Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
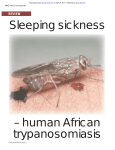
Wijangco 1 Welcome to the second half of the unit on African trypanosomiasis. This portion will focus on diagnosis, treatment, and prevention. By the end of this presentation, you will have a better understanding of the steps in trypanosomiasis diagnosis, the most effective diagnosistic tools for the field, the current treatments for trypanosomiasis, the novel drugs that are still in development and the push for more extensive research in this area, the main means for prevention and control, and the deep connection between trypanosomiasis and political conflict. This will be demonstrated using a case study of the DRC. Diagnosis Diagnosis of Human African trypanosomiasis depends on a definitive, laboratory diagnosis demonstrating the parasite using various techniques. While clinical diagnosis can consider various human symptoms, these tend to be nonspecific. Laboratory diagnosis then follows three steps: screening, diagnostic confirmation of trypansomes in the patient sample, and staging of the disease.1 This presentation will also emphasize which tests are more feasible to the field work that, as will be discussed later on the presentation, is essential to the prevention and control of this disease. Screening Mass population screening is performed in order to identify active cases of trypanosomiasis for treatment. Screening techniques have been developed that are considered “sensitive, practical, quick, and cheap” and capable of being utilized in the field. Screening can be done by measuring biological parameters or by serologic tests. Screening using biological parameters would look for increased erythrocyte sedimentation rate and low hematocrit. These signs are still considered nonspecific, however, and other biological parameters are generally considered not helpful for field screening.1 Wijangco 2 Screening is primarily done using serological techniques, including CATT, LATEX, immunofluorescence assays, and ELISA. CATT and LATEX are the most useful for screening in the field. CATT stands for the Card Agglutination Test for Trypanosomiasis. With samples of blood, plasma, or serum, CATT serves as a rapid and simple agglutination assay that detects antibodies for T.b. gambiense. When using CATT, a single drop of reagent is mixed with a single drop of blood. The reagent has been laboratory-produced to contain antigens specific to T.b. gambiense. The two droplets are then shaken for five minutes on a rotator and results can be looked for with the naked eye. As can be seen in this video, CATT screening is extremely straightforward and not labor intensive.1 (Show Wellcome Trust video.) CATT screening can also be done en masse, with technicians able to test ten patients at a time and see hundreds per day. Sensitivity is of the test is estimated between 87-98%. It should be noted, though, that falsenegatives can occur with strains of trypanosome infection lack the gene used for creating the reagent antigen. Specificity is calculated to be about 95%. Infection with malaria or a non-human trypanosome can result in false-positives.1 Serologically-based screening in the field also utilizes a test called the LATEX. The procedure for LATEX is analogous to that of CATT. Key differences are that it utilizes three different surface antigens and that these antigens are coupled with latex particles in suspension. Sensitivity of LATEX is estimated to be 71% to 100%, and specificity is estimated to be 96% to 99%.1 Additional screening tests include immunofluorescence assays and enzyme-linked immunosorbent assays (ELISA). These can generally only be done in the lab, however, and are not useful in the field. Immunofluorescence assays are performed with serum or filter paper eluates. ELISA is performed with serum, FP eluates, or cerebrospinal fluid (CSF).1 Wijangco 3 Here you can see trypanosomes stained with different antibodies. Diagnostic Confirmation Following screening, there must be diagnostic confirmation of the presence of the parasite. This is done by finding trypanosomes in the blood, lymph node aspirate, or CSF. This can be quite challenging, as parasite numbers of T.b. gambiense for an infected individual can vary from 10,000 trypanosomes/ml to only 100 trypanosomes/ml. Moreover, the process of parasite detection is labor-intensive. In order to improve sensitivity, serial examination of blood over a period of consecutive days can be performed. Larger quantities of blood can also be examined. Great care should be taken with the samples once they are taken, as trypanosomes can lyse quickly.1 Tests for diagnostic confirmation include examination of chancre aspirate, lymph node aspirate, wet and thick blood films, microhematocrit centrifugation technique, quantitative buffy coat, and mini-anion exchange centrifugation technique (mAECT). The chancre aspirate can be examined directly under a microscope but this is typically not useful in the field because most