Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
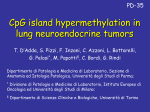
Vol. 9, 3635–3640, September 1, 2003 Clinical Cancer Research 3635 Epigenetic Inactivation of RASSF1A in Head and Neck Cancer1 Seung Myung Dong,2 Dong-Il Sun,2 Nicole E. Benoit, Igor Kuzmin, Michael I. Lerman, and David Sidransky3 moter methylation and HPV infection abrogate the same pathway in tumorigenesis. Department of Otolaryngology-Head and Neck Surgery, Head and Neck Cancer Research Division, Johns Hopkins University School of Medicine, Baltimore, Maryland 21205-2196 [S. M. D., D-I. S., N. E. B., D. S.]; Laboratory of Immunobiology, National Cancer Institute, Frederick, Maryland 21702 [I. K., M. I. L.]; and Department of Otolaryngology-Head and Neck Surgery, The Catholic University of Korea, College of Medicine, Seoul, Korea [D-I. S.] INTRODUCTION ABSTRACT Purpose: RASSF1A, a recently identified candidate tumor suppressor gene, was found to be inactivated in lung cancer and other tumor types. We sought to understand the role of RASSF1A in head and neck cancer. Experimental Design: We analyzed the status of RASSF1A and presence of high-risk human papilloma virus (HPV) in head and neck cancer squamous cell carcinoma (HNSCC) cell lines and primary tumors. We used methylation-specific PCR to detect promoter hypermethylation and direct sequence analysis to detect point mutations in primary tumors and cell lines. 5-aza-2-deoxycytidine was used to demethylate the RASSF1A promoter in cell lines. Results: Promoter methylation of RASSF1A was detected in 42.9% (3 of 7) cell lines and 15% (7 of 46) primary tumors but not in the normal control DNA. Direct sequence analysis revealed a point mutation in a cell line and another in a primary HNSCC. After treatment with 5-aza-2-deoxycytidine, re-expression and demethylation of RASSF1A gene were detected in cell lines with promoter hypermethylation. HPV DNA was detected in 34.7% (16 of 46) primary HNSCC. We found a significant inverse correlation between RASSF1A promoter methylation and HPV infection (P ⴝ 0.038). Conclusions: Our results suggest that RASSF1A is inactivated in a subset of HNSCC primary tumors. Moreover, an inverse correlation between RASSF1A and HPV supports a biological mechanism in which both RASSF1A pro- Received 10/15/02; revised 3/20/03; accepted 4/14/03. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported by NIH Grants RO1-DEO12588 entitled, “Molecular Progression Model for HNSCC” and NO1-CO-12400. 2 S. M. D. and D-I. S. contributed equally to this study. 3 To whom requests for reprints should be addressed, at Department of Otolaryngology–Head and Neck Surgery, Division of Head and Neck Cancer Research, The Johns Hopkins University School of Medicine, 818 Ross Research Building, 720 Rutland Avenue, Baltimore, MD 21205-2196. Phone: (410) 502-5153; Fax: (410) 614-1411; E-mail: [email protected]. HNSCC4 occurs in ⬎50,000 Americans each year, and the incidence of this type of tumor is expected to rise as a result of the increasing number of female and adolescent smokers. Despite the great emphasis on early diagnosis and the efforts to improve surgical and radiation treatment, ⬃50% of HNSCC patients do not survive for ⬎5 years after diagnosis (1). The growing epidemiological problem and lack of progress in head and neck oncology emphasizes the need for basic studies on the molecular biology of HNSCC. Over the past decade, molecular and cytogenetic studies have contributed significantly to the identification of genetic and epigenetic changes associated with this cancer. Tobacco and alcohol consumption are well-established risk factors of HNSCC (2). Loss of chromosomal areas and mutations in oncogenes are crucial events in tumor formation (3–7). In addition, inactivation of TSGs by promoter methylation is also common. However, a small proportion (15–20%) of HNSCC occurs in nonsmokers and nondrinkers, suggesting the presence of other risk factors. Recent epidemiological and molecular data suggest that HPV infection of the upper airway may promote head and neck tumorigenesis (8 –10). HPV-positive oropharyngeal cancers display distinct pathological molecular features as well as a different clinical course from HPV-negative oropharyngeal cancers, whose etiology is linked to smoking and drinking (9). Allelic loss on chromosomal arm 3p is common in head and neck cancers (11–15) and other cancers, including lung, kidney, breast, and bladder (14 –16). Dammann et al. (20) described the cloning and characterization of a human RAS effector homologue, RASSF1, located in the 120-kb region of minimal homozygous deletion at 3p21.3 in lung cancer (17). The RASSF1A isoform was frequently inactivated in several types of tumors (18 –20). Huang et al. (21) also provided evidence that promoter hypermethylation and allelic loss are the major mechanisms for inactivation of RASSF1A in nasopharyngeal tumorigenesis. In this study, we investigated whether RASSF1A alterations might play a role in the tumorigenesis of head and neck cancer. We also tested for HPV status based on previous evidence that HPV and RASSF1A alterations rarely occur together in cancer cell lines. 4 The abbreviations used are: HNSCC, head and neck cancer squamous cell carcinoma; MSP, methylation-specific PCR; RT-PCR, reverse transcription-PCR; HPV, human papilloma virus; LOH, loss of heterozygosity; TSG, tumor suppressor gene; GAPDH, glyceraldehydes-3-phosphate dehydrogenase; Rb, retinoblastoma gene. Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2003 American Association for Cancer Research. 3636 RASSF1A Inactivation in Head and Neck Cancer MATERIALS AND METHODS Samples. Forty-six head and neck primary tumors from the Johns Hopkins Hospital were selected to include a high proportion of oropharyngeal tumors with a high frequency of HPV positivity. Seven head and neck cancer squamous cell lines (06, 011, 013, 019, 023, 028, and 029) were also included. DNA was purified by phenol-chloroform extraction and ethanol precipitation and dissolved in distilled water as described previously (22). DNA Sequence Analysis. Samples from 26 primary tumors and seven cell lines were subjected to DNA sequencing for screen of RASSF1A gene mutation. All six exons of RASSF1A gene were examined using the 10 pairs of primers, as described previously (21). After detection of a PCR product, direct PCR sequencing reactions were performed using the Amplicycle Sequencing Kit (Perkin-Elmer, Branchburg, NJ). Bisulfite Treatment. DNA from primary tumor and cell lines was subjected to bisulfite treatment, as described previously (23). Briefly, 1 g of DNA was denatured by sodium hydroxide and modified by sodium bisulfite. DNA samples were then purified using the Wizard purification resin (Promega Corp.), again treated with sodium hydroxide, precipitated with ethanol, and resuspended in water. MSP. Genomic DNAs, modified by bisulfite treatment and sodium hydroxide, were used as a template for MSP. The RASSF1A gene primer pairs specific for methylated and unmethylated DNA were listed as described previously (21). Each PCR product was directly loaded on 4% agarose gels, stained with ethidium bromide, and visualized under UV illumination. Microsatellite Analysis of DNA. A panel of four dinucleotide microsatellite repeats PCR primers (D3S1588, D3S1621, D3S1568, and D3S3582; Research Genetics, Huntsville, AL) was used to identify losses at the 3p21.3 region. PCR conditions and criteria for LOH and homozygous deletion were described previously (22). Expression Analysis of RASSF1 Isoforms and RNA Analysis. Isoform-specific RT-PCR assays were used for analysis of RASSF1A and RASSF1C expression. Primers for RASSF1A and RASSF1C included R182 and either NF or NOX182 as described previously (19). Total RNA was isolated from the head and neck cancer cell lines by TRIzol extraction (Life Technologies, Inc., Rockville, MD). Five g of total RNA were reverse transcribed by use of Super Script First Strand cDNA kit (Invitrogen Co.). To induce expression of RASSF1A after exposure to 5-aza-2-deoxycytidine, a drug that inhibits DNA methylation, subconfluent cultures of either RASSF1Aexpressing or nonexpressing cell lines, were exposed to 1 M 5-aza-2deoxycytidine for 7 days. After isolation of total RNA using RNeasy extraction kit (Qiagen), multiplex RT-PCR was performed for GAPDH and either RASSF1A or RASSF1C. RT-PCR of GAPDH transcripts was performed with PCR primers described previously (19). RT-PCR products were separated by 4% agarose gel electrophoresis and visualized after staining with ethidium bromide. Analysis of p53. Using the Affymetrix GeneChip p53 reagent kit, genomic DNA from tumor or cell line samples was PCR amplified for p53 exons 2–11. Next, the amplified DNA Fig. 1 Expression of RASSF1A after treatment of head and neck cancer cells with 5-aza-2-deoxycytidine. 