Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
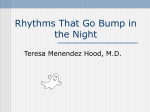
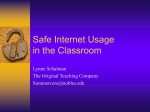
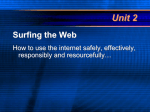
Arrhythmia/Electrophysiology Dual-Chamber Versus Single-Chamber Detection Enhancements for Implantable Defibrillator Rhythm Diagnosis The Detect Supraventricular Tachycardia Study Paul A. Friedman, MD; Robyn L. McClelland, PhD; William R. Bamlet, MS; Helbert Acosta, MD; David Kessler, MD; Thomas M. Munger, MD; Neal G. Kavesh, MD; Mark Wood, MD; Emile Daoud, MD; Ali Massumi, MD; Claudio Schuger, MD; Stephen Shorofsky, MD; Bruce Wilkoff, MD; Michael Glikson, MD Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Background—Delivery of inappropriate shocks caused by misdetection of supraventricular tachycardia (SVT) remains a substantial complication of implanted cardioverter/defibrillator (ICD) therapy. Whether use of optimally programmed dual-chamber ICDs lowers this risk compared with that in single-chamber ICDs is not clear. Methods and Results—Subjects with a clinical indication for ICD (n⫽400) at 27 participating centers received dual-chamber ICDs and were randomly assigned to strictly defined optimal single- or dual-chamber detection in a single-blind manner. Programming minimized ventricular pacing. The primary end point was the proportion of SVT episodes inappropriately detected from the time of programming until crossover or end of study. On a per-episode basis, 42% of the episodes in the single-chamber arm and 69% of the episodes in the dual-chamber arm were due to SVT. Mortality (3.5% in both groups) and early study withdrawal (14% single-chamber, 11% dual-chamber) were similar in both groups. The rate of inappropriate detection of SVT was 39.5% in the single-chamber detection arm compared with 30.9% in the dual-chamber arm. The odds of inappropriate detection were decreased by almost half with the use of the dual-chamber detection enhancements (odds ratio, 0.53; 95% confidence interval, 0.30 to 0.94; P⫽0.03). Conclusions—Dual-chamber ICDs, programmed to optimize detection enhancements and to minimize ventricular pacing, significantly decrease inappropriate detection. (Circulation. 2006;113:2871-2879.) Key Words: arrhythmia 䡲 defibrillation 䡲 heart arrest 䡲 tachyarrhythmias T he implanted cardioverter/defibrillator (ICD) is highly effective in decreasing mortality due to cardiac arrhythmias in high-risk patients.1,2 However, delivery of inappropriate shocks caused by misclassification of rapidly conducted supraventricular tachycardia (SVT) as ventricular tachycardia (VT) remains a substantial complication of ICD therapy, affecting 8% to 40% of patients.3– 8 Inappropriate shocks can lead to pain, anxiety, depression, impaired quality of life, proarrhythmia, and poor tolerance of life-saving ICD therapy.9 Intuitively, dual-chamber detection enhancements, which use atrial and ventricular intracardiac information to formulate a diagnosis, should be superior to single-chamber, ventricularonly detection enhancements. However, early nonrandomized studies and subsequent small randomized studies failed to show any superiority of dual-chamber over single-chamber diagnosis.3–5 Moreover, the finding that backup ventricular pacing is not inferior to dual-chamber pacing in ICD recipients who do not require pacing10 and recent studies showing the effectiveness of single-chamber ICDs in prophylactic sudden death prevention2 have led to a decrease in dual-chamber ICD use. In the United States, the Center for Medicare and Medicaid Services ruled that “providers must justify the medical necessity of devices other than those with a single lead.”11 Editorial p 2862 Clinical Perspective p 2879 The most desirable method of limiting inappropriate therapies is appropriate rhythm detection and discrimination by the ICD. Received October 19, 2005; revision received February 17, 2006; accepted April 7, 2006. From the Division of Cardiovascular Diseases (P.A.F., T.M.M.) and the Division of Biostatistics (R.L.M., W.R.B.), Mayo Clinic, Rochester, Minn; Electrophysiology, Trinity Medical Center, Rock Island, Ill (H.A.); Electrophysiology and Cardiac Pacing, Austin Heart, Austin, Tex (D.K.); Cardiology/Electrophysiology, Watson Clinic, Lakeland, Fla (N.G.K.); Internal Medicine/Cardiology, Virginia Commonwealth University, Richmond (M.W.); Cardiovascular Disease, MidWest Research Foundation, Riverside Methodist Hospital, Columbus, Ohio (E.D.); Center for Cardiac Arrhythmias and Electrophysiology, Texas Heart Institute, Houston (A.M.); Cardiology, Henry Ford Hospital, Detroit, Mich (C.S.); Maryland Heart Center, University of Maryland Medical Center, Baltimore (S.S.); Cardiovascular Disease, The Cleveland Clinic Foundation, Cleveland, Ohio (B.W.); and Electrophysiology and Pacing, Heart Institute, Sheba Medical Center, Tel Hashomer, Ramat Gan, Israel (M.G.). Correspondence to Paul A. Friedman, MD, Division of Cardiovascular Diseases, Mayo Clinic, 200 First St SW, Rochester, MN 55905. © 2006 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/CIRCULATIONAHA.105.594531 2871 2872 Circulation June 27, 2006 Figure 1. Default programming detection enhancement parameters. A indicates atrial rate; FIB, ventricular fibrillation; and V, ventricular rate. Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Detection enhancement programming is complex, and one reason for the lack of superiority of dual-chamber over single-chamber enhancements in previous studies may have been the use of nonoptimal enhancement settings. Perhaps more important, improvements in atrial sensing and morphology-based algorithms, which may substantially improve dual-chamber detection, have recently become available.12–15 We hypothesized that the optimal use of the latest generation dual-chamber detection enhancements would decrease inappropriate detection of SVT compared with optimal single-chamber detection enhancements in a broad population of ICD recipients. If true, this would indicate that dualchamber ICDs are preferable to single-chamber devices in most ICD recipients because of a decrease in the morbidity due to inappropriate therapy. younger than 18 years, Mobitz II or greater heart block, previous atrioventricular (AV) node ablation, permanent atrial fibrillation or flutter, preexisting separate pacemaker pulse generator that was not to be explanted, life expectancy of ⬍1 year or on a transplant waiting list, intra-aortic balloon pump, inotropic drug (not digitalis) necessary for hemodynamic support, chronic serious bacterial infection, inability to receive nonthoracotomy ICD, or inability to program device as per protocol. Subjects were randomly assigned to device programming for ventricular-only or dual-chamber detection within 3 days of ICD implantation in a single-blind manner (subject not aware). The randomization was balanced within a site in blocks, with the use of sequentially numbered, opaque sealed envelopes. Subjects were followed up for 6 months, with a patient visit, device function assessment, and data collection at baseline and at 3 follow-up visits scheduled at 2 to 4 weeks, 3 months, and 6 months after programming. Data from unscheduled visits were also retrieved for analysis. Devices and Programming Methods Study Conduct The study was investigator initiated and managed. Data were independently managed by Mayo Clinical Trial Services. A steering committee of 2 electrophysiologists (P.A.F., M.G.), 2 statisticians (R.L.M., W.R.B.), and a coordinating center representative met approximately every 3 months to review safety and accrual data. The members of the steering committee wrote the article and assume overall responsibility for the data and analysis. The study was supported by an unrestricted grant from St Jude Medical (St Paul, Minn), which had no role in study design, analysis, or interpretation. The institutional review boards of all participating institutions approved the study. Study Design Subjects were enrolled between December 2002 and October 2004 at 27 participating centers. Eligible patients had a clinical indication for ICD therapy and received a dual-chamber defibrillator. Patients were excluded if any of the following conditions were present: age All subjects received a dual-chamber ICD manufactured by St Jude Medical. Systematic efforts were made during implantation to eliminate far-field R wave oversensing, and the absence or presence of far-field R wave oversensing was recorded. The optimal detection enhancement programming used in this study was defined by a previous analysis of a large episode database14 and determined by the investigators, with manufacturer input. Detection enhancement programming is summarized in Figure 1. Programming was specified to minimize ventricular pacing. Defibrillator programmers were preloaded with study templates for dual-chamber and ventricular-only detection enhancement to facilitate uniform programming across all subjects. Dual-chamber detection used rate branch classification based on the relative rates in the atria (A) and ventricles (V; V⬎A, V⫽A, or V⬍A) before application of detection enhancements to maximize enhancement performance, as described in Figure 1. In all subjects, use of extended timers that delivered therapy after a tachyarrhythmia duration was met regardless of device diagnosis was disallowed to prevent degradation of detection specificity. At least 1 detection zone with rate enhancements was programmed. To ensure a large window Friedman et al Dual-Chamber vs Single-Chamber ICD Detection 2873 Figure 2. Patient enrollment, status, and episodes of arrhythmia. Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 for rhythm discrimination, a VT detection rate no faster than 150 beats per minute (bpm) and a ventricular fibrillation (VF) detection rate no slower than 200 bpm, with application of discriminators up to the VF cutoff, were required. It was strongly suggested that devices in all subjects be programmed to DDD or DDI with a lower rate of 50 to 60 bpm with an AV interval as long as possible to permit native conduction when present. Use of antitachycardia pacing (ATP) in the VT zone was strongly encouraged to minimize painful shocks. However, to maximize detection programming compliance, all therapy programming was at the discretion of the investigator. Optimization of subparameters without changing detection type (single- or dual-chamber) was permitted after a subject received an inappropriate therapy. Optimization events were recorded. End Points The primary end point was the proportion of SVT episodes inappropriately detected (number of inappropriately detected SVT episodes divided by total number of SVT episodes) from the time of programming until crossover or end of study. Inappropriately detected SVT was defined as any SVT episode that met ventricular rate detection criteria and was inappropriately classified as VT. Any episode lasting long enough to trigger detection resulting in a stored electrogram was reviewed and classified in an unblinded manner by the site investigator and in a blinded manner by a core group investigator; discrepancies in the overall type (SVT versus VT) were adjudicated by an additional blinded review. Disagreements concerning arrhythmia subtypes (type of SVT or VT) were not adjudicated, and results presented are based on the opinion of the blinded reviewer. Secondary end points included time to first inappropriately treated episode, VT/VF sensitivity, number of arrhythmia-related hospitalizations or clinic visits, and the early termination rate. A post hoc analysis was performed to determine how selection of a VT detection rate ⬎150 bpm would alter detection and discrimination. Sample Size and Power We estimated that 30% of patients would have at least 1 SVT episode during the 6-month follow-up period. We predicted that the singlechamber device would inappropriately detect 30% of the SVT episodes.3 In contrast, we believed that if only 10% of all SVT episodes for the dual-chamber group were inappropriately detected, this would constitute a minimal clinically important decrease of 20 percentage points. Because only 30% of the subjects were anticipated to have any SVT episodes, the total number of patients was increased to 400 (⬇200 subjects per arm) to maintain an 80% power. Many subjects had ⬎1 episode, which increased the study power. Statistical Analysis Patient characteristics were compared between study arms with the use of 2-sample t tests for continuous variables and 2 tests for categorical variables. If the number of occurrences of a categorical variable was very small, we verified the results using the Fisher exact test. The primary end point was the proportion of SVT episodes inappropriately detected by the device within the first 6 months after implantation. A logistic regression model was fit to investigate the association between treatment group (dual- versus single-chamber) and the odds of inappropriate detection. The correlation between multiple episodes within the same subject was accounted for by using a generalized estimating equations (GEE) approach, with a compound symmetrical correlation structure.16,17 Note that the GEE model estimates an odds ratio, not a relative risk. The odds ratio does not approximate the relative risk in this study because the end point is not rare. We report the raw per-episode rates of inappropriate detection and the GEE-adjusted rates, which move the per-episode rate estimates toward the average per-subject rate based on the within-subject correlation and the GEE model. Time to first inappropriate detection was examined graphically with Kaplan-Meier plots and with Cox proportional hazards regression models including a term for programming arm. Time was indexed in 2 ways: by calendar time and by the number of SVT episodes observed. 2 tests were used to compare rates of early study withdrawal and crossovers between study arms. The total number of hospitalizations and clinic visits related to arrhythmias or inappropriate therapies delivered by the ICD was compared by Wilcoxon rank sum tests. The authors had full access to the data and take responsibility for its integrity. All authors have read and agree to the manuscript as written. Results Patients and Events During the study period, 400 subjects were prospectively randomly assigned to ventricular-only (n⫽199) or dualchamber (n⫽201) detection. A total of 1253 arrhythmia episodes occurred in 103 of the 199 subjects in the ventricular-only detection arm, and 1090 episodes occurred in 104 of the 201 subjects in the dual-chamber detection arm (Figure 2). Sixty-two subjects (31%) in the ventricular-only arm and 75 subjects (37%) in the dual-chamber arm had SVTs; the risk of SVT occurrence was similar in patients with and without a history of SVT. On a per-episode basis, 42% of the episodes in the single-chamber arm and 69% of the episodes in the dual-chamber arm were due to SVT (P⫽0.06). Mortality (3.5% in both groups) and overall early study withdrawal (noncompletion of 6 months of follow-up due to any 2874 Circulation June 27, 2006 Patient Characteristics and Medications by Study Group Detection Patient Characteristic/Medication Age at implantation, y Ventricular Only (n⫽199) Dual Chamber (n⫽201) P 0.46 65.1⫾11.3 64.3⫾11.3 Men 156 (78) 163 (81) 0.50 ICD indication, primary prevention 132 (66) 136 (68) 0.78 Left ventricular ejection fraction, % 32⫾13 32⫾13 0.95 Arrhythmia history Atrial fibrillation Atrial flutter Other SVT 40 (20) 36 (18) 0.59 8 (4) 12 (6) 0.36 12 (6) 8 (4) 0.35 VT 128 (64) 119 (59) 0.32 VF 21 (11) 31 (15) 0.14 Catheter ablation (not AV node) 1 (0.5) 8 (4) 0.02 Surgical maze 2 (1) 1 (0.5) 0.56 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Cardiac history Hypertension 122 (61) 111 (55) 0.22 Coronary artery disease 161 (81) 163 (81) 0.96 Percutaneous coronary intervention 80 (40) 91 (45) 0.31 Coronary artery bypass graft 82 (41) 90 (45) 0.47 Congestive heart failure 98 (49) 109 (54) 0.32 Dilated cardiomyopathy 36 (18) 30 (15) 0.39 AV node agents 178 (89) 184 (92) 0.47 -Blocker 162 (81) 168 (84) 䡠䡠䡠 AV nodal slowing 12 (6) 15 (7) 䡠䡠䡠 Non–AV nodal slowing (dihydropyridines) 19 (10) 18 (9) 䡠䡠䡠 䡠䡠䡠 0.37 Calcium channel blocker Digoxin/digitalis 53 (27) 70 (35) Antiarrhythmic drugs 59 (30) 68 (34) Sotalol 14 (7) 11 (5) 䡠䡠䡠 Amiodarone 44 (22) 55 (27) 䡠䡠䡠 Dofetilide 0 (0) 1 (0.5) 䡠䡠䡠 Other 9 (5) 9 (4) 䡠䡠䡠 Values are mean⫾SD or number of patients (percentage). cause, including death; 14% ventricular-only, 11% dualchamber) were similar in both groups (P⫽0.46). More patients crossed over from ventricular-only to dual-chamber detection (n⫽17) than the reverse (n⫽2; P⬍0.001), but the overall crossover rate was small. Demographic and clinical data for the 2 treatment groups are shown in the Table. No clinically important differences were seen between the groups at baseline. At baseline, the mean left ventricular ejection fraction was 32⫾13%, the ICD was implanted in 67% of subjects for primary sudden death prevention, and 25% of subjects had a known history of SVT. Use of AV node conduction slowing medications and antiarrhythmic medications was the same in both groups at baseline (Table) and at each follow-up visit. Far-field R wave oversensing at device check occurred in 3% of patients in the dual-chamber arm and 9% of subjects in the ventricular-only arm. Primary End Point: Inappropriate Detection The rate of inappropriate detection of SVT was 39.5% (210 of 531 SVT episodes) (GEE rate estimate, 46.5%) in the ventricular-only detection arm compared with 30.9% (232 of 750 episodes) (GEE rate estimate, 32.3%) in the dualchamber arm (Figure 3). After we accounted for the positive correlation between multiple episodes occurring within the same subject, the odds of inappropriate detection were decreased by almost half with the use of the dual-chamber detection enhancements (odds ratio, 0.53 [95% confidence interval, 0.30 to 0.94]; P⫽0.03). With the exception of sinus tachycardia, for which single- and dual-chamber detection were similar, dual-chamber detection consistently had a lower rate of inappropriate detection than ventricular-only detection across all arrhythmia subtypes (Figure 3). However, differences in classification of arrhythmia subtype between the site investigator and blinded reviewers were not adjudicated, and Friedman et al Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Figure 3. Rate of inappropriate detection of SVT, with breakdown by arrhythmia subtype (atrial fibrillation, atrial flutter/atrial tachycardia [tach], sinus tachycardia, or other), for subjects with single- or dual-chamber detection. “Other” arrhythmias include atrial tachycardia, junctional tachycardia, AV nodal reentrant tachycardia, and AV reentrant tachycardia. Subtype classification was based on blinded episode reviewer. The odds ratio (OR) and probability value refer only to the overall comparison of inappropriate detection of SVT. these rates are presented only to examine consistency across the subtypes. In general, rate branch sorting permitted differential application of the detection enhancements, resulting in superior performance of dual-chamber algorithms, as shown Dual-Chamber vs Single-Chamber ICD Detection 2875 in Figure 4. SVT occurred in the VF zone (in which detection enhancements were not applied) in 17% of all inappropriately detected episodes in the dual-chamber arm and 2% in the single-chamber arm (P⬍0.001). Of all SVT episodes detected as VF, the investigator classified 45% as atrial fibrillation, 10% as atrial flutter, and 45% as 1:1 SVT or “other.” In terms of the statistical analysis, the within-subject correlation was quite high (⬇0.50). This is likely because subjects tend to experience the same types of arrhythmias repeatedly. Thus, it is important to use a statistical model that can handle correlated data. On a per-subject basis, among those with some SVT episodes the median number of episodes was 4 (range, 1 to 58). The average per-subject rate of inappropriate detection was 51% for the single-chamber group and 34% for the dual-chamber group. Figure 5 depicts the percentage of subjects with at least 1 inappropriate detection based on the number of episodes experienced. The cumulative number of recorded SVT episodes is used because detection enhancement effectiveness is best assessed by the response to actual episodes, as opposed to time to an episode. Subjects in the dual-chamber arm were less likely to have an inappropriate detection for any given number of recorded SVT episodes, although this difference did not reach statistical significance (P⫽0.13). The median number of episodes until the first inappropriate detection was Figure 4. Examples of single-chamber and dual-chamber detection. A, Stored electrogram of an atrial tachycardia episode (T) inappropriately detected as VT in the single-chamber arm, resulting in ATP therapy delivery. Episode of atrial tachycardia begins with a premature atrial complex (asterisk), which is followed by a regular tachycardia. The arrhythmia has an abrupt onset (indicating VT), is regular (favoring VT), but has a morphology consistent with SVT (check marks at arrow). Because this patient had single-chamber detection, atrial information is not used, and because 2 of 3 detection enhancements indicate VT, therapy is delivered inappropriately. Note that the arrhythmia was not terminated by the ATP. This led to additional therapies (not shown). B, Stored electrogram of an appropriately diagnosed atrial tachycardia episode resulting in withholding of therapy in a patient in the dual-chamber arm. Asterisk indicates initiating atrial premature complex. The episode is detected in the V⫽A rate branch indicated by the “I⫽” symbol (circled). In this rate branch, only morphology is programmed on, as per protocol. Morphology indicates SVT (check marks at arrows), so therapy is appropriately withheld. Correct classification of SVTs with a 1:1 A to V relationship is often problematic for ICDs given their abrupt onset (mimicking VT) and regular intervals (also mimicking VT). This makes morphological discrimination potentially more useful in this group of arrhythmias. A indicates atrial electrogram; P, sensed P wave; R, sensed R wave; S, sinus beat; TB, tachycardia B; and V, ventricular electrogram. Numbers indicate intervals between P or R waves. 