infections are detected long after the chancre first appears. Lymph node aspirate refers to the palpation and puncture of the cervical lymph node (CLN). Following a positive CATT test, lymph node aspirate is examined under a microscope for motile trypansomes. This is simple and cheap, but not cost-effective for CATT-negative individuals. Here you can see a chancre and enlarged lymph node. Wet and thick blood films can be put together following a finger prick and can be examined under the microscope for motile trypansomes. Wet blood films have a low sensitivity, but are cheap and simple. Thick blood films have a higher sensitivity, but are more time-consuming and require technical expertise for proper diagnosis. Here you can see trypanosomes in wet and thick blood films. Microhematocrit centrifugation technique involves Wijangco 4 the centrifugation of blood samples to separate a layer of trypanosomes between the plasma and the erythrocytes. This is a very time-consuming process, but this can be used by mobile mass screening teams. The quantitative buffy coat test also involves centrifugation. Blood is centrifuged in order to concentrate the parasites. The sample is then stained with acridine orange, causing the kinetoplasts and nuclei of the parasite to fluorescence. This has a high sensitivity, but is relatively sophisticated, requiring a darkroom, microscope, technicians, and more. Finally, the mini-anion-exchange centrifugation technique (mAECT) separates trypanosomes from blood cells in a sample due to the lower negative charge of the parasite. The newly separated sample is then centrifuged to concentrate the parasites and can be examined under the microscope. This procedure is equally time-consuming and labor-intensive.1 These images demonstrate the layers resulting from centrifugation in the quantitative buffy coat and the fluorescence of kinetoplasts and nuclei following acridine orange staining. Staging As the final step in the diagnostic process, should a patient test positive in screening and have confirmed parasitemia in the blood (or demonstrated parasites in the lymph node aspirates or CSF), the stage of the patient’s infection must finally be determined. First-stage HAT features parasites only in the hemolymphatic system, whereas second-stage HAT features considerable numbers of the parasite in the meningoencephalitic system. There are several clinical signs and blood tests that can indicate the infection stage, but CSF examination following lumbar puncture is considered essential. The lumbar puncture and examination will indicate the disease stage depending on three factors: white blood cell count, presence or absence of trypanosomes, and protein content. A high white blood cell count exceeding more than 5 cells/ul is the most common technique. The threshold of 5 cells/ul is debatd, but it is agreed that should a patient Wijangco 5 present with confirmed trypanosomes in the lymph node or bed and with more than 20 cells/ul in CSF, he or she should be treated for meningoencephalitic HAT. The visualization of trypanosomes in CSF confirms second-stage HAT. Sensitivity for this test can be improved via single or double centrifugation, but this is time-consuming and requires more equipment that could be less feasible in field work. Finally, a high protein content of greater than 370 mg/liter in a dye-binding protein assay can also be indicative of second stage HAT. This procedure is not recommended for use in general, due to its method sophistication, the lack of standardization, the instability of the relevant reagents, and its low added value to the information garnered from the cell count. For future tests, second-stage HAT infections tend to have extremely high levels of immunoglobulins but a simple and robust serological test for stage has not yet been developed for the field.1 Here you can see a patient whose brain has been invaded by HAT. To the right you can see trypanosomes in the brain. Treatment Treatment mainly utilizes the following four drugs: melarsoprol, suramin, pentamidine, and eflornithine. Please take a moment to consider the following chart and the administration of different drugs or drug combinations depending on 1) whether the patient is infected with T.b. gambiense or T.b. rhodesiense and 2) whether the infection has progressed into second-stage, meningoencephalitic HAT or is still in first-stage, hemolymphatic HAT.2 Melarsoprol is melarsen oxide complexed with dimercaprol. It may also be referred to as Arsobal or mel B. As melarsoprol is capable of crossing the blood-brain barrier, it is the primary drug used for treating A. trypanosomiasis when the infection has reached the neurological stage. This is crucial. However, as it has an arsenic component, it is therefore extremely toxic. As much as 10% of patients treated with melarsoprol die or experience post-treatment reactive Wijangco 6 encephalopathy (PTRE). To prevent the patient from getting a Herxheimer reaction, pretreatment with corticosteroids may be