013, 019, 028 head and neck squamous carcinoma cell lines that express RASSF1C (data not shown) but not RASSF1A were grown in the presence (⫹ lanes) and absence (⫺ lanes) of 1 M 5-aza-2-deoxycytidine for 7 days. Total RNA was isolated, cDNA was prepared, and isoform-specific RT-PCR was performed for RASSF1A and GAPDH as a control. was fragmented with calf intestine alkaline phosphatase (Roche). The fragmented DNA was fluorescently end-labeled using Enzo’s BioArray Terminal Labeling Kit. The samples were hybridized to the GeneChip p53 array and washed then visualized using a GeneArray scanner. A reference DNA sample (provided in the Affymetrix kit) was also run to use as a baseline sequence for analysis. Samples read as mutated with the GeneChip p53 array were manually sequenced for confirmation. Analysis of HPV. Purified genomic DNA was amplified by PCR for the HPV-16 and HPV-18 E7 genes as well as for an internal reference gene, -globin. Oligonucleotide primers and PCR conditions were described previously (24). Statistical Analysis. Statistical analysis was performed by use of 2 and Fisher’s exact tests to test for differences between groups. All analyses were performed using SPSS Window version 9.0 (SPSS, Inc., Chicago, IL). RESULTS To investigate epigenetic silencing of RASSF1A in HNSCC, we first tested for promoter methylation in seven head and neck HNSCC cell lines (06, 011, 013, 019, 023, 028, and 029). Using MSP, 42.9% (3 of 7) of cell lines demonstrated RASSF1A methylation. To determine the precise pattern of CpG methylation within the RASSF1A CpG islands, we directly sequenced all three MSP products from the methylated cell lines. All three samples demonstrated methylation of all 16 CpG sites within the amplified fragment. RT-PCR analysis of the three HNSCC cell lines with RASSF1A methylation demonstrated complete transcriptional silencing, whereas RASSF1A expression was detected in the other four cell lines without RASSF1A methylation. To confirm that promoter hypermethylation contributes to the lack of expression of RASSF1A in the HNSCC cell lines, we assessed the effect of 5-aza-2-deoxycytidine, a drug that inhibits DNA methylation. We exposed the RASSF1A-nonexpressing HNSCC cell lines (013, 019, and 028) to 5-aza-2-deoxycytidine for 3 days and found re-expression of RASSF1A by these cell lines but little or no change in the expression of the housekeeping gene GAPDH (Fig. 1) or in the expression of the other isoform RASSF1C (data not shown). We then tested 46 HNSCC primary tumors for allelic loss using microsatellite markers, which map close to the RASSF1A gene. We found allelic loss in 43.5% (20 of 46) of the HNSCC primary tumors in at least one closely mapped marker. We then investigated the frequency of RASSF1A promoter methylation in Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2003 American Association for Cancer Research. Clinical Cancer Research 3637 Fig. 2 MSP for the detection of methylated RASSF1A 5⬘ CpG sequences in primary resected HNSCCs. Representative samples are shown. M, DNA size marker (50, 100, and 150 bp); U, results with primers specific for unmethylated sequences; M, results with primers specific for methylated sequences. MC, in vitro methylated positive control; UC, in vitro unmethylated positive control; H2O, negative control with water blanks. Each lane shows the PCR results for the methylated (#3– 42) and unmethylated (#43) sequences from HNSCCs. all 46 HNSCC primary tumors by MSP (Fig. 2). Aberrant promoter methylation of RASSF1A was found in 15% (7 of 46) primary tumors but not in the paired normal DNA (Table 1). Only three cases with RASSF1A promoter methylation demonstrated an allelic imbalance in the 3p21.3 region by microsatellite analysis. To determine whether the RASSF1A gene was altered by mutation in a subset of 26 primary tumors (including all four