2876 Circulation June 27, 2006 Figure 5. Number of SVT episodes until the first inappropriate detection. Graph shows percentage of subjects with at least 1 inappropriate detection by total number of SVT episodes recorded (P⫽0.13 for difference between the 2 curves). Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 1.5 for the single-chamber group and 4 for the dual-chamber group. The calendar time to first inappropriate detection of SVT episodes was not significantly different between groups (median, 103 days for ventricular-only versus 108 days for dual-chamber; P⫽0.45). Inappropriate Therapy Delivery Inappropriate detection led to inappropriate therapy delivery for the 2 groups, as depicted in Figure 6. The overall rate of inappropriate therapy delivery (ATP or shock) of 33.0% (GEE rate estimate, 38.3%) in the ventricular-only group was significantly greater than that in the dual-chamber group (24.8%; GEE rate estimate, 26.1%; P⫽0.02), for a 46% decrease in the odds of inappropriate therapy. The odds of an inappropriate shock were not significantly different (P⫽0.18) because of the greater use of ATP in the ventricular-only arm. VT Detection Overall, of 937 VT episodes that occurred (615 in the ventricular-only arm, 322 in the dual-chamber arm), 871 (93%) were detected. Of the 66 episodes that were not detected, 16 were sustained (⬎30 seconds in duration): 9 in the ventricular-only arm and 7 in the dual-chamber arm. Thus, 98.2% of episodes were either detected or terminated spontaneously in ⬍30 seconds. No VF episodes were missed (of 12 in the ventricular-only arm and 10 in the dual-chamber arm). No difference was seen between the groups in the total number of arrhythmia-related hospitalizations (6% of patients in each group had at least 1 hospitalization) or additional clinic visits (5% of ventricular-only subjects, 7% of dualchamber subjects). Optimization of detection enhancements within each study group was also the same, occurring in 34 subjects (17%) in the ventricular-only group (19 due to inappropriate detection of SVT, 6 due to underdetection of VT/VF, and 9 not specified) and in 34 subjects (17%) in the dual-chamber group (23 for inappropriate detection of SVT, 2 for underdetection of VT/VF, and 9 not specified). Complications In the entire study population, atrial lead fracture or failure was reported in 1 patient (0.25%), atrial lead dislodgment in 4 patients (1%), and atrial sensing errors in 4 patients (1%). There was no difference between groups in the rate of any complication. Atrial sensing errors were uncommon, occurring in ⬍5% of patients in the dual-chamber group. Discussion Main Findings Our study had 2 principal findings. First, the odds of inappropriate detection of SVT as VT were decreased by half with use of dual-chamber detection compared with ventricular-only detection with optimal programming of both. This observation held true in a broad population of ICD recipients and resulted from improved detection across all arrhythmia subtypes, with the exception of sinus tachycardia, for which detection was equivalent in both arms. Second, as expected, the decrease in inappropriate detections led to a decrease in inappropriate therapy, from 33% to 25% (including all therapy types) at 6 months. Although the overall number of therapies was decreased in the dual-chamber arm, the number Figure 6. Therapy delivery for all SVT episodes by study group. In the singlechamber group, 321 of the 531 SVT episodes (60.4%) were appropriately diagnosed as SVT, and therapy was withheld (Rejected, no Rx). Thirty-five episodes (6.6%) were misdiagnosed but received no therapy (Detected, no Rx), predominantly because of termination after detection but before therapy delivery; 154 (29.0%) received inappropriate ATP only, and 21 (4.0%) received inappropriate shocks. In contrast, of the 750 SVT episodes in the dual-chamber group, 518 (69.1%) were appropriately diagnosed as SVT and therapy withheld, 46 (6.1%) were misdiagnosed but received no therapy, 118 (15.7%) received inappropriate ATP only, and 68 (9.1%) received inappropriate shocks. The rate of inappropriate therapy delivery was significantly higher in the single-chamber group (33.0%) than the dual-chamber group (24.8%; P⫽0.03). Friedman et al of shocks delivered was slightly higher in the dual-chamber arm, although this difference was not significant. This discrepancy between therapies and shocks reflects the greater use of ATP in the ventricular-only arm. In our study, the type of therapy programmed was left up to the investigator to ensure compliance with the strict detection programming requirements. Treating physicians programmed more ATP for patients in the single-chamber arm to minimize the risk of inappropriate shock. Had identical therapies been programmed, we predict that dual-chamber detection would have resulted in fewer shocks. This result highlights the importance of detection and therapy programming in minimizing ICD morbidity. The role of ATP in reducing shocks has been described previously.18 Comparison With Other Studies Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Most