resistant staphylococci (MRSA) is one typical example. Shortly Correspondence and offprint requests to: Masaki Kobayashi MD, Department of Nephrology, Tokyo Medical University Kasumigaura Hospital, 3-20-1 Chuo, Ami, Inashiki, Ibaraki 300-0395, Japan. after methicillin came into clinical use, MRSA strains were first detected in the UK in 1961 [1]. These strains were subsequently isolated in many countries including Japan. MRSA as a nosocomial pathogen has become a serious problem both from a clinical and epidemiological standpoint [2]. Staphylococci have been identified as causal agents in the genesis of glomerulonephritis. Most reports linking staphylococcal infection in glomerulonephritis emphasize two clinical settings: