Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
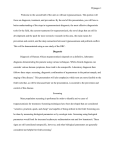
East African Trypanosomiasis Steven L. Oscherwitz pleting three separate courses of the drug by April 19. On that drug, the patient developed transient restless leg sensations and tingling paresthesias of the distal extremities. Approximately 4 to 5 days following the first and second sets of melarsoprol doses, the patient developed a headache with delirium and periods of somnolence, and these symptoms improved rapidly on high dose dexamethasone (4 mg intravenously every 6 hours) and subsequent prednisone taper. Magnetic resonance imaging of the brain with gadolinium was unremarkable. During the patient’s hospitalization, thrombocytopenia, hepatocellular dysfunction, and renal insufficiency improved in a steady fashion. No fevers or opportunistic infections became apparent. At discharge on April 20, 2001 the patient was much improved clinically. Over the months following hospital discharge, peripheral neuropathy pain and muscle weakness slowly subsided. The patient tolerated a second course of melarsoprol in November 2001 for persisting CSF lymphocytosis. The CSF white blood cell count has decreased in a steady fashion subsequently. Lumbar punctures continue every several months and are scheduled through 2005 for surveillance. The patient has vowed never again to travel to Africa, as have most of his acquaintances. A 56-year-old white male sustained fly bites in southern Kenya, beginning on approximately March 14, 2001, in the Masai Mara game reserve area. He awoke on Friday, March 16 with fever, chills, and swollen, red, bite areas on the right facial and cervical areas. Stomach cramps became apparent on March 18, and the patient was subsequently advised to return to the United States for further care. He left South Africa on March 19. The patient came to a local emergency room here in Mesa, Arizona, on March 21, reporting fevers and headaches over the preceding days, occasional scotomata, severe right submandibular swelling with ulceration, and a chancre of the left upper back. He was anemic and thrombocytopenic, with renal insufficiency. Buffy coat preparations showed active trypanosomes, and trypanosomes were also seen in large numbers on peripheral blood smears (Fig.). The patient’s white blood cell count was 5800/mm3, with 45% segs, 43% bands, 7% lymphocytes, 4% monocytes, and 1% metamyelocytes on differential. Hematocrit was 37% and platelets 9000/uL. The patient underwent initiation of hemodialysis in the intensive care unit and was quickly able to begin suramin therapy, following a call to the Centers for Disease Control and Prevention (CDC) in Atlanta and air delivery of the drug. Magnetic resonance imagery of the patient’s face and neck showed minimal soft tissue thickening in the area of the trypanids (chancres), with deep cervical adenopathy evident on those films. The patient’s cerebrospinal fluid (CSF) white blood cell count was 12 per mL with a differential of 76% lymphocytes, 13% segs, and 11% monocytes. His CSF glucose was 82 mg/dL and protein 45 mg/dL, with no trypanosomes evident on CSF examination. Stage II (meningoencephalitic) infection with Trypanosoma brucei rhodesiense disease was suspected, per World Health Organization (WHO) guidelines (African trypanosomiasis or sleeping sickness).1 The patient began melarsoprol on March 26, 2001, com- Discussion Trypanosoma brucei gambiense (western and central African) and Trypanosoma brucei rhodesiense (east African) parasites are transmitted by tsetse flies of genus Glossina. Infection with T. b. rhodesiense disease runs a more rapid course than the gambiense form, with meningoencephalitis sometimes seen less than 4 weeks after receiving an infective bite. T. b. gambiense has a chronic and protracted course and may last several years, whereas T. b. rhodesiense is acute and can cause death in a matter of weeks or months. Both types of sleeping sickness are fatal if left untreated. Sleeping sickness is found uniquely in subSaharan Africa. Sleeping sickness of both varieties is a daily threat to more than 60 million men, women, and children in 36 countries of subSaharan Africa, 22 of which are among the least developed countries in the world. This is the fifth patient since 1967 with T. b. rhodesiense second-stage disease reported in the United States (Anne Moore, CDC, verbal communication). Of the 30 cases of trypanosomiasis (both T. b. rhodesiense and T. b. gambiense) reported in the United States in the past 34 years, 7 were reported in 2000. Since 1990, 14 of 15 US cases have been found in travelers to game parks near Steven L. Oscherwitz, MD: 2501 E. Southern Avenue, #22, Tempe, Arizona. The author had no financial or other conflicts of interest to disclose. Correspondence: Steven L. Oscherwitz, MD, 2501 E. Southern Avenue, #22, Tempe, AZ 85282. J Travel Med 2003; 10:141–143. 