previous studies comparing dual-chamber with singlechamber ICDs have not found a superiority of dual-chamber detection.3–5 The lack of superiority in most previous studies relates to difficulties with atrial sensing, the predominant cause of detection errors in dual-chamber ICDs.19 Accurately determining that the ventricular rate is greater than the atrial rate eliminates approximately half of all tachycardia episodes from further analysis, which prevents subsequent detection error14; conversely, underdetecting the atrial rate leads to misclassification as “V⬎A” and to misdiagnosis of SVT as VT with consequent inappropriate therapy. Rate branch sorting also permits differential application of the detection enhancements on the basis of relative atrial and ventricular rates, improving the performance of the enhancements and the ICDs (Figure 4).14 In the present study, careful attention to atrial sensing resulted in ⬍3% far-field R wave oversensing in the dualchamber arm; atrial sensing errors accounted for only 5% of the misclassifications in the dual-chamber arm. In contrast, atrial sensing errors accounted for 41% to 75% of treated misclassifications in previous comparative studies.3,4,8 In the report by Kuhlkamp et al,3 an early-generation dual-chamber defibrillator was used with a relatively long, fixed, atrial blanking period (86 ms) after each sensed or paced ventricular event. This configuration resulted in the atrial undersensing that led to most misclassifications. In the trials by Theuns et al20 and Deisenhofer et al,4 various defibrillators with differing atrial sensing characteristics were used, but atrial sensing errors were common. The 1⫹1 trial21 randomly assigned patients to a crossover comparison of single-chamber and dual-chamber detection. Only patients with known slow VT were enrolled. A “more than moderate superiority” of dual-chamber detection was found for the study end point, which was a combination of the number of inappropriate therapies and VTs slower than the VT detection interval. Our study confirms the results of the 1⫹1 trial and extends them beyond patients with known slow VTs to the general ICD population. Indeed, two thirds of the patients in the present study received their device for primary sudden death prevention. Like the 1⫹1 trial and in contrast to other previous studies, all patients in our study received dual-chamber ICDs that recorded atrial and ventricular intracardiac electrograms. This Dual-Chamber vs Single-Chamber ICD Detection 2877 ensured the accuracy of human-reviewer rhythm diagnosis in both study arms. In single-chamber devices, the absence of stored atrial electrograms limits interpretation of some arrhythmia episodes. Additionally, because the presence of atrial and ventricular electrograms in both groups gives their episode printouts an identical appearance, blinding for core group review was permitted, thus eliminating bias. It must be emphasized that the high frequency of end point occurrence in the present study (40% in the ventricular-only arm, 31% in the dual-chamber arm) was because we used inappropriate detection rather than inappropriate therapy as our study end point. This end point was chosen because the selection of dual- or single-chamber detection directly affects detection, not ventricular therapy. The rate of inappropriate detection in our single-chamber arm was similar to that reported as a secondary end point by Theuns et al5 (42%). Moreover, the rate of inappropriate shock in our population (4% to 9%) compares favorably with the 10% to 41% described in the other comparative studies.3–5 Because detection enhancements are not applied during redetection in current ICDs and because many SVTs are not terminated by ventricular therapies, a single misclassified episode may result in many therapies. Clinical Implications Although the implantable defibrillator is the most effective therapy available for sudden death prevention, substantial morbidity results from inappropriate therapy. We found that with optimally programmed current-generation defibrillators, use of dual-chamber devices decreases the odds of inappropriate detection by approximately half compared with optimal single-chamber detection. Although this decrease in detection resulted in fewer inappropriate therapies, number of shocks was not decreased because of greater use of ATP in the single-chamber arm. The benefit of the atrial lead may be modest in that aggressive use of ATP may prove as effective as dual-chamber detection for preventing shocks; however, we believe appropriate diagnosis is superior to inappropriate ATP for shock prevention. Inappropriate ATP carries a small risk of proarrhythmia. Other studies have found that a history of SVT predicts subsequent SVT.8 In our study, we found no such association. The proportion of subjects having at least 1 episode of SVT during the 6 months after implantation was high (32%), similar to that reported in other studies3–5 and almost identical for those with and without a history of SVT. This result suggests that dual-chamber devices should be considered in all ICD patients. Our findings also support the previous observation that therapy programming with use of ATP further minimizes patient shocks.18,22 Shock delivery is the final step in a cascade of events beginning with detection. Attention to each step of the cascade will minimize ICD morbidity. It is important to note that detection enhancements are nominally off in most currently available ICDs. In clinical use, the great majority of ICD parameters are left at nominal settings; therefore, if manufacturers were to set the detection enhancements nominally on, use of the enhancements might increase. 