Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Marburg virus disease wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Oesophagostomum wikipedia , lookup
Schistosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
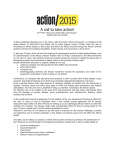
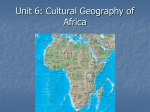
Case Report East African Sleeping Sickness in Chennai R Gopalakrishnan, JM Easow Abstract A traveler to East Africa developed fever, an eschar on his forearm and thrombocytopenia shortly after returning home to Chennai, India. Trypanosoma brucei rhodesiense infection was diagnosed on examination of his peripheral smear. He made a full recovery after receiving a course of suramin. INTRODUCTION E ast African trypanosomiasis is an endemic disease in animals in parts of Kenya, Tanzania and Uganda. It is transmitted to humans by the bite of infected tsetse flies,1 and has been reported in American and European travelers to game parks in these countries.2-5 A literature search of the Medline/Pubmed database revealed no human cases of East African trypanosomiasis documented in India. We believe this case may be the first. leptospira IgM, anti HAV IgM, anti HCV, HIV 1 and 2 ELISA and HBsAg were all negative. ECG and echocardiogram were normal. Blood and urine cultures showed no growth. CSF analysis revealed five cells/hpf (lymphocytes), protein = 50, glucose = 103. Examination of his peripheral smear revealed the trypomastigotes of Trypanosoma brucei (Fig. 2). A diagnosis of haemo-lymphatic stage East African CASE REPORT A 40 years male presented with fever, chills, nausea and jaundice for one week. He had noticed a painless black skin lesion on his right forearm, gradually increasing in size. He denied headache, other CNS symptoms or arthraglia. His past medical history was notable only for impaired glucose tolerance. There was no history of tobacco/alcohol abuse. He had returned three days earlier from a two week trip to the Serengeti and Ngorongoro game parks in Kenya and Tanzania with his family. He did not recall any insect bites, but did not use full sleeved clothing or insect repellent on exposed skin areas. Examination revealed stable vital signs except for fever to 102°F. Jaundice was present and he had a black, necrotic, non-tender eschar over his right forearm, about 6 cm in size (Fig. 1). The remainder of his examination was unremarkable. Laboratory tests revealed that ALT = 420, AST = 440, alkaline phosphatase = 425, albumin = 3.3, globulin = 3.2, LDH = 434, bilirubin = 6.6 (direct = 5.1), CPK = 39. Hb = 12.4, Hct = 37, platelets = 17,000 and WBC = 4400/mm3 (N 73, L 19, E 1, M 7). Urinalysis revealed 6-8 RBCs and 3-5 WBCs/hpf. The CXR was clear and an ultrasound abdomen showed hepatosplenomegaly. Peripheral smear for MP/MF, Apollo Speciality Hospital, Chennai. Received : 5.2.2002; Revised : 25.6.2002; Accepted : 2.8.2002 302 Fig. 1 : Eschar over right forearm Fig. 2 : Peripheral smear JAPI • VOL. 51 • MARCH 2003 trypanosomiasis was made and he was treated with suramin (five doses of 1g IV on days 1, 3, 7, 14 and 21). All symptoms, laboratory abnormalities and the eschar resolved completely and the patient was doing well on follow up six months later. - The presence of a chancre narrows the differential diagnosis even further to trypanosomiasis and rickettisal disease caused by either Rickettsia africae6 or R. conori. - Diagnosis can be made in most cases by a simple peripheral smear examination. DISCUSSION - Suramin is not available in India and has to be imported. In our case we obtained a supply from the Liverpool School of Tropical Medicine in the UK. In summary, in this era of increasing globalization and foreign travel, this case highlights the importance of documenting a travel history well and suspecting diseases endemic to the area of travel. Trypanosomiasis or sleeping sickness is caused by the bite of an infected tsetse fly (Glossina species). It comprises two stages of clinical disease, an initial hemo-lymphatic stage and a subsequent CNS stage. The East African form, caused by T. brucei rhodiesiense, is a zoonosis of cattle and other wild ungulates and occurs in Kenya, Tanzania and Zambia. It is more rapidly progressive than the West African variety and is uniformly fatal if untreated. The hemolymphatic phase is characterized by a chancre at the site of inoculation, fever, pancytopenia and widespread lymphadenopathy. Diagnosis is usually by peripheral smear examination which reveals the characteristic trypomastigotes. Serology is available but is not usually needed in East African disease diagnosis as the levels of parasitemia are high. The CNS stage is characterized by the development of meningo-encephalitis, and is diagnosed by the appearance of CSF pleocytosis or the demonstration of trypomastigotes in the CSF. It is important to distinguish the two stages as prognosis is worse and treatment different. Suramin, the drug of choice for the hemo-lymphatic phase, is ineffective once the CNS is involved, for which the drug of choice is a toxic agent, melarsoprol. REFERENCES There has been a recent upsurge in cases of trypanosomiasis reported among travellers to East African game parks.5 Our case has several important illustrative points: - It is important to suspect the diagnosis in any febrile traveler to East African game parks. 1. Guerrant RL, Walker DH, Weller PF (editors). Tropical infectious diseases - Principles, pathogens and practice (Churchill Livingstone). 2. Sinha A, Grace C, Alston WK, Westenfeld F, Maguire JH. African trypanosomiasis in two travelers in the United States. Clin Infect Dis 1999;29:840-4. 3. Hepburn BC, Wolfe RD, Vestal MA. East African trypanosomiasis in the United Sates. Am Fam Physician 1995;52:381. 4. Braendli B, Dankwa E, Junghanns T. East African sleeping sickness (Trypanosoma rhodesiense infection)P in two Swiss travelers to the trophics. Schweiz Med Wochenschr 1990;120:1348-52. 5. Moore DAJ, Edwards M, Escombe R, et al. African trypanosomiasis in travelers returning to the United Kingdom. Emerg Inf Dis 2002;8:74-6. 6. Raoult D, Fournier PE, Fenollar F, et al. Rickettsia africae, a tick borne pathogen in travelers to sub-Saharan Africa. N Eng J Med 2001;344:1504-10. Announcement The office bearers of the Association of Physicians of India, Orissa State Branch, for the year 2003. Chairman : SP Das Vice Chairman : RK Dalai Hon. Secretary : KN Padhiary Jt. Hon. Secretary : S Mohanty Treasurer J K Panda : Sd/KN Padhiary JAPI • VOL. 51 • MARCH 2003 303