necessary.3 Melarsoprol can be absorbed orally but usually is administered via intravenous infusion. Notably, there are now resistance issues with melarsoprol. As much as 30% of patients in the Congo and Uganda have now been found to be resistant and unresponsive to melarsoprol treatment.2 The image to the right demonstrates the apoptosis occurring as a result of melarsoprol treatment. Suramin is less toxic than melarsoprol because it is absorbed by trypanosomes, but it is not absorbed by mammalian cells. However, it is still toxic and can induce nausea, vomiting, seizures and unconsciousness. Suramin is effective for the hemolymphatic stage but ineffective for second-stage neurological involvement. For serious cases of neurological involvement, suramin might be needed as a pretreatment before melarsoprol.3 Typially, suramin is given via an intravenous injection. Before the first treatment dosage in the suramin series, a test dosage of 200mg should be administered to test the patient reaction. Historically some patients have responded to suramin with anaphylactic shock.2 Pentamidine, like suramin, is effective for the hemolymphatic stage, but ineffective for neurological involvement. Side effects include hypotension, tachycardia, nausea, and vomiting. Like melarsoprol, pentamidine treatment may need pretreatment with corticosteroids to prevent a Herxheimer reaction in the patient.3 Along with suramin, pentamidine is mainly used for T.b. gambiense since T.b. rhodesiense tends to have the more acute progression of the infection and consequently rapid CNS involvement. Suramin is typically administered via intramuscular or intravenous injection, which has technical challenges in the rural, endemic field.2 Eflornithine is DL-alpha-difluoromethylornithine, or DFMO. Eflornithine is only effective against T. b. gambiense, as several T. b. rhodesiense samples were found to be resistant Wijangco 7 to the drug naturally. Despite this limitation, eflornithine has distinctive advantages. It is effective for both early and late stage disease.3 It is the first drug that is effective against late stage infection that does not have an arsenic component.4 Moreover, it is effective for patients whose strain of infection have been found to be resistant to melarsoprol and other arsenic-based treatment.3 As with the other medicines just discussed, eflornithine is administered intravenously.2 Combination therapy is also being investigated and has shown promising results.2,5 A combination of nifurtimox has been used with melarsoprol2,5 and separately with eflornithine. Nifurtimox Eflornithine Combination Therapy (NECT) is currently being studied by Epicenter and MSF-Holland.6 Fexinidazole is also currently being studied by Drugs for Neglected Diseases Initiative.6 The hope is that combination therapy will be more effective than the use of a single therapy on its own and that new drugs can be designed with lower toxicity than the current prevailing treatments.2,5 This speaks to a serious issue in terms of treatment of African trypanosomiasis. Until around 2001, there was a lack of research and innovation in developing novel, safer, and more effective treatments. North America, Europe, and Japan have no market for kinetoplastid infection treatments. Therefore, pharmaceutical companies and other institutions have had little incentive invest time and energy into drug development for illnesses like A. trypanosomiasis. Most of the drugs still in use were developed in the early or mid-20th century. As was evident among the side effects of the four major drug treatments, he current drugs are extremely toxic and sometimes deadly to patients.4 Therefore, groups like DNDi are working to develop new drugs and decrease current drug toxicity. Prevention Wijangco 8 Prevention methods are closely linked to the diagnosis methods discussed earlier in this presentation, as there is a heavy use of mass screening and treatment to control HAT. It should be noted that transmission via the tsetse fly tends to be complicated and slow, and thus only about 0.1% of flies tend to carry mature parasites. When human prevalence is low, which is the case outside of epidemic foci, a low density of flies can break the entire cycle of transmission.7 This presentation will now consider different prevention methods the key difference between T.b. gambiense and T.b. rhodesiense in prevention and control in that only the latter has animal reservoirs, and then provide examples of various prevention programs. Prevention methods use several different approaches. First, it should be noted that no vaccine exists and that chemoprophylaxis is avoided because of high drug toxicity and low risk of infection. As discussed in the section on diagnosis, there are means for case-finding and treating those who test positive. This tends to use a strictly targeted, vertical approach, whereby mobile teams visit remote areas. Those who test positive in the screening are treated immediately by the team or recommended to