Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
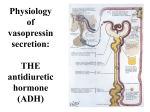
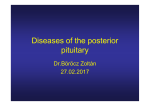
Assist prof. of Medical Physiology Excess GH Before Union of epiphysis Gigantism After Union of epiphysis Acromegaly Decreased GH In children In adults Dwarfism Loss of some body proteins Causes: 1. Hyperplasia or 2. Tumor of the somatotrop cells (adenoma) Manifestations: • The manifestations depends upon, if it occurs before or after the union of the epiphyses. A) Gigantism: ↑ed GH before the union of the epiphyses. B) Acromegaly: ↑ed GH after the union of the epiphyses or in adults Def: • Condition caused by excess GH before union of epiphysis Manifestations: 1) Marked elongation of bones but in a relative proportion. 2) Overgrowth of soft tissues e.g. the muscles & viscera. Gigantism in a 36-year-old woman. Her companions are normal. Manifestations: 3) Hyperglycemia and increased MR. 4) Hypogonadism: • Gonads and accessory sex organs remain infantile due to↓ed gonadotropins secretion GH secreting cells encroach upon the other cells. S S S S G S S S S S S T S S M S G S S M S T S S C S Pituitary tumor causes compression and atrophy of gonadotrophes Manifestations: 5) Headache due to pressure on Sella Turcica and visual disturbances (Bitemporal hemianopia) due to pressure of the growing tumor on the optic chiasma. 6) These patients are often mentally subnormal Bitemporal hemianopia Def: • Condition caused by excess GH after union of epiphysis in adults Manifestations: 1. The bones become thicker and deformed; the ms and viscera also enlarge 2. Generalized coarsening of the features due to: a. Thick skin and SC tissues. b. Enlargement of the head, hands and feet. c. Prognathism: the lower jaw enlarged & protrudes forward, and separated teeth. Spade hand Manifestations: • 3) Kyphosis due to thickening of the vertebrae. • 4) Hyperglycemia and glucosuria. • 5) Raised BMR. Manifestations: • 6) Hypogonadism. 7) Some patients have visual fields defects due to pressure of the tumor on optic chiasma. Increased intracranial tension lead to headache & vomiting. • 8) Hirsutism (increased body hair). • 9) Gynaecomastia and may be galactorrhea Treatment: • 1) Surgical: removal of tumor • 2) Medical: • Somatostatin or • Somatostatin synthetic compounds e.g. Octreotide and lanreotide Def: • Condition caused by deficiency of GH in children Manifestations: a) Short stature due to rapid closure of the epiphyses leading to proportionate reduction of all body sizes. b) The growth rate of soft tissues is reduced, but mild obesity is common. • The patient looks much younger than his age. Manifestations: c) Normal Mental growth usually. d) Low metabolic rate & episodes of hypoglycemia due to lack of insulin antagonism by GH. e) Normal Sexual maturation in cases of isolated GH deficiency. • Few dwarfs show hypogonadism and the gonads, external sexual organs and characters remain infantile Infantilism . NB: Deficiency of GH in adults has no physical signs • 1) Cretinism: Thyroid hypofunction in infants. • 2) Precocious puberty: – in cases of hypergonadism in children, which leads to early closure of the epiphyses. • 3) Gonadal dysgenesis e.g. Turner’s syndrome where an XO chromosomal pattern instead of XX or XY. • 4) Bone and metabolic diseases. • 5) Constitutional delayed growth in many cases no evident cause for stunted growth is found. Turner syndrome Excess prolactin Due to Hypothalamic dysfunctions Decreased prolactin Due to Pituitary tumors Destruction of ant. Pituitary G. Manifestations: • High prolactin inhibit GnRH and pituitary gonadotropins resulting in; • a) In women, 1. Loss of menses (amenorrhea), 2. Anovulation and infertility. 3. Galactorrhea: lactation unassociated with pregnancy 4. Decreased libido. Manifestations: • b) In men, 1) Decreased: testosterone secretion. sperm production. libido. 