Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
[CANCER RESEARCH 50. 5904-5910. September 15. 1990]
Serum Tumor Marker Half-Life during Chemotherapy Allows Early Prediction of
Complete Response and Survival in Nonseminomatous Germ Cell Tumors'
Guy C. Toner, Nancy L. Geller, Claire Tan, Jerome Nisselbaum, and George J. Bosl2
Genitourinary Oncology Sen'ice [C. C. T., G. J. B.], Division of Soliti Tumor Oncology, Department of Medicine, Division of Biostalistics [N. L. G., C. T.], Department
oj Epidemiology and Biostatistics, and Department of Clinical Chemistry ¡J.N.], Memorial Sloan-Keltering Cancer Center, New York, New York 10021 and Department
of Medicine ¡G.C. T., G. J. B.¡,Cornell University Medical College, Ithaca, New York 14850
ABSTRACr
The prognostic value and therapeutic utility of monitoring the decay
of a-fetoprotein (AFP) and human chorionic gonadotropin (HCG) after
chemotherapy for nonseminomatous germ cell tumors was assessed.
Patients treated on successive front line chemotherapy protocols at
Memorial Hospital between 1979 and 1988 were studied. Marker values
taken within the first 90 days of treatment were reviewed for the 198
patients who had initially abnormal values and serial measurements at
Memorial Hospital. Since markers frequently increased in an unpredict
able fashion in the first week after chemotherapy, prechemotherapy
values would be inaccurate for assessment of subsequent half-life. There
fore, the first two values measured >7 days after the start of treatment
were used for all calculations of half-life. Among 38 patients who had
the two successive AFP measurements elevated, those who later achieved
a complete response (CR) had a median AFP half-life of 6.1 days (n =
20), whereas those not achieving CR had a median AFP half-life of 13.3
days (P = 0.02). Among 37 patients with the two successive HCG values
elevated, those who later achieved CR had a median HCG half-life of 4.2
days (n = 10), whereas those not achieving CR had a median HCG halflife of 18.4 days (P = 0.04). Forty-two patients who had an AFP halflife >7 days or an HCG half-life >3 days had significantly shorter overall
survival (median, 8 months) than the other 156 patients (median not
reached) (P < 0.0001). These 42 patients also achieved CR in lower
proportion (29%) than the other 156 patients (89%) (P < 0.0001). Cox
regression identified prolonged marker half-life as the most significant
independent predictor of survival. Lack of appropriate decay of serum
tumor markers can identify patients unlikely to achieve CR or prolonged
survival and thus can be used to select patients during treatment who
may benefit from an early change to more aggressive therapy.
INTRODUCTION
Identification of the 20-30% of patients with advanced
NSGCT' who are destined to fail conventional therapy (and
ultimately die from malignancy) remains an important objective
of clinical research. Most studies have concentrated on pretreat
ment clinical characteristics as prognostic variables. Pretreat
ment features have been used to predict the probability of
attaining CR (1) and relapsing after CR (2), demonstrate po
tential prognostic features within risk strata (3), and provide
evidence of stage migration (4). Despite their use, as many as
10% of "good risk" patients fail to achieve CR in current trials
The introduction of novel treatment strategies may allow an
improvement in survival for patients with a poor prognosis,
particularly if introduced early during management.
The management of NSGCT has been distinguished not only
by the frequency with which patients can be cured but also by
the availability of accurate serum tumor markers. AFP and
HCG are glycoproteins that are present at elevated levels in the
serum of most patients with metastatic NSGCT (10, 11). These
markers aid in management by reducing errors in diagnosis and
staging, providing prognostic information at the time of pres
entation of patients with metastatic disease and furnishing an
accurate and objective means of monitoring response to therapy
and detecting recurrent disease (10, 12-14).
Each marker is elevated in approximately 50-70% of patients
and 70-85% of patients with disseminated disease will have
one or both markers elevated at presentation (10, 11). The
kinetics of both markers have been studied after complete
surgical resection of disease and the biological half-life was 57 days for AFP and 18-48 h for HCG (15). This is the same as
the half-life in normal subjects (16, 17). While clearance from
the serum after chemotherapy has been less well studied, one
group reported mean half-lives of 5.7 days for AFP and 3.1
days for HCG (18).
In the setting of advanced disease, elevated pretreatment
marker values have been associated with a worse prognosis (1,
19). Therefore, a higher proportion of patients likely to fail
conventional therapy will have elevated marker levels prior to
the commencement of chemotherapy. Studies of markers after
chemotherapy have identified an increase immediately after
initiation of treatment in some patients (18, 20). This has been
postulated to be due to release of these substances after tumor
cell death.
The aim of this study was to analyze the prognostic value of
monitoring the decay of AFP and HCG after the commence
ment of chemotherapy. Prior studies of prognostic features
have emphasized pretreatment clinical characteristics. Marker
regression is a posttreatment characteristic which may be able
to identify early treatment failure (21) regardless of pretreat
ment risk stratification.
(5, 6). Almost all patients with refractory disease subsequently
die (7). A proportion of "poor risk" patients will achieve long-
PATIENTS AND METHODS
term survival with conventional therapy (3, 8, 9), making the
use of very intensive initial therapy inappropriate. Clarification
of new clinical characteristics permitting more accurate recog
nition of patients likely to fail therapy is therefore valuable.
All patients with NSGCT treated on Memorial Hospital front-line
chemotherapy protocols designed for good risk and poor risk patients
between 1979 and 1988 who had elevated AFP or HCG levels were
considered. To assure comparability of laboratory measurements, pa
tients who did not have an adequate number of serial measurements at
Memorial Hospital were excluded. The numbers of patients studied
and inclusion criteria are detailed in Table 1. All patients received
chemotherapy regimens containing high doses of cisplatin (>100 mg/
nr/cycle) or carboplatin. The details of treatment and response have
been described previously (5. 8, 22. 23).
Complete resolution of all biochemical and radiographie abnormal
ities or the resection of only teratoma or necrotic debris after chemo
therapy was classified as CR to chemotherapy. Complete resection of
residual malignancy after chemotherapy was classified as CR to chemo-
Received 3/19/90: accepted 6/14/90.
The costs of publication of this article were defrayed in pan by the payment
of page charges. This article must therefore be hereby marked advertisement in
accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Supported in part by N1H Grants CA 05826 and CM 57732 and the Brian
Piccolo Cancer Research Fund.
! To whom requests for reprints should be addressed, at Memorial SloanKettering Cancer Center. 1275 York Avenue, New York, NY 10021.
3The abbreviations used are: NSGCT. nonseminomatous germ cell tumor;
AFP. u-fetoprotcin: CR, complete response; d.f., degrees of freedom; HCG.
human chorionic gonadotropin; LDH. láclatedchydrogenase.
5904
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.
HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
Table 1 Criteria for inclusion in the analysis
Patients
Criteria
Evaluable patients with NSGCT entered in
prospective clinical trials 1979-1988
AFP > 15 ng/ml or HCG > 2 ng/ml (i.e.,
266
75 patients had normal pretreatment
AFP and HCG)
Marker levels monitored at Memorial
231
Hospital
198°
>2 marker values assayed between days 7
and 90 of treatment
or
Initial marker value after day 7 was nor
mal
176'
>2 marker values assayed between days 7
and 90 of treatment
" Patients included in analysis.
* Patients included in Cox regression analysis.
341
therapy plus surgery. Any response less than CR was considered to be
an incomplete response. Patients were classified as good or poor risk
according to their predicted probability of achieving CR calculated by
a logistic regression model using pretreatment HCG, LDH, and number
of metastatic sites (1). Patients with an NSGCT and either a predicted
probability of CR <0.50 or an extragonadal primary site were consid
ered poor risk. Patients with an NSGCT arising in the testis and a
predicted probability of CR >0.50 were considered good risk.
HCG was assayed using a modification of the highly sensitive and
specific double antibody radioimmunoassay procedure of Vaitukaitis et
al. (24). The standard HCG for this assay was obtained from National
Institute of Arthritis, Metabolism and Digestive Diseases (standard
CRII7). The antiserum against the purified /i subunit of HCG was
prepared in rabbits. A value of <2 ng/ml was considered normal. Two
assays were used to quantitate serum AFP. Prior to June 1984, a
radioimmunoassay was used with reagents kindly provided by Wampole
Laboratories, a division of Carter Wallace. A specific antiserum to
purified AFP from pooled human fetal serum was prepared in rabbits.
After June 1984, a sandwich enzyme immunoassay method from Hybritech (San Diego, CA) was used. Both the capture and signal antibod
ies were monoclonal. Both methods provide equivalent quantitative
results, but the enzyme immunoassay has an improved sensitivity of 15
ng/ml. All values for AFP >15 ng/ml were considered abnormal.
The first 10 values for HCG and AFP recorded in the clinical
chemistry department at Memorial Hospital were collected for 231
patients. Marker values were plotted semilogarithmically, and the halflife of marker decline was calculated between each point using a
computer spreadsheet program. Marker values frequently increased in
an unpredictable manner during the first 7 days after the initiation of
chemotherapy. This is consistent with release from treated, dying tumor
(18). Therefore, no pretreatment values or values measured during the
first week of therapy were used for assessment of marker half-life. The
first two values measured more than 7 days after the start of treatment
were used for all calculations of the half-life of marker decline. In order
to limit the time span under study, only values measured in the first 90
days after the start of chemotherapy were considered.
Patients were classified as having prolonged marker half-life if the
first 2 values after the seventh day of treatment were abnormal and the
half-life for AFP was >7 days or for HCG was >3 days. Marker decline
was deemed to be satisfactory if the half-life of AFP was <7 days or
HCG was <3 days or if either of the first 2 values after day 7 was
normal. Patients who had elevations of both markers were considered
to have prolonged marker half-life if either HCG or AFP half-life was
prolonged.
Hypotheses concerning differences in proportions were tested using
x2 and Fisher's exact tests and those concerning differences in medians
analysis were made with the log rank test (27). In the second analysis
utilizing Cox regression (28), survival was always calculated from the
date of the second marker value after day 7. This analysis included 176
patients, since the remaining 22 patients did not have a second marker
value prior to day 90. If both AFP and HCG were elevated, survival
was calculated from the latter of the 2 dates. Survival was always
calculated from a date within 90 days from the start of chemotherapy.
Cox regression analysis (28) was used to assess whether prolonged
marker half-life was a prognostic factor for survival. A variable, NOR
MALIZE, was defined to indicate whether markers were decaying at
the proper rate or not. NORMALIZE took the value 1 if marker halflife was prolonged and 0 if markers were decreasing satisfactorily, as
defined above. Along with known prognostic variables (see below), we
considered whether NORMALIZE was an independent prognostic
variable for survival.
Cox regression considers the logarithm (base e) of the relative risk
of death, log [\(t)/\0(t)}, to be a linear function of A-prognostic variables
Z¡,where i = 1,2
k:
AO(')
(A)
In Equation A, \(t) is the hazard function (relative rate of death) at
time t, A0(f)is a baseline hazard function (corresponding to Z, = Z2 =
. . . = Zk = 0), Z, is a value of the /th prognostic variable, and the
coefficients a¡are estimated from the data. The variables considered as
potential prognostic factors were NORMALIZE and the known prog
nostic factors (1, 19, 29): pretreatment HCG [or log (HCG + 1)],
pretreatment LDH [or log (LDH + 1)], the total number of metastatic
sites (coded as 0 for elevated markers only, 1 for one site of metastasis,
or 2 for two or more sites of metastasis), AFP [or log (AFP + I)], site
of primary tumor, and a variable termed RISK (coded as 0 for good
risk patients and 1 for poor risk patients). RISK took the value 1 if the
probability of CR (1) was calculated to be <0.5 or the primary site was
extragonadal. Otherwise, RISK took the value 0. Procedures of the
Statistical Analysis System were used for all computation (30).
RESULTS
Patient Characteristics. AFP baseline values were elevated in
151 patients, HCG values in 134 patients, and both markers in
87 patients. Patient characteristics for the 198 patients studied
are shown in Table 2.