2878 Circulation June 27, 2006 Finally, devices were programmed to minimize ventricular pacing. Frequent ventricular pacing might have prevented template updates, affecting morphology function. Additionally, ventricular pacing introduces blanking and refractory periods that may have affected arrhythmia detection and classification, and it promotes heart failure and atrial fibrillation,23 which may also have affected the results. Limitations Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 ICD detection involves numerous complex functions, and unique approaches have been developed by each manufacturer. The results with dual-chamber detection found in the present study may not extend to other manufacturers’ devices. A blinded core group prevented physician bias, and GEE analysis mitigated biased variability estimates due to excessive episodes from a single subject. The study was designed to be powered for the primary end point. The Kaplan-Meier approach does not use as much information as the GEE approach (only the first inappropriately detected episode per subject is used) and hence has somewhat less power. However, the point estimates using this approach were in the same direction, and the magnitude of the effect appeared (qualitatively) similar. We chose to explore and present this analysis because it has a useful graphical component. Conclusion SVTs were common, occurring in 34% of ICD recipients within 6 months of implantation. SVT was inappropriately detected in ⬇66% of subjects in whom it occurred. More than three fourths of inappropriately detected episodes resulted in inappropriate therapy. Current-generation dual-chamber detection enhancements significantly lowered the rate of inappropriate detection from 40% to 31% (P⬍0.05). Dual-chamber ICDs, programmed to optimize detection enhancements and to minimize ventricular pacing, significantly decrease inappropriate detection. Acknowledgments John McGuire and Tamara Shipman of St Jude Medical reviewed the manuscript for technical accuracy. Editing, proofreading, and reference verification were provided by the Section of Scientific Publications, Mayo Clinic. Source of Funding This study was sponsored by an unrestricted grant from St Jude Medical (St Paul, Minn). Disclosures Dr Daoud reports having served as a consultant for St Jude and having served on the Speakers Bureau for St Jude. Dr Wilkoff reports having served as a consultant for St Jude Medical. The remaining authors report no conflicts. References 1. Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML, for the Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877– 883. 2. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, ClappChanning N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH, for the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure [published correction appears in N Engl J Med. 2005;352:2146]. N Engl J Med. 2005;352:225–237. 3. Kuhlkamp V, Dornberger V, Mewis C, Suchalla R, Bosch RJ, Seipel L. Clinical experience with the new detection algorithms for atrial fibrillation of a defibrillator with dual chamber sensing and pacing. J Cardiovasc Electrophysiol. 1999;10:905–915. 4. Deisenhofer I, Kolb C, Ndrepepa G, Schreieck J, Karch M, Schmeider S, Zrenner B, Schmitt C. Do current dual chamber cardioverter defibrillators have advantages over conventional single chamber cardioverter defibrillators in reducing inappropriate therapies? A randomized, prospective study. J Cardiovasc Electrophysiol. 2001;12:134 –142. 5. Theuns DA, Klootwijk AP, Goedhart DM, Jordaens LJ. Prevention of inappropriate therapy in implantable cardioverter-defibrillators: results of a prospective, randomized study of tachyarrhythmia detection algorithms. J Am Coll Cardiol. 2004;44:2362–2367. 6. Grimm W, Flores BF, Marchlinski FE. Electrocardiographically documented unnecessary, spontaneous shocks in 241 patients with implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 1992;15: 1667–1673. 7. Schmitt C, Montero M, Melichercik J. Significance of supraventricular tachyarrhythmias in patients with implanted pacing cardioverter defibrillators. Pacing Clin Electrophysiol. 1994;17:295–302. 8. Theuns DA, Klootwijk AP, Simoons ML, Jordaens LJ. Clinical variables predicting inappropriate use of implantable cardioverter-defibrillator in patients with coronary heart disease or nonischemic dilated cardiomyopathy. Am J Cardiol. 2005;95:271–274. 9. Schron EB, Exner DV, Yao Q, Jenkins LS, Steinberg JS, Cook JR, Kutalek SP, Friedman PL, Bubien RS, Page RL, Powell J. Quality of life in the antiarrhythmics versus implantable defibrillators trial: impact of therapy and influence of adverse symptoms and defibrillator shocks. Circulation. 2002;105:589 –594. 10. Wilkoff BL, Cook JR, Epstein AE, Greene HL, Hallstrom AP, Hsia H, Kutalek SP, Sharma A, for the Dual Chamber and VVI Implantable Defibrillator Trial Investigators. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: the Dual Chamber and VVI Implantable Defibrillator (DAVID) Trial. JAMA. 2002;288:3115–3123. 11. Centers for Medicare & Medicaid Services. Coverage determinations: implantable automatic defibrillators. In: Medicare National Coverage Determinations Manual. Baltimore, Md. CMS-Pub 100-3; Pt 1, section 20.4 [cited 2005 Jul 20]. Available at: http://www.cms.hhs.gov/mcd/ viewncd.asp?ncd_id⫽20.4&ncd_version⫽3&basket⫽ncd%3A20%2E4% 3A3%3AImplantable⫹Automatic⫹Defibrillators. Accessed May 24, 2006. 