2) Stimulation of breast enlargement (Gynaecomastia) & Galactorrhea is rare. • Diagnosis : by a high prolactin blood level. • Treatment: by: A) Surgical removal of the tumor or B) Dopaminergic drugs to reduce prolactin secretion In women produces inability to lactate. No other clinical consequences are known. Results from destruction of the ant pituitary, leads to: – Severe deficiency of its hormones and – Atrophy of the thyroid and adrenal glands and of the gonads. Manifestations: 1. In children: lead to infantilism. – failure of growth and of sexual maturity. 2. In adults, the lack of trophic hormones results in – hypofunction of the target endocrine glands with relative hyperinsulinism. Manifestations: • a) Thyroid gland (Myxoedema) • b) Adrenal cortex (hypocorticism or ‘Addison’s disease) → leading to ms weakness, loss of weight, hypoglycaemia and dehydration. • c) The gonads (hypogonadism). Manifestations: d) Loss of weight and severe wasting of muscles (cachexia) due to: – loss of appetite (anorexia) and absence of anabolic effect of GH and androgens. e) Premature senility: – dry skin and wrinkled with early graying of hair – so the patient looks older than his age. Manifestations: f) Hypoglycaemia due to: – relative increase insulin level – lack the effects of antagonistic hormones. g) Skin colour becomes lighter due to: – anaemia and – deficiency of ACTH and beta-MSH. • Thousands of nerve fibres connect the hypothalamus, (supra-optic & para-ventricular nuclei), with the post pituitary. • The crude extract of the post lobe is called pituitrin that contains 2 hormones: 1). Antidiuretic hormone (ADH), also called vasopressin or pitressin. 2). Oxytocin (or pitocin) hormone. Synthesis and Storage: • Oxytocin & ADH, are synthesized in the hypothalamus and stored in granules with a binding protein (neurophysin) 1. Neurophysin-1 for oxytocin 2. Neurophysin-2 for antidiuretic hormone. • Granules pass down the axons through hypophyseal tracts to the nerve endings in post pituitary. • The terminal swellings of nerve endings are called ‘Herring bodies’. • When a nerve impulse is transmitted from the cell body in hypothalamus down the axon: 1. Depolarizes the terminal Herring body. 2. Ca+ influx into the Herring body induce hormone release by exostosis, and enters the adjacent capillary. Source: • Mainly from supraoptic hypothalamic nucleus Chemistry: • Peptide hormone 9 a.a. 1. Reabsorption of water from renal tubules (major action) 2. Vasoconstriction of blood vessels (in large dose) 3.As CRH on pituitary gland • Is the major action of ADH • Reabsorption of free water from the tubular fluid. • Target site of action: 1. Distal convoluted tubules 2. Collecting ducts • In large doses • ADH causes vascular smooth muscles contraction leading to: 1. Elevation of the blood pressure 2. Coronary vasoconstriction 3. Intense splanchnic vasoconstriction. • This effect used clinically in controlling, serious GIT bleeding. ADH Used in treatment of GIT bleeding • Some of ADH pass to the ant pituitary via its portal veins where it act as CRH → Increase ACTH. Regulation of vasopressin secretion. 1. Osmotic regulation 2. Blood volume 3. Other factors (stimulators and inhibitors) • Hypothalamic supraoptic nuclei contain very sensitive osmoreceptors. • Rise in plasma osmolarity (1%) → loss of intracellular water from osmoreceptor neurons → ADH secretion. • ADH produces reabsorption of free water (without electrolytes) from tubular fluid→ dilutes the plasma→ return of osmolarity to its normal value. • Normal plasma osmolarity is 290 m osm/liter. Causes of increase plasma osmolarity: 1) Dehydration (Water deprivation), either due to: Decreased water intake or Excessive loss. 2) Administration of solutes: which do not rapidly penetrate the cell membrane, such as Na+. – Substances that enter cells rapidly, as urea do not stimulate ADH secretion, because they do not produce osmotic dysequilibrium between ECF and ICF. • ADH