Since marker values increased unpredictably in the first 7
days after the initiation of chemotherapy, only values measured
after the seventh day of treatment were used to calculate the
half-life of marker decay. For patients with 2 elevated marker
values after the seventh day, the half-life between the first 2
values was calculated and results are shown in Table 3. Both
AFP and HCG half-lives were significantly prolonged in those
patients not achieving a CR.
Half-life values were calculated in this way; patients whose
AFP half-life was >7 days or whose HCG half-life was >3 days
had significantly shorter survival and achieved CR less fre
quently. The cutoff values of 7 days and 3 days were chosen
prospectively, based on the expected biological half-lives. Even
though the median half-life of HCG decline in patients achiev
ing CR with chemotherapy was 3.5 days, a cutoff of 3 days was
used, because only 2 patients had a half-life for HCG between
3 and 4 days and neither achieved a prolonged CR.
Response Proportions and Relapse. Proportions of CR ac
of continuous data using the Wilcoxon test (25). Survival distributions
cording to prolonged or satisfactory decline of serum markers
were estimated by the method of Kaplan and Meier (26), and univariate
are shown in Table 4. If prolonged half-life of either AFP or
comparisons were made using the log rank test (27).
HCG were considered separately, each was capable of identi
Two analyses were performed. In the first analysis of 198 patients,
fying a group of patients less likely to achieve CR. If patients
survival was calculated from the time the patient was deemed to have
satisfactory markers or a prolonged half-life. This was at the date of with a prolonged half-life of either marker were included in a
single group, a larger, more clinically useful group of 42 patients
the first marker value after day 7 if this value was normal or at the date
of the second marker value otherwise. Comparisons of survival in this
was identified. Only 12 of these 42 patients (29%) achieved a
5905
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.
HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
Table 2 Characteristics
of 198 patients
with elevated AFP or HCG
risk2813-54118(100%)0018(16%)51risk2615-5155
PatientsAge
(yr)MedianRangePrimary
siteTestisMediastinumRetroperitoneumNo.
(69%)14(17%)11
sites0Markers
of metastatic
only1>2Chemotherapy
elevated
(7%)1
(6%)18(9%)61
1
(14%)0
(0%)10(12%)70
(31%)117(60%)75642930151
(44%)47
(40%)54640091
(88%)210293060
regimenVAB-6*-rVAB-6
EPfVAB-6
vi.
EP*CBE'AFPElevatedMedian
+
(76%)25616-139.600134(68%)642.2-44.500141
(77%)16518-10.40071
(75%)45316-139.60063
(ng/ml)Range
elevated value
(ng/ml)HCGElevatedMedian
(60%)192.5-3.80063
(79%)1.4922.2-44.50078
(ng/ml)Range
elevated value
(ng/ml)LDH°ElevatedMedian
(54%)347239-1.440Poor
(98%)771240-16.629
(72%)493239-16.629Good
(units/liter)Range
elevated value
(units/liter)All2613-54173(87%)14
°Adequale data available in 196 patients.
* Ref. 22.
' Ref. 5.
" Ref. 23.
' Ref. 8.
' VAB-6. cyclophosphamide + vinslastine + bleomycin + dactinomycin + cisplatin: EP. etoposide + cisplatin; CBE. carboplatin + bleomycin + etoposide.
Table 3 Correlation of response and marker half-life calculated between the first
and second marker values measured after day 7 of chemotherapy, for 66 patients
in whom both the first and second values were abnormal
Table 4 Correlation
of response with prolonged
marker half-life
CR. All CR IR
chemo
N % N % N % P value*
value*0.0170.037
ResponseAFP
Response
half-lifeNo.
All
patients
patientsMedian
of
AFP or HCG half-life prolonged (N = 42)
819
12293071
(davs)Range
Satisfactory AFP and HCG (A/= 156)
126 81 139 89 17 11 <0.0001
(days)HCG
half-lifeNo.
AFP half-life >7 days (N = 16)
3 19
5 31 11 69
patientsMedian
of
Satisfactory AFP (N = 129)
99 77 111 86 18 14 <0.0001
(days)Range
HCG half-life >3 days (N = 29)
5 17
7 24 22 76
(days)CR-chemo"175.93.3-35.783.52.5-62.4AIICR206.13.3-Inc104.22.5-62.4IR1813.33.2-Inc2718.30.9-lncP
Satisfactory HCG (A"= 102)
82 80 91 89 11 11 <0.0001
°CR-chemo. complete response to chemotherapy alone: All CR, all complete
responses, including CR-chemo; IR. incomplete response: Inc. increasing marker
Good risk patients
value, half-life not valid.
