Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
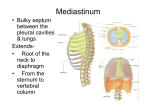
Cardiovascular Development: 1. Development of the Heart 2. Development of the Vasculature Pamela Knapp, Ph.D. Professor, Dept. Anatomy & Neurobiology MSB1 - Rm. 411 6-7570 [email protected] Early Vessel Formation A. Blood islands are first formed by proliferating yolk sac, connecting stalk, and chorion. These unite to form plexi of capillaries, some of which enlarge forming extraembryonic veins and arteries. Embryonic blood islands are formed by proliferation of visceral (splanchnic) mesoderm during mid-3rd week (~day 18). Blood islands migrate to surround the neural plate in a horse shoe-shaped cardiogenic area. Chorion (fetal placenta) Blood islands – Cardiogenic region B. Blood cells are supplied at first by the yolk sac. Starting at ~5 wks, they are supplied by a sequence of embryonic organs - liver, spleen, thymus, and, finally bone marrow. Yolk Sac ARTERIAL SYSTEM Derived from 2 structures – Aortic arches & Dorsal aortae Primitive pattern established early in 4th week Aortic arches are the arteries that supply the embryonic pharyngeal arches 5 arches (#5 is rudimentary in humans) Paired – initially identical Form in craniocaudal manner Blood flows from primitive heart, through aortic sac, and out to dorsal aortae through aortic arches Major contributions to adult arterial system made by arches 3, 4, and 6. Restructuring of aortic arches EXT. CAROTID BRACHEOCEPHALIC Art. Asc. Aorta Pulm. Trunk RIGHT 1st and 2nd LEFT arches largely regress. Critical to restructuring is breakdown of left and right DA between arches 3 and 4. 3rd arches - same fate right and left sides -remain connected at ends to aortic sac & DA -proximal parts form common carotid arteries; distal parts form portion of internal carotid artery (rest from dorsal aorta); ext carotids sprout later from 3rd arch also 4th arches - different fates on right and left side. -Left 4th arch forms midportion of the arch of the aorta. Retains connections to derivatives of aortic sac and dorsal aorta, which form proximal and distal portions of the arch of the aorta. -Right 4th arch also retains connections to derivatives of aortic sac and dorsal aorta. Forms proximal segment of right subclavian artery, (leads to more distal section formed by dorsal aorta). Aortic sac here is restructured into the bracheocephalic artery. 6th arches – different fates on right and left side. - Left proximal portion forms proximal part of left pulmonary artery. Distal left forms transient ductus arteriosus. - Right proximal forms proximal portion fo right pulmonary artery. Distal right regresses. Aortic arch restructuring affects course of recurrent laryngeal nerves Branches of vagus. Originally hook under the 6th aortic arch on both sides. Left 6th arch persists as ductus arteriosus, and then as ligamentum arteriosum. Right 6th duct regresses at distal end. 5th arches degenerate. Nerve ends up hooking under the right subclavian artery, the 4th arch derivative on the right side. In position superior to same nerve on left side. More derivatives of dorsal aortae Initial right and left dorsal aorta run the length of the embryo. They fuse just below the pharyngeal arches, creating a single dorsal aorta. Right dorsal aorta degenerates below origin of 7th intersegmental artery (branch of dorsal aorta that becomes far distal portion of right subclavian artery). Cranial paired dorsal aortae remain, forming a large part of the internal carotid arteries. The portion of the dorsal aorta located between 3rd and 4th arches is obliterated (carotid duct). The left 7th intersegmental artery becomes the left subclavian artery. It’s origin shifts cranially due to overgrowth of cephalic regions. Segmental & Intersegmental arteries These are paired, dorsal aorta derivatives that supply derivatives of the somites. Many lose their original physical connections to the aorta. Segmental arteries: Ventral: Vitelline (yolk sac) arteries fuse as the ventral dorsal aortae fuse. These will form the arteries of the dorsal mesentery of the GI tract (celiac, sup & inf mesenteric) Umbilical arteries contribute to common iliacs Lateral – give rise to renals, gonadals, and phrenics, etc. Dorsal intersegmental arteries (30+ pairs!): Cervical intersegmentals anastomose to form vertebrals 7th cervical intersegmentals contribute to subclavians Thoracic intersegmentals form the posterior intercostals Abdominal intersegmentals form lumbars Ventral segmental arteries 5th lumbar intersegments contribute to common iliacs (along with umbilical arts) Arterial Anomalies * ** VI arch derivatives Pulm. Trunk Patent ductus arteriosus* Common anomaly – often