with RASSF1A promoter methylation and absence of LOH) and seven cell lines, we performed extensive mutational analysis for all six exons (including intron/exon boundaries) of the RASSF1A gene using direct PCR sequencing. We found two missense mutations, one mutation in a cell line and another in a primary HNSCC without evidence of promoter hypermethylation of the RASSF1A gene. The mutation was at codon 133 (GCT to TCT) that predicts Ala to Ser in the 011-cell line and at codon 281 (TTT to TCT) that predicts Phe to Ser in HNSCC primary tumor. The latter mutation was somatic, i.e., not present in the matched lymphocyte DNA. The identical mutation at codon 133 was detected previously in a breast tumor by Burbee et al. (19). We then screened for the presence of HPV DNA in these tumors by PCR for both E6 and E7 genes, 34.7% (16 of 46) of the primary tumors demonstrated the presence of HPV-16 genes, and HPV was not present in any of the cell lines. There was an inverse correlation between RASSF1A promoter methylation and the presence of HPV in the 46 primary HNSCCs (P ⫽ 0.038 by 2). We further investigated the correlation between p53 gene mutation and the presence of HPV from our data bank. Among the 46 head and neck cancers, a result of p53 sequence information analysis was available from Affymetrix p53 chip array followed by direct sequence analysis in all cases. A portion (34.8%; 16 of 46) of HNSCCs had p53 gene mutation. Among nine tumors with p53 gene mutation, only one tumor sample also harbored HPV. Although p53 mutations were found in one-third of all tumors, there was a marked difference in p53 mutation frequency between HPV-positive and -negative tumors in head and neck (P ⫽ 0.026). DISCUSSION Genetic aberrations have been investigated as markers of disease progression and/or outcome in HNSCC, including gain or loss of chromosomal regions (7, 25–27). More recently, several studies involving promoter hypermethylation have iden- tified genes such as p16, MGMT, GST-, and DAP-kinase, whose expression is down-regulated in HNSCC samples compared with normal tissue (28 –29). Mapping studies of chromosome 3 deletions provide evidence for the presence of three discrete 3p deleted regions (3p14, 3p21, and 3p24-p25) in lung and head and neck cancers (13, 15). It has been suggested that the short arm of chromosome 3 harbors several TSGs, which may be of diagnostic and therapeutic importance (12, 30). Extensive LOH studies in carcinoma of the lung, breast, cervix, kidney, and head and neck suggest that either a single TSG or a group of different ones reside on 3p and contribute to the pathophysiology of these cancers (31, 32). More recently, homozygous deletions of 3p21.3 have been reported in several breast cancer and lung cancer cell lines, and deletion may be a major mechanism of inactivation for RASSF1A in these cancers (12, 15). Ectopic expression of RASSF1A decreases in vitro colony formation, suppresses anchorage-dependent growth, and dramatically reduces tumorigenecity in vivo (17, 19). With these tumor suppression effects, the presence of a RAS association domain suggests that RASSF1A may function as an effecter molecule in the RAS-activated growth inhibition signaling pathways. Recent studies suggest that RASSF1A inhibits accumulation of native cyclin D1, and RASSF1A-induced cell cycle arrest can be relieved by ectopic expression of cyclin D1 or of other downstream activators of the G1-S phase transition (33). There is strong evidence that RASSF1A functions as a bonafide TSG that undergoes epigenetic inactivation in cancer by methylation of the CpG islands in the promoter region (16 –21, 34). We have confirmed the presence of RASSF1A methylation in 15% of primary HNSCCs and higher frequency in cell lines. After treatment of 5-aza-2-deoxycytidine in HNSCC cell lines with RASSF1A gene promoter hypermethylation, reexpression and demethylation of the promoter region of RASSF1A gene were demonstrated. Our results suggest that aberrant hypermethylation of the RASSF1A promoter region is directly responsible for transcriptional inactivation of its expression in HNSCC cell line as shown in other tumor types (18, 19). Half (50%) of primary HNSCCs showed LOH at the 3p21.3 region. These