141 142 Figure Trypanosome at high power 330 original magnification. or in Tanzania.2 Notable recent cases of trypanosomiasis in travelers include five European tourists and one South African tourist who became ill with trypanosomiasis in East Africa toward the end of March, 2001.3 Another American traveler presented in March after diagnosis and partial therapy in Nairobi.4 All physicians should consider T. b. rhodesiense infection in travelers returning from East Africa, especially if cutaneous chancres and fever are noted (although chancres may be absent). The symptoms and examination findings of East African trypanosomiasis may mimic those caused by malaria, borreliosis, brucellosis, tularemia, plague, anthrax, enteric fever, and rickettsial infection. Fever, rash, lethargy, headache, gastrointestinal symptoms, delirium, and myalgias have been common in the few patients evaluated in the United States.4,5 Trypanosomal chancres or trypanids have also been described in some detail, accompanying the other clinical manifestations.6–8 Trypanosomes seen in blood, CSF, lymph node aspirate, or chancre aspirate smears make the diagnosis; serologic methods for T. b. rhodesiense infections are unreliable due to late seroconversion and unknown sensitivity and specificity of these tests at the present time (Anne Moore, CDC, verbal communication). T. b. rhodesiense and gambiense trypomastigotes are indistinguishable on microscopic examination. Treatment must be started earlier in T. b. rhodesiense infections than in T. b. gambiense infections to prevent long-term sequelae, due to the more rapid progression of the former disease. All treatment schedules currently in use are empiric; the schedules are based predominantly on patients with T. b. gambiense infections and relatively less severe clinical status.9 Considerable discussion continues regarding which regimen might be best, with some authors advising more aggressive treatment and others believing that therapy is already too aggressive.9 Although organisms were read- J o u r n a l o f Tr a v e l M e d i c i n e , Vo l u m e 1 0 , N u m b e r 2 ily apparent on this patient’s peripheral blood smears and buffy coat wet preparation, parasites are often difficult to demonstrate on CSF examinations, even in the setting of high level parasitemia. Melarsoprol is not recommended in early (hemo-lymphatic) trypanosomiasis because of its toxicity.10 Suramin and pentamidine are recommended by the WHO Expert Committee on Trypanosomiasis for such cases, with CSF white blood cell count ≤ 5 cells/mm3 and protein ≤ 25 mg/dL. Neurologic (second stage) involvement is indicated by trypanosomes in the CSF or CSF white blood cell count > 5 cells/mm3 or CSF protein > 25 mg/dL. Lumbar puncture is indicated in all cases of suspected African trypanosomiasis. Sleeping sickness has continued to prevent development of large tracts of African land by decreasing the human labor force and preventing use of domestic animals. The disease is 100% fatal if left untreated, with resurgence of disease occurring in the African countries with ongoing civil violence (Angola, Republic of Congo, Sudan, and Uganda). Disrupted or absent public health infrastructure, short supplies of medication, as well as the biology of the trypanosomes make control efforts problematic. Even if antigenic variation, immune response of the human host, and the mechanisms of natural resistance of wild mammals against trypanosomes are elucidated, substantial obstacles to control of the disease will remain. The general public, the public health community, and much of the scientific community are not generally aware of this infection, its public health importance, and its devastating impact.11,12 Changing treatment recommendations based on data from ongoing trials, and WHO literature, which does not distinguish between T. b. rhodesiense and gambiense disease, will serve to keep our job challenging in the future. Acknowledgment Thanks to Louis Rosati, MD and Karen Woo, BS, Medical Laboratory Technologist, Pathology Department Desert Samaritan Hospital, Mesa, AZ. Their digital video of this patient’s actively motile T. b. rhodesiense parasites may soon appear on the DPDx portion of the CDC Parasitology Diagnostic Web site. References 1 World Health Organization. Fact sheet number 258. March 2001. Available at: http://www.who.int/inffs/on/fact258.html. 2. Centers for Disease Control and Prevention. Interactive Session #2: Clinical Investigations from the CDC. Presented to the 50th annual meeting of the American Society of Tropical Medicine and Hygiene at the American Committee on Tropical Medicine and Travelers’ Health Session, November 14, 2001, Atlanta, Georgia. O s c h e r w i t z , E a s t A f r i c a n Tr y p a n o s o m i a s i s 3. TropNetEurop. Outbreak of African trypanosomiasis among travelers to the Serengeti. 28.03.01 May 2001. 4. Promed V2001 Monday March 26, 2001. 5. Sinhua A, Grace C, Alston WK, et al. African trypanosomiasis in two travelers from the United States. Clin Infect Dis 1999; 29:840–844. 6. Iborra C, Danis M, Bricaire F, Caumes E. A Traveler returning from Central Africa with fever and a skin lesion. Clin Infect Dis 1999; 28:679–680. 7 McGovern TW, Williams W, Fitzpatrick JE, et al. Cutaneous manifestations of African trypanosomiasis. Arch Dermatol 1995; 131:1178–1182. 143 8. Panosian CB, Cohen L, Bruckner D, et al. Fever, leukopenia, and a cutaneous lesion in a man who had recently traveled in Africa. Rev Infect Dis 1991; 13:1130–1138. 9. Burri C, Nkunku S, Merolle A, Smith T. Efficacy of new, concise schedule for melarsoprol in treatment of sleeping sickness caused by Trypanosoma brucei gambiense: a randomized trial. Lancet 2000; 355:1419–1425. 10. Dumas M, Bouteille B. Treatment of human African trypanosomiasis. Bull World Health Organ 2000; 78:1474. 11. Seed JR. Current status of African trypanosomiasis. ASM News 2000; 66:395–402. 12. WHO. Communicable disease surveillance and response. CSR 2001. Waiting to depart from the Milano Central Railway Station. Submitted by Marc Shaw.