12. Swerdlow CD, Brown ML, Lurie K, Zhang J, Wood NM, Olson WH, Gillberg JM. Discrimination of ventricular tachycardia from supraventricular tachycardia by a downloaded wavelet-transform morphology algorithm: a paradigm for development of implantable cardioverter defibrillator detection algorithms. J Cardiovasc Electrophysiol. 2002;13: 432– 441. 13. Gold MR, Hsu W, Marcovecchio AF, Olsovsky MR, Lang DJ, Shorofsky SR. A new defibrillator discrimination algorithm utilizing electrogram morphology analysis. Pacing Clin Electrophysiol. 1999;22:179 –182. 14. Glikson M, Swerdlow CD, Gurevitz OT, Daoud E, Shivkumar K, Wilkoff B, Shipman T, Friedman PA. Optimal combination of discriminators for differentiating ventricular from supraventricular tachycardia by dual-chamber defibrillators. J Cardiovasc Electrophysiol. 2005;16:732–739. 15. Swerdlow CD, Friedman PA. Advanced ICD troubleshooting: part II. Pacing Clin Electrophysiol. 2006;29:70 –96. 16. Wilkoff BL, Kuhlkamp V, Volosin K, Ellenbogen K, Waldecker B, Kacet S, Gillberg JM, DeSouza CM. Critical analysis of dual-chamber implantable cardioverter-defibrillator arrhythmia detection: results and technical considerations. Circulation. 2001;103:381–386. 17. Liang K-L, Zewger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73:13–22. 18. Wathen MS, DeGroot PJ, Sweeney MO, Stark AJ, Otterness MF, Adkisson WO, Canby RC, Khalighi K, Machado C, Rubenstein DS, Volosin KJ, for the PainFREE Rx II Investigators. Pacing Fast Ventric- Friedman et al ular Tachycardia Reduces Shock Therapies (PainFREE Rx II) trial results. Circulation. 2004;110:2591–2596. 19. Israel CW, Gronefeld G, Iscolo N, Stoppler C, Hohnloser SH. Discrimination between ventricular and supraventricular tachycardia by dual chamber cardioverter defibrillators: importance of the atrial sensing function. Pacing Clin Electrophysiol. 2001;24:183–190. 20. Theuns D, Klootwijk AP, Kimman GP, Szili-Torok T, Roelandt JR, Jordaens L. Initial clinical experience with a new arrhythmia detection algorithm in dual chamber implantable cardioverter defibrillators. Europace. 2001;3:181–186. 21. Bansch D, Steffgen F, Gronefeld G, Wolpert C, Bocker D, Mletzko RU, Schols W, Seidl K, Piel M, Ouyang F, Hohnloser SH, Kuck KH. The 1⫹1 Dual-Chamber vs Single-Chamber ICD Detection 2879 trial: a prospective trial of a dual- versus a single-chamber implantable defibrillator in patients with slow ventricular tachycardias. Circulation. 2004;110:1022–1029. 22. Wilkoff B, Al E. EMPIRIC study. Paper presented at: Heart Rhythm 2005 Scientific Sessions; May 4 –7, 2005; New Orleans, La. 23. Sweeney MO, Hellkamp AS, Ellenbogen KA, Greenspon AJ, Freedman RA, Lee KL, Lamas GA, for the MOde Selection Trial Investigators. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. 2003;107: 2932–2937. CLINICAL PERSPECTIVE Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 The implanted cardioverter/defibrillator (ICD) has become the gold standard for sudden cardiac death prevention in high-risk patients. Delivery of inappropriate shocks caused by misclassification of rapid supraventricular tachycardia (SVT) is a substantial limitation of ICDs, affecting up to 40% of patients. Dual-chamber ICDs, which use atrial and ventricular electrograms for arrhythmia diagnosis, were anticipated to improve discrimination between SVT and ventricular arrhythmias. Early studies did not support this hope, suggesting that single-ventricular-lead ICDs should be favored if atrial pacing is not required. The present multicenter prospective study sought to determine whether dual-chamber arrhythmiasensing algorithms reduce ICD misclassification of SVT. Four hundred patients receiving dual-chamber ICDs were randomly assigned to dual- or single-chamber detection enhancements and followed up for 6 months. All ICDs were programmed to minimize ventricular pacing. SVTs occurred frequently, regardless of whether a history of atrial tachyarrhythmias was present. The odds of misclassification of SVT were decreased by almost half with the use of dual-chamber detection enhancements (odds ratio, 0.53; P⫽0.03). This improved detection translated to a reduction in inappropriate ICD therapies. It did not, however, reduce inappropriate shocks, because antitachycardia pacing, rather than shocks, was used more frequently in the single-lead group. These data show that use of a dual-chamber ICD that provides atrial sensing is a reasonable consideration for most patients. They also demonstrate the importance of both appropriate detection and programming of antitachycardia pacing for minimizing shocks. Dual-Chamber Versus Single-Chamber Detection Enhancements for Implantable Defibrillator Rhythm Diagnosis: The Detect Supraventricular Tachycardia Study Paul A. Friedman, Robyn L. McClelland, William R. Bamlet, Helbert Acosta, David Kessler, Thomas M. Munger, Neal G. Kavesh, Mark Wood, Emile Daoud, Ali Massumi, Claudio Schuger, Stephen Shorofsky, Bruce Wilkoff and Michael Glikson Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Circulation. 2006;113:2871-2879; originally published online June 12, 2006; doi: 10.1161/CIRCULATIONAHA.105.594531 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2006 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/113/25/2871 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/