release is stimulated by a 5% to 10% decrease in circulating blood volume, or cardiac output. – Haemorrhage decreases blood volume, – Standing & positive pressure breathing reduce cardiac output. • Hypovolemia is perceived by pressure sensors : a. Arterial baroreceptors in carotid sinus and aortic arch b. Stretch receptors in the walls of left atrium & pulmonary veins. • Pressure receptors normally maintain tonic inhibition of ADH secretion, so hypovolemia decreases the flow of these inhibitory impulses increases ADH secretion. c. Juxtaglomerular apparatus is stimulated by hypovolemia & secrete Renin which generate angiotensin II • Angiotensin II directly stimulate thirst & stimulate ADH secretion. Juxtaglomerular apparatus Renin Angiotensin II ↓ Plasma Volume (Hypovolemia) ADH secretion ↑ Plasma Volume Stretch receptors and baroreceptors 1. Inhibitors a) Diuretics b) Water loading c) Prostaglandin E d) Cortisol, and e) K+ deficiency f) Ca+ excess g) -adrenergic agonists h) Cold weather, i) Ethanol 2. Stimulators a) Sulfonylureas b) Nicotine c) opiates d) Hot weather e) -adrenergic agents f) oestrogens, & progesterone Excess Secretion Decreased Secretion Syndrome of inappropriate ADH secretion (SIADH) Diabetes Inspidus Causes: 1. Deficiency of ADH secretion (neurogenic DI) 2. Inability of the kidney to respond to ADH (nephrogenic type). Symptoms : 1) Polyuria: (urine volume reach 25 liters/day) • Due to failure of the facultative water reabsorption by the distal tubules. • Very low urine specific gravity (1001-1003). 2) Polydepsia: • drinking large amount of water due to intense thirst 2ry to polyuria. 3) Anorexia and general weakness due to loss of important substances in urine as vitamins. • Treated by: • By Administration of ADH except Nephrogenic’ type as there is a congenital defect in the renal tubules. Cause: • Increased ADH than predicted by plasma volume or tonicity Manifestations: a) Hyponatremia (serum sodium 100 - 115 mEq/L). • Results in headache, drowsiness, nausea and often coma. b) High urine osmolality. c) Slight increase in ECF volume. d) Excess renal sodium excretion despite the low serum sodium due to; • Elevated levels of atrial natriuretic factors caused by the expanded plasma volume. Source: • Mainly from paraventricular hypothalamic nucleus Chemistry: • Peptide hormone 9 a.a. Mechanism of action: • Bind to specific cell membrane receptors • Exerts its effects by increasing intracellular Ca++ content. 1. Milk Ejection 2. Uterine contraction during labour 3. Transport of sperms in female genital tract 4. Transport of sperms in male genital tract 5. Stimulation of apocrine sweat glands Mechanism: Stimulate contraction of the myoepithelial cells of the alveoli of the mammary glands. This forces milk into the ducts. This action of oxytocin is: Potentiated by oestrogen Inhibited by catecholamines. • Suckling-reflex: – Suckling stimulates touch receptors at the nipple and areola which send afferent impulses to the hypothalamus to release both oxytocin and prolactin hormones. • Lower the threshold for membrane depolarization of the myometrial ms. • This effect is: 1. Potentiated by oestrogen 2. Inhibited by progesterone. • Oxytocin has minimal effect in initiating labour • But plays an important role in the sustained post-partum uterine contractions that help to : 1. Maintain haemostasis after evacuation of the placenta, 2. Involution of the uterus after delivery. 3. In females: • Transport of the sperms into the uterus during intercourse. – By the end of intercourse, oxytocin is secreted & induce rhythmic uterine contractions which suck, the sperms into the uterus & giving the orgasm sensation. 4. In males, – help the discharge of sperms from the semineferous tubules and epididymis to vas deferens. During ejaculation 5. Stimulation of apocrine sweat secretion – at the axillae, nipples, groins and perineum that produce sex attraction in animals.