results are consistent with reports that methylation and LOH are the major loss function pathways for RASSF1A inactivation because we detected only one primary tumor with a somatic mutation. Other studies have also reported RASSF1A methylation in head and neck and other tumors and the observation that point mutations of this gene are rare (18 –21, 35–38). Inactivation in one case (primary tumor #3) by point mutation of one allele and promoter hypermethylation in the other provides additional support for a complete abrogation of RASSF1A function in tumor cells. HPV has also been implicated in the etiology of HNSCC. Recent observations suggest that patients with HPV-associated HNSCC may display a clinical course different from those of patients with HNSCC whose etiology in linked to smoking and drinking (9). HPV was detected in primary HNSCC tumors without RASSF1A promoter methylation status. This result points to a strong inverse correlation between HPV infection and RASSF1A silencing/promoter hypermethylation. This correlation could also reflect a functional role of the cellular RASSF1A and viral proteins in the G1 cell cycle check point. Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2003 American Association for Cancer Research. 3638 RASSF1A Inactivation in Head and Neck Cancer Table 1 LOH at RASSF1A 3p21.3 methylation Cell line 06 011 013 019 022 028 029 Primary tumor 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 a b HNSCC primary tumora RASSF1A mutation HPV infection p53 mutation Site nd nd nd nd nd nd nd ⫺ ⫺ ⫹ ⫹ ⫺ ⫹ ⫺ ⫺ 133, GCT(Ala) ⫺ TCT(Ser) ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ 36, CCG(Pro) ⫺ CCA(Pro)b 248, CGG(Arg) ⫺ CTG(Leu) 138, ⫺1 bp ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫹ ⫺ ⫹ ⫺ ⫹ ⫹ ⫹ ⫺ ⫺ ⫺ ⫺ ⫹ ⫹ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫹ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫹ ⫺ ⫹ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫹ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫹ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ 281, TTT(Phe) ⫺ TCT(Ser) ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ nd nd nd nd nd nd nd nd nd nd nd ⫺ nd nd nd nd nd nd nd nd nd nd nd nd nd ⫺ ⫺ ⫺ ⫹ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ ⫹ ⫺ ⫹ ⫹ ⫹ ⫹ ⫹ ⫺ ⫹ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫹ ⫹ ⫺ ⫺ ⫹ ⫹ ⫹ ⫺ Tongue 281, GAC(Asp) ⫺ GAG(Gln) Tongue 278, CCT(Pro) ⫺ GCT(Ala) Tongue ⫺ Tongue ⫺ Tongue 247, AAC(Asn) ⫺ ATC(Ile) Tongue ⫺ Tongue 342, CGA(Arg) ⫺ TGA(stop) Tongue 193, CAT(His) ⫺ CTT(Leu) Floor of mouth ⫺ Floor of mouth ⫺ Floor of mouth 220, TAT(Tyr) ⫺ TGT(Cys) Floor of mouth 272, GTG(Val) ⫺ ATG(Met) Alveolus ⫺ Alveolus ⫺ Supraglottis 146, TGG(Trp) ⫺ TGA(stop) RMT 248, CGG(Arg) ⫺ TGG(Trp) RMT/Alveolus ⫺ Hypophar, wall 243–244, ⫺3 bp Pyriform sinus ⫺ Glottic larynx ⫺ Tonsil ⫺ Tonsil ⫺ Tonsil 285, GAG(Glu) ⫺ TAG(stop) Tonsil 342, ⫺1 bp Tonsil ⫺ Tonsil ⫺ Tonsil ⫺ Tonsil ⫺ Tonsil ⫺ Tonsil ⫺ Tonsil ⫺ Tonsil ⫺ Base of tongue ⫺ Base of tongue ⫺ Base of tongue ⫺ Base of tongue 192–193, CAGCAT ⫺ CATTAT (2 aa) Base of tongue 237, ATG(Met) ⫺ ATT(Ile) Base of tongue 36, CCG(Pro) ⫺ CCA(Pro)b Base of tongue ⫺ Base of tongue ⫺ Base of tongue ⫺ Base of tongue 196, CGA(Arg) ⫺ TGA(stop) Base of tongue ⫺ Base of tongue ⫺ Base of tongue ⫺ Base of tongue Tongue Larynx Unknown Base of tongue Larynx Unknown Base of tongue ⫹, positive; ⫺, negative; nd, not detected; RMT, retromolar trigone; ALV, alveolar ridge. Possible splice site mutation, attributable to proximity to intron:exon boundary. P16, cyclin D1 (and rarely, Rb) are critical regulators of the G1 checkpoint and play important roles in the tumorigenesis of head and neck cancer. The E7 papillomavirus protein can bypass Rb family-dependent cell cycle regulation by directly inhibiting the interaction of Rb protein with E2F transcription factors and other pocket-binding proteins. H1299 and HeLa CCL2 cell lines are known to be insensitive to RASSF1A-induced cell cycle arrest. This is likely attributable to the expression of the papillomavirus E7 protein that can bypass the Rb family cell cycle checkpoint control (9). Recently, Agathanggelou et al. (20) also described the absence of RASSF1A promoter methylation in primary