specialized services.8 In regards to control and surveillance, for areas that have already reached a prevalence low enough to no longer be considered a public health problem, as is seen particularly with T.b. gambiense in some places, a strong control and surveillance program must be implemented by the national health care infrastructure to maintain this.9 Much work concentrates on the vector control of the tsetse flies. Insecticides are applied in a variety of ways. Tsetse fly traps or screens are often doused in insecticide, while also covered with odors that are attractive to flies. Some areas use the sequential aerosol spraying technique, with repeated aerial spraying of low concentration insecticide. Control methods also include spraying of animals with insecticide.8 As can be expected, the control methods have their limitations. The fly traps’ effectiveness is limited when they are applied on a small scale, which Wijangco 9 tends to allow reinfection or reemergence.10 Fly traps also tend to only be effective bait for savannah tsetse flies, and not river-based tsetse flies. The aerosol spraying is limited by high expense and the necessary infrastructure. A final method of control is the sterile insect technique (SIT), in which sterile males are engineered and released into the wild to compete with wild, possibly infectious males.7 One of the control methods mentioned was insecticide spraying of animals, which is particularly relevant to T.b. rhodesiense. T.b. rhodesiense has animal reservoirs ranging from domestic animals like cattle and dogs, to wild animals like antelope. In order to manage these reservoirs, public health officials should therefore coordinate with veterinary and natural resource management services. For both T.b. rhodesiense and T.b. gambiense, however, asymptomatic humans who have not yet developed symptoms of sleeping sickness can act as harmful reservoirs.9 Several groups and collaborations have worked toward prevention and control. The WHO in particular designed the Programme to Eliminate Sleeping Sickness and various other WHO initiatives. The WHO, the Food and Agriculture Organization (FAO), the International Atomic Energy Agency (IAEA), and the Organization of African Unity organized the “Initiative for Central Africa” in the 1990s to coordinate HAT programs across the region, including national governmental powers and institutions like MSF.6 The WHO, in partnership with FAO, IAEA, and the African Union InterAfrican Bureau for Animal Resources (AU-IBAR), formed what became the Programme Against African Trypanosomiasis (PAAT) in 1997.9 Public-private partnerships began around 1999 to develop new drugs and drug combinations, bringing in the voices of such pharmaceutical companies as Aventis, Bayer, and Bristol-Myers Squibb (BMS).6 The Pan-African Tsetse and Trypanosomiasis Eradication Campaign (PATTEC) formed in 2000 Wijangco 10 with the goal to eliminate the tsetse fly in isolated foci using insecticide spraying, traps, and sterile insect technique. The founders considered the tsetse fly and trypanosomiasis problems as influential to Africa’s development.10 The Drugs for Neglected Diseases Initiative (DNDi) was founded in 2003 by MSF, the UNDP/World Bank/WHO’s Special Programme for Research and Training in Tropical Diseases (TDR), and five other public sector entities (the Oswaldo Cruz Foundation, the Indian Council for Medical Research, the Kenya Medical Research Institute, the Malaysian Ministry of Health, and the Pasteur Institute of France). The work of DNDi focuses on developing new drugs and HAT is one of its primary diseases.11,12 Thus much work is being done to prevent and control HAT. Conflict and Contagion: A case study of the Democratic Republic of the Congo (DRC) Now we will consider HAT in the light of humanitarian crises. Conflict has influenced both the resurgence and continuation of HAT incidence in several African countries, with the Democratic Republic of the Congo serving as the perfect example. HAT incidence and conflict have been associated with one another both qualitatively and quantitatively. For example, Berrang-Ford et al. looked at 35 African countries affected by HAT over a thirty year period from 1976 to 2004 and found that periods of high HAT incidence correspond closely to conflict and socio-political instability. Up through the early. 