Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
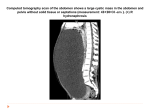
Clinico-Pathological Conference (CPC) Meet Karpagam Medical College Hospital 30-01-2015 Case History • • • • • • • • 37 yr. old female Puberty at 14 yrs Regular menstrual cycles 3-4/30 Married at 17 yrs Para 2 Live 2 MTP1 First Child -17 yrs, FTND, A&W Second Child – 19 yrs, FTND, A&W Sterilisation done . LCB – 14 yrs Chief Complaints • Increased , continuous , and painless bleeding Per vaginum - 1 month • Cycles usually regular, once in 30 days, lasts for 3-4 days • Discomfort in the lower abdomen – 1 month • Bowel and micturition habits – normal • No loss of appetite/weight • Feeling of extreme lassitude General Examination • Moderately built and nourished • Severe anemia • No jaundice or cyanosis • No significant lymphadenopathy • Vital signs -Normal Abdominal Examination • Fullness in the lower abdomen • No enlarged veins over the abdominal wall • Swelling midline, about 8-10 cm in size, uniform surface , non tender, firm to hard in consistency , Mobile – side to side • No free fluid Pelvic Examination • The exact size of uterus could not be made out • Swelling not palpable bimanually • No rectal nodes Investigations • • • • • • • • BLOOD GROUP - AB+ve Hb - 8 gm% Platelets count – 5.64 lakhs/cu.mm Serology - Normal Renal function tests – Normal TSH- 0.55 IU/ml CA- 125 = 25.5 U/ml ECG, X-ray Chest PA - Normal Ultrasound Abdomen • • • • Bulky Uterus - 9.1 x 6.6 x 6.1 cm Thickened Endometrium - 2.0 cm ?Endometrial hyperplasia/polyp Thick walled cystic area in right adnexa ?Cystic ovarian mass ?Broad ligament myxoma with degeneration Differential Diagnosis • OVARIAN CYST • FIBROID UTERUS -? BROAD LIGAMENT • ABNORMAL UTERINE BLEEDING WITH OVARIAN CYST Gross Appearance – Specimen of Total Abdominal Hysterectomy with Bilateral Salphingo-oopherectomy (11x6x5cm). – Cross Section of the uterus – unremarkable. Gross Appearance Right ovary is cystic and ms (9x9x4.5cm) Cross Section: Variegated, solid and cystic growth (9x8.5x4.5cm) Gross Appearance • Left ovary (3x2x1cm) showed multiple cysts • Both tubes were unremarkable Microscopy • Patterns - microfollicular, trabecular and macrofollicular • Proliferation malignant cells having – round to oval nuclei , scanty cytoplasm – Some of these cells have prominent nucleoli and nuclear grooving Foci showing Call-Exner bodies and hemorrhagic areas are also seen. Microscopic Picture Call-Exner bodies Microscopic Picture Differential Diagnosis • Granulosa cell tumor • Endometrioid tumor • Undifferentiated/poorly differentiated tumor Ovarian tumor staging – FIGO (2014) Stage Definition I Tumor confined to ovaries. IA Tumor limited to one ovary (capsule intact); no tumor on ovarian surface; no malignant cells in the ascites or peritoneal washings. IB Tumor limited to both ovaries (capsules intact); no tumor on ovarian surface; no malignant cells in the ascites or peritoneal washings. IC Tumor limited to one or both ovaries, with any of the following: IC1: Surgical spill intraoperatively. IC2: Capsule ruptured before surgery or tumor on ovarian surface. IC3: Malignant cells present in the ascites or peritoneal washings. II Tumor involves one or both ovaries with pelvic extension (below pelvic brim) or peritoneal cancer (Tp). IIA Extension and/or implants on the uterus and/or fallopian tubes and/or ovaries. IIB Extension to other pelvic intraperitoneal tissues. Stage Definition III Tumor involves one or both ovaries, or primary peritoneal cancer, with cytologically or histologically confirmed spread to the peritoneum outside of the pelvis and/or metastasis to the retroperitoneal lymph nodes. IIIA Metastasis to the retroperitoneal lymph nodes with or without microscopic peritoneal involvement beyond the pelvis. IIIA(i) Positive retroperitoneal lymph nodes only (cytologically or histologically proven). IIIA(ii) Metastasis >10 mm in greatest dimension. IIIA2 Microscopic extrapelvic (above the pelvic brim) peritoneal involvement with or without positive retroperitoneal lymph nodes. IIIB Macroscopic peritoneal metastases beyond the pelvic brim ≤2 cm in greatest dimension, with or without metastasis to the retroperitoneal lymph nodes. IIIC Macroscopic peritoneal metastases beyond the pelvic brim >2 cm in greatest dimension, with or without metastases to the retroperitoneal nodes.a IV Distant metastasis excluding peritoneal metastases. IVA Pleural effusion with positive cytology. IVB Metastases to extra-abdominal organs (including inguinal lymph nodes and lymph nodes outside of the abdominal cavity). Report • Uterus with chronic cervicitis and endometrium with cystoglandular hyperplasia and adenomyosis. Right ovary shows features of Adult Granulosa Cell Tumor – Stage IA (T1a Nx Mx)* • Suggested further immuno histochemical studies for alpha-inhibin, CD99 & calretinin for definite diagnosis. Review of literature • Granulosa cell tumors (GCT) were described for the first time in 1855 by Rokitansky. • characterized by a prolonged natural history and a tendency to late recurrences. • very rare ovarian malignancies; they represent <5% of all ovarian cancers. Limited data is available from India. Review of literature • Two distinct histological types—adult GCT (AGCT) and juvenile GCT (JGCT) which display different clinical and histopathological features • AGCTs are more common; usually seen in perimenopausal and postmenopausal women, peak incidence at 50–55 years • JGCTs are rare tumors, representing 5 % of all GCTs and occurring in premenarchal girls and young women • characterized by a good prognosis Review of literature • The main immunohistochemical markers expressed by these cells are vimentin, CD99 and alpha inhibin. • The serum tumor markers are estradiol, inhibin, and anti-Müllerian hormone. Review of literature • Various factors determine the prognosis. The most important prognostic variable is the stage. • Overall survival (approximately 90% at 5 years for early stage) is good, because most tumors are diagnosed early Review of literature • A special feature - appearance of recurrences long after treatment of primary tumour, mean time is 5.6 years. • Recurrences after more than 10 years are reported. TAKE HOME MESSAGE • Solid and cystic tumor with combination of yellow tissue and hemorrhage is highly suggestive of Granulosa cell tumor Thank you