cervical Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2003 American Association for Cancer Research. Clinical Cancer Research 3639 cancers. Although the report did not demonstrate the presence of HPV in cervical cancers, we can postulate a low frequency of RASSF1A promoter methylation because of a high rate HPV infection in these tumors. Thus, an inverse correlation between RASSF1A and HPV in cancers may be common. There was no association between RASSF1A inactivation and p53 status. The inverse association between p53 mutations and HPV presence in head and neck cancer continues to support two parallel pathways of HNSCC development (9, 39, 40). Our results further suggest that there may be important overlapping pathways in the development of head and neck cancers between HPV and RASSF1A. Although the E6 protein inactivates p53, E7 may block Rb family-mediated cell cycle arrest in oropharyngeal tumors. Thus, RASSF1A inactivation now represents another important genetic feature of HPV-negative tumors. Our study provides evidence that promoter hypermethylation is the major mechanism for inactivation of RASSF1A in HNSCC and indicates this gene may be a key tumor suppressor target at 3p21.3. Some sites were underrepresented in our study (e.g., larynx) and could harbor a higher frequency of RASSF1A methylation. The inverse correlation between HPV infection and RASSF1A silencing in the development of head and neck cancers is based on a limited number of tumors and remains to be fully explored. REFERENCES 1. Greenlee, R. T., Hill-Harmon, M. B., Murray, T., and Thun, M. Cancer statistics, 2001. CA Cancer J. Clin., 51: 15–36, 2001. 2. Mashberg, A., Boffetta, P., Winkelman, R., and Garfinkel, L. Tobacco smoking, alcohol drinking, and cancer of the oral cavity and oropharynx among U. S. veterans. Cancer, 72: 1369 –1375, 1993. 3. Nawroz, H., van der Riet, P., Hruban, R. H., Koch, W., Ruppert, J. M., and Sidransky, D. Allelotype of head and neck squamous cell carcinoma. Cancer Res., 54: 1152–1155, 1994. 4. Sanchez-Cespedes, M., Okami, K., Cairns, P., and Sidransky, D. Molecular analysis of the candidate tumor suppressor gene ING1 in human head and neck tumors with 13q deletions. Genes Chromosomes Cancer, 7: 319 –322, 2000. 5. Lee, D. J., Koch, W. M., Yoo, G., Lango, M., Reed, A., Califano, J., Brennan, J. A., Westra, W. H., Zahurak, M., and Sidransky, D. Impact of chromosome 14q loss on survival in primary head and neck squamous cell carcinoma. Clin. Cancer Res., 3: 501–505, 1997. 6. van der Riet, P., Nawroz, H., Hruban, R. H., Corio, R., Tokino, K., Koch, W., and Sidransky, D. Frequent loss of chromosome 9p21–22 early in head and neck cancer progression. Cancer Res., 54: 1156 –1158, 1994. 7. Carey, T. E., Van Dyke, D. L., and Worsham, M. J. Nonrandom chromosome aberrations and clonal populations in head and neck cancer. Anticancer Res., 13: 2561–2567, 1993. 8. Franceschi, S., Munoz, N., Bosch, X. F., Snijders, P. J., and Walboomers, J. M. Human papillomavirus and cancers of the upper aerodigestive tract: a review of epidemiological and experimental evidence. Cancer Epidemiol. Biomark. Prev., 5: 567–575, 1996. 9. Gillison, M. L., Koch, W. M., Capone, R. B., Spafford, M., Westra, W. H., Wu, L., Zahurak, M. L., Daniel, R. W., Viglione, M., Symer, D. E., Shah, K. V., and Sidransky, D. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Inst. (Bethesda), 92: 709 –720, 2000. 10. Gillison, M. L., Koch, W. M., and Shah, K. V. Human papillomavirus in head and neck squamous cell carcinoma: are some head and neck cancers a sexually transmitted disease? Curr. Opin. Oncol., 11: 191–199, 1999. 11. Wistuba, I. I., Behrens, C., Virmani, A. K., Mele, G., Milchgrub, S., Girard, L., Fondon, J. W., III, Garner, H. R., McKay, B., Latif, F., Lerman, M. I., Lam, S., Gazdar, A. F., and Minna, J. D. High resolution chromosome 3p allelotyping of human lung cancer and preneoplastic/ preinvasive bronchial epithelium reveals multiple, discontinuous sites of 3p allele loss and three regions of frequent breakpoints. Cancer Res., 60: 1949 –1960, 2000. 12. Kok, K., Naylor, S. L., and Buys, C. H. Deletions of the short arm of chromosome 3 in solid tumors and the search for suppressor genes. Adv. Cancer Res., 71: 27–92, 1997. 