20th century, the African content experienced severe outbreaks of HAT. However, due to a heavy investment of resources during the colonial time period, HAT was nearly eliminated in the 1960s. Alongside conflict and political instability, coupled with fewer resources for prevention and control, HAT reemerged in the 1970s. Up until the decrease that started a few years ago, HAT had been increasing steadily.13 Wijangco 11 Reasons for the close association between conflict and contagion are multifold. First, conflicts tend to demonstrate a high level of population movement, either exposing previously unexposed groups to the infection or immunologically compromised by the strain of unrest and migration. Second, vector control and eradication interventions are impeded. Finally, surveillance and treatment programs are also hindered. With HAT in particular, conflict dramatically reduced, reallocated, or eliminated resources for interventions. As consequence, the surveillance, reporting, testing, and treatment of HAT were all obstructed. Examples of this include Uganda, Sudan, Equatorial-Guinea, and Congo-Brazzaville. With the case of the DRC, the ruin of the public health infrastructure and increase in HAT incidence are correlated with civil conflict.13 As is demonstrated by these figures, the incidence of HAT fluctuated from 1960 to 2004 in Africa, with the DRC representing 58% of all cases. From 1994 to 2000, the DRC showed far higher numbers of new cases than expected. This relates closely to a political regime change and ensuing conflict, leading to an approximately three-year lag period of decreased control programs. Notably, the DRC had maintained high incidence leading up to the 1994-2000 time period due to constant socio-political problems, including corruption and violent regimes.13 Medecins Sans Frontieres began working on HAT in the 1980s and for the past few years had been treating as much as 20- to 30% of all diagnosed cases. Taking a recent example of the tension between conflict and contagion, MSF worked in Haut-Uélé in Province Orientale in the DRC. From 2007 to 2009, they found extremely high infection rates, particularly for a fatal disease. Some areas had 3.4% infection rates and some even had 10% infection rates. Haut-Uélé is impoverished and has been an area of repeated conflict and political instability for years. Added to conflicts between the Lord’s Resistance Army (LRA) and the Uganda and DRC Wijangco 12 militaries, the general instability of the area has forced MSF to withdraw nearly all of its programs in Haut-Uélé. Given the approximately 3.4% infection rate, the two year long progression from stage one to stage two, and the fact that stage two is fatal by six to twelve months, it is conservatively estimated that 1,000 more people will die of HAT per every six months on top of those dying due to conflict.8 Thus, African trypanosomiasis is closely link to socio-political context. Only by considering these forces can progress be made. As Dr. Peter Hotez was kind enough to recommend upon inquiry, the key next step in the battle against HAT and in raising HAT attention is aggressive screening and treatment for T.b. gambiense, interrupting the cycle of transmission with cattle for T.b. rhodesiense, continuing to work in even remote and difficult areas of post-conflict zones, and further research into the promise of combination drugs. References: 1. Chappuis F, Loutan L, Simarro P, Lejon V, Büscher P. Options for Field Diagnosis of Human African Trypanosomiasis. Clin. Microbiol. Rev. 2005; 18: 133-146. 2. Leder K, Weller PF. Diagnosis, treatment, and prevention of African trypanosomiasis. UpToDate website. 2011 Available at: http://www.uptodate.com/contents/diagnosis-treatmentand-prevention-of-african-trypanosomiasis. Accessed March 3, 2012. 3. John DT, Petri WA. Markell and Voge’s Medical Parasitology. St. Louis: Elsevier; 2006. 4. Hotez P. Forgotten People, Forgotten Diseases: The Neglected Tropical Diseases and Their Impact on Global Health and Development. Washington, DC: ASM Press; 2008. 5. Odero RO, Cleveland KO, Kiminyo, KP, Lucey, DR. African Trypanosomiasis (Sleeping Sickness). eMedicine website. 2012. Available at: http://emedicine.medscape.com/article/228613. Accessed March 3, 2012. 6. Corty J-F. Human African Trypanosomiasis. In: Medical Innovations in Humanitarian Situations. Available at: http://www.doctorswithoutborders.org/publications/book/medicalinnovations/book.cfm?id=5243 &cat=medical-innovations. Accessed March 3, 2012. Wijangco 13 7. Brun R, Blum J, Chappuis F, Burri C. Human African trypanosomiasis. Lancet. 2010; 375: 148-59. 8. Chappuis F, Jochum B. Tackling Sleeping Sickness in conflict. Humanitarian Exchange Magazine. 2009. 9. Simarro PP, Diarra A, Ruiz Postigo JA, Franco JR, Jannin JG. The Human African Trypanosomiasis Control and Surveillance Programme of the World Health Organization 20002009: The Way Forward. PLoS Neglected Tropical Diseases. 2011; 5: e1007. 10. Simarro PP, Jannin J, Cattand P. Eliminating Human African Trypanosomiasis: Where Do We Stand and What Comes Next? PLoS Medicine. 2008; 5: 174-180. 11. Drugs for Neglected Diseases initiative. History. Drugs for Neglected Diseases initiative website. Available at: http://www.dndi.org/overview-dndi/history.html. Accessed March 3, 2012. 12. Medecins Sans Frontieres: Doctors Without Borders. Sleeping Sickness. Medecins Sans Frontieres: Doctors Without Borders website. Available at: http://www.doctorswithoutborders.org/news/issue.cfm?id=2401. Accessed March 3, 2012. 13. Berrang-Ford L, Lundine J, Breau S. Conflict and human African trypanosomiasis. Social Science and Medicine. 2011; 72: 398-407.