associated with hypoxia Failure of the ductus arteriosus to close after birth. DA closure is related to increased PO2 at birth. Low P02 and other factors cause production of prostaglandins that inhibit ductus muscular contraction, keeping the opening patent. Higher left side pressure after birth shunts blood through the patent DA, back to the pulmonary arteries. May respond to PG inhibitors. Coarctation of the aorta** A localized narrowing of aorta in region of DA Can be above the DA (preductal) (shown here) or below the DA (postductal). Etiology uncertain. One theory is that PO2 sensitive muscle from wall of DA is incorporated into aortic wall … contracting as PO2 rises. Double Aortic Arch: Uncommon Abnormal persistence of the right dorsal aorta between the origin of the 7th intersegmental artery and the junction with the left dorsal aorta. Result is that the trachea and esophagus are trapped inside a vascular ring. This connection should break down to form normal structures shown below EXT. CAROTID NORMAL BRACHEOCEPHALIC Art. Asc. Aorta Pulm. Trunk RIGHT LEFT VENOUS SYSTEM Posterior cardinal v. Anterior cardinal v. Umbilical v. Time: 4 weeks 3 sets of veins are returning blood to the primitive heart (rt and left horns of sinus venosus) Common cardinal v. Vitelline v. Umbilical – paired; highly oxygenated blood from fetal placenta (chorion) Vitelline – paired; originally drain the yolk sac, then its derivatives in the GI tract Cardinal – 3 pairs carry blood from the embryo proper. Anterior and posterior cardinals drain into the common cardinals. Developmen t of the Vitelline Veins Vitelline veins form a plexus of vessels around the gut before passing through the septum transversum. Right Left Yolk Sac Hepatic IVC Muscular interventricular septum The growing plexus invades the liver tissues. Blood from the left side of the abdomen drains through the plexus to the right side. Parts of the plexus form the ductus venosus – a transient structure important in shunting relatively oxygenated blood centrally and bypassing the liver tissue. Inferior portions of the right vitelline vein (below the liver) form the portal and superior mesenteric veins. Portions of the plexus contribute to the portal vein system. The midportion of the right vitelline vein forms the hepatic vein. The superior portion becomes the terminal (hepatic) part of the inferior vena cava (IVC). RIGHT LEFT Developmen t of the Umbilical Veins Both umbilical veins initially bypass the liver. They eventually make connections with hepatic sinusoids (like vitelline veins). Placenta Proximal portions of both umbilical veins, and entire RIGHT umbilical vein degenerate. The caudal, LEFT umbilical vein is the only remaining path from placenta to liver. The left umbilical vein forms an anastomosis with the ductus venosus (a transient shunt that develops in the liver, channeling blood into the nascent inferior vena cava … formerly part of the right vitelline vein). The ductus venosus is critical during fetal life. It shunts about half of the oxygenated blood from the umbilical vein directly to the right atrium via the IVC. The ductus venosus and left umbilical vein degenerate after birth to form the ligamentum venosum and ligamentum teres hepatis. Development of the Cardinal Veins Anterior and common cardinal veins: An anastomosis between anterior cardinal veins creates the left bracheocephalic vein. Cranial portions of right and left anterior cardinal veins form internal jugular veins. (External jugular veins from facial capillary plexi that connect with the internal jugular veins). The right common cardinal vein and caudal portion of the right anterior cardinal vein form the superior vena cava. Posterior cardinal veins Both are largely obliterated and replaced by 3 other venous systems: a. Subcardinal b. Sacrocardinal c. Supracardinal These venous systems form large anastomoses. Large portions degenerate during embryonic period. Subcardinal remnants include the renal, suprarenal and gonadal veins. Portions of the subcardinal, supracardinal, and sacrocardinal venous anastomoses contribute to the inferior vena cava, as well as azygous veins that drain the body wall. Venous Anomalies Largely due to persistence of structures that normally degenerate. Double Superior Vena Cava: Common defect Left anterior cardinal vein persists Result is inefficient anastomosis between left and right anterior cardinals AND persistance of a vessel that drains the coronary sinus on the left side. RIGHT LEFT Fetal and Postnatal Cirulatory Systems Be able to compare -structures that differ (ex. ductus arteriosus, ligamentum arteriosum) -bloodflow pathways Be able to explain the basis of these differences