13. Maestro, R., Gasparotto, D., Vukosavljevic, T., Barzan, L., Sulfaro, S., and Boiocchi, M. Three discrete regions of deletion at 3p in head and neck cancers. Cancer Res., 53: 5775–5779, 1993. 14. Alimov, A., Kost-Alimova, M., Liu, J., Li, C., Bergerheim, U., Imreh, S., Klein, G., and Zabarovsky, E. R. Combined LOH/CGH analysis proves the existence of interstitial 3p deletions in renal cell carcinoma. Oncogene, 19: 1392–1399, 2000. 15. Lerman, M. I., and Minna, J. D. The 630-kb lung cancer homozygous deletion region on human chromosome 3p21.3: identification and evaluation of the resident candidate tumor suppressor genes. The International Lung Cancer Chromosome 3p21.3 Tumor Suppressor Gene Consortium. Cancer Res., 60: 6116 – 6133, 2000. 16. Dammann, R., Yang, G., and Pfeifer, G. P. Hypermethylation of the CpG island of Ras association domain family 1A (RASSF1A), a putative tumor suppressor gene from the 3p21.3 locus, occurs in a large percentage of human breast cancers. Cancer Res., 61: 3105–3109, 2001. 17. Dammann, R., Li, C., Yoon, J. H., Chin, P. L., Bates, S., and Pfeifer, G. P. Epigenetic inactivation of a RAS association domain family protein from the lung tumour suppressor locus 3p21.3. Nat. Genet., 25: 315–319, 2000. 18. Dreijerink, K., Braga, E., Kuzmin, I., Geil, L., Duh, F. M., Angeloni, D., Zbar, B., Lerman, M. I., Stanbridge, E. J., Minna, J. D., Protopopov, A., Li, J., Kashuba, V., Klein, G., and Zabarovsky, E. R. The candidate tumor suppressor gene, RASSF1A, from human chromosome 3p21.3 is involved in kidney tumorigenesis. Proc. Natl. Acad. Sci. USA, 98: 7504 –7509, 2001. 19. Burbee, D. G., Forgacs, E., Zochbauer-Muller, S., Shivakumar, L., Fong, K., Gao, B., Randle, D., Kondo, M., Virmani, A., Bader, S., Sekido, Y., Latif, F., Milchgrub, S., Toyooka, S., Gazdar, A. F., Lerman, M. I., Zabarovsky, E., White, M., and Minna, J. D. Epigenetic inactivation of RASSF1A in lung and breast cancers and malignant phenotype suppression. J. Natl. Cancer Inst. (Bethesda), 93: 691– 699, 2001. 20. Agathanggelou, A., Honorio, S., Macartney, D. P., Martinez, A., Dallol, A., Rader, J., Fullwood, P., Chauhan, A., Walker, R., Shaw, J. A., Hosoe, S., Lerman, M. I., Minna, J. D., Maher, E. R., and Latif, F. Methylation associated inactivation of RASSF1A from region 3p21.3 in lung, breast and ovarian tumours. Oncogene, 20: 1509 –1518, 2001. 21. Lo, K. W., Kwong, J., Hui, A. B., Chan, S. Y., To, K. F., Chan, A. S., Chow, L. S., Teo, P. M., Johnson, P. J., and Huang, D. P. High frequency of promoter hypermethylation of RASSF1A in nasopharyngeal carcinoma. Cancer Res., 61: 3877–3881, 2001. 22. Spafford, M. F., Koch, W. M., Reed, A. L., Califano, J. A., Xu, L. H., Eisenberger, C. F., Yip, L., Leong, P. L., Wu, L., Liu, S. X., Jeronimo, C., Westra, W. H., and Sidransky, D. Detection of head and neck squamous cell carcinoma among exfoliated oral mucosal cells by microsatellite analysis. Clin. Cancer Res., 7: 607– 612, 2001. 23. Herman, J. G., Graff, J. R., Myohanen, S., Nelkin, B. D., and Baylin, S. B. Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands. Proc. Natl. Acad. Sci. USA, 93: 9821– 9826, 1996. 24. Dong, S. M., Pai, S. I., Rha, S. H., Hildesheim, A., Kurman, R. J., Schwartz, P. E., Mortel, R., McGowan, L., Greenberg, M. D., Barnes, W. A., and Sidransky, D. Detection and quantitation of human papillomavirus DNA in the plasma of patients with cervical carcinoma. Cancer Epidemiol. Biomark. Prev., 11: 3– 6, 2002. 25. Jin, Y., Mertens, F., Mandahl, N., Heim, S., Olegard, C., Wennerberg, J., Biorklund, A., and Mitelman, F. Chromosome abnormalities in eighty-three head and neck squamous cell carcinomas: influence of Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2003 American Association for Cancer Research. 3640 RASSF1A Inactivation in Head and Neck Cancer culture conditions on karyotypic pattern. Cancer Res., 53: 2140 –2146, 1993. 26. Gollin, S. M. Chromosomal alterations in squamous cell carcinomas of the head and neck: window to the biology of disease. Head Neck, 23: 238 –253, 2001. 27. Van Dyke, D. L., Worsham, M. J., Benninger, M. S., Krause, C. J., Baker, S. R., Wolf, G. T., Drumheller, T., Tilley, B. C., and Carey, T. E. Recurrent cytogenetic abnormalities in squamous cell carcinomas of the head and neck region. Genes Chromosomes Cancer, 9: 192–206, 1994. 28. Rosas, S. L., Koch, W., da Costa Carvalho, M. G., Wu, L., Califano, J., Westra, W., Jen, J., and Sidransky, D. Promoter hypermethylation patterns of p16, O6-methylguanine-DNA-methyltransferase, and deathassociated protein kinase in tumors and saliva of head and neck cancer patients. Cancer Res., 61: 939 –942, 2001. 29. Sanchez-Cespedes, M., Esteller, M., Wu, L., Nawroz-Danish, H., Yoo, G. H., Koch, W. M., Jen, J., Herman, J. G., and Sidransky, D. Gene promoter hypermethylation in tumors and serum of head and neck cancer patients. Cancer Res., 60: 892– 895, 2000. 30. Hosoe, S., Shigedo, Y., Ueno, K., Tachibana, I., Osaki, T., Tanio, Y., Kawase, I., Yamakawa, K., Nakamura, Y., and Kishimoto, T. Detailed deletion mapping of the short arm of chromosome 3 in small cell and non-small cell carcinoma of the lung. Lung Cancer, 10: 297–305, 1994. 31. Wei, M. H., Latif, F., Bader, S., Kashuba, V., Chen, J. Y., Duh, F. M., Sekido, Y., Lee, C. C., Geil, L., Kuzmin, I., Zabarovsky, E., Klein, G., Zbar, B., Minna, J. D., and Lerman, M. I. Construction of a 600-kilobase cosmid clone contig and generation of a transcriptional map surrounding the lung cancer tumor suppressor gene (TSG) locus on human chromosome 3p21.3: progress toward the isolation of a lung cancer TSG. Cancer Res., 56: 1487–1492, 1996. 32. Waber, P. G., Lee, N. K., and Nisen, P. D. Frequent allelic loss at chromosome arm 3p is distinct from genetic alterations of the VonHippel Lindau tumor suppressor gene in head and neck cancer. Oncogene, 12: 365–369, 1996. 33. Shivakumar, L., Minna, J., Sakamaki, T., Pestell, R., and White, M. A. The RASSF1A tumor suppressor blocks cell cycle progression and inhibits cyclin D1 accumulation. Mol. Cell. Biol., 22: 4309 – 4318, 2002. 34. Lee, M. G., Kim, H. Y., Byun, D. S., Lee, S. J., Lee, C. H., Kim, J. I., Chang, S. G., and Chi, S. G. Frequent epigenetic inactivation of RASSF1A in human bladder carcinoma. Cancer Res., 61: 6688 – 6692, 2001. 35. Hogg, R. P., Honorio, S., Martinez, A., Agathanggelou, A., Dallol, A., Fullwood, P., Weichselbaum, R., Kuo, M. J., Maher, E. R., and Latif, F. Frequent 3p allele loss and epigenetic inactivation of the RASSF1A tumour suppressor gene from region 3p21.3 in head and neck squamous cell carcinoma. Eur. J. Cancer, 38: 1585–1592, 2002. 36. van den Brekel, M. W., and Balm, A. J. Editorial comment on “frequent 3p allele loss and epigenetic inactivation of the RASSF1A tumour suppressor gene from region 3p21.3 in head and neck squamous cell carcinoma” by Hogg and colleagues. Eur. J. Cancer, 38: 1561– 1563, 2002. 37. Hasegawa, M., Nelson, H. H., Peters, E., Ringstrom, E., Posner, M., and Kelsey, K. T. Patterns of gene promoter methylation in squamous cell cancer of the head and neck. Oncogene, 21: 4231– 4236, 2002. 38. Kwong, J., Lo, K. W., To, K. F., Teo, P. M., Johnson, P. J., and Huang, D. P. Promoter hypermethylation of multiple genes in nasopharyngeal carcinoma. Clin. Cancer Res., 8: 131–137, 2002. 39. Boyle, J. O., Hakim, J., Koch, W., van der Riet, P., Hruban, R. H., Roa, R. A., Correo, R., Eby, Y. J., Ruppert, J. M., and Sidransky, D. The incidence of p53 mutations increases with progression of head and neck cancer. Cancer Res., 53: 4477– 4480, 1993. 40. Sauter, E. R., Cleveland, D., Trock, B., Ridge, J. A., and KleinSzanto, A. J. p53 is overexpressed in fifty percent of pre-invasive lesions of head and neck epithelium. Carcinogenesis (Lond.), 15: 2269 – 2274, 1994. Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2003 American Association for Cancer Research. Epigenetic Inactivation of RASSF1A in Head and Neck Cancer Seung Myung Dong, Dong-Il Sun, Nicole E. Benoit, et al. Clin Cancer Res 2003;9:3635-3640. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://clincancerres.aacrjournals.org/content/9/10/3635 This article cites 40 articles, 24 of which you can access for free at: http://clincancerres.aacrjournals.org/content/9/10/3635.full.html#ref-list-1 This article has been cited by 8 HighWire-hosted articles. Access the articles at: /content/9/10/3635.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on June 12, 2017. © 2003 American Association for Cancer Research.