AFP or HCG half-life prolonged (N = 9)
111
4 44 5 56
* Wilcoxon test comparing all CR with incomplete responses.
Satisfactory AFP and HCG (N = 109)
97 89 106 97 3 3 <0.0001
CR, compared with 139 of 156 patients (89%) with satisfactory
marker values (x2 = 63.67, l d.f., P < 0.0001).
Twelve patients who had prolonged marker half-life achieved
a CR. Residual viable malignancy was resected after chemo
therapy more frequently in this group of patients. Four of the
12 patients (33%) had residual malignancy resected compared
to 13 of 139 patients (9%) who were found to have satisfactory
marker decay (Fisher's exact test, P = 0.03). Relapse also
occurred much more frequently; 8 of the 12 patients (67%) with
abnormal marker half-life relapsed after CR compared to 18 of
139 patients (13%) with satisfactory markers (Fisher's exact
Poor risk patients
AFP or HCG half-life prolonged (N = 33)
Satisfactory AFP and HCG (N = 47)
7 21
29 62
8 24 25 76
33 70 14 30
0.0001
Cox regression patients
AFP or HCG half-life prolonged (N = 42)
8 19 12 29 30 71
Satisfactory AFP and HCG (N = 134)
105 78 118 88 16 12 <0.0001
°CR-chemo, complete response to chemotherapy alone; All CR. all complete
responses, including CR-chemo: IR, incomplete response.
X2test.
Patients with prolonged marker half-life had dramatically
shorter survival compared to the other patients (log rank x2 =
66.4, l d.f., P < 0.0001). Only 6 patients with prolonged marker
half-life were alive >24 months from the start of treatment.
test, P = 0.0001). The 13% relapse rate is slightly higher than
Three of these 6 patients had viable malignancy resected after
expected for an overall group of patients with germ cell tumors,
chemotherapy; 1 additional patient relapsed 13 months after
but this was probably due to the worse prognosis of patients
starting chemotherapy and has remained alive with disease at
who were selected for this analysis because they had an NSGCT
35+ months. Only 2 patients with prolonged marker half-life
and elevated markers.
achieved a CR with chemotherapy alone and remained alive
Proportions of CR are shown in Table 4 for Memorial
and free of disease >24 months (32+ and 69+ months) after
Hospital good and poor risk patient groups (1). Prolonged
marker half-life identified patients within each group who starting treatment.
Prolonged half-life of both AFP and HCG could be used
achieved a CR less frequently.
Survival Analysis. Survival for all patients is shown in Fig. 1. individually to identify a group of patients with shorter survival
5906
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.
HALF-LIFE OF SERUM Tl'MOR
MARKIÕR!>!•:<
LINK IN NSGCT
A 100*
100*
80%
Satisfactory
(156
pts,
Satisfactory
(109
pts.
80*
Markers
129 olive)
60«
n
(/I
Markers
100 alive)
60*
40*
o
o.
o
i
Prolonged
20*
Prolonged
(42
Marker
pts,
oÃ- 20*
Half-Life
(9
Marker
pts,
Half-Life
3 alive)
12 alive)
0%
2
4
Years
B
100*
80*
en
co
c
o
100*
8
10
Years
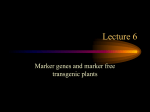
Fig. 1. Survival for 198 patients according to abnormal or satisfactory decay
of AFP and HCG after initiation of chemotherapy (log rank test, x2 = 66.37, 1
d.f.,/>< 0.0001).
/\
6
r
-
r
60*
80*
Satisfactory
(129
pts,
60*
AFP
103 alive)
Satisfactory
(47 pts,
Markers
29 alive)
40*
o
a.
o
Q_
40*
20*
Prolonged
(33
Prolonged
20*
(16
AFP
pts,
Marker
pts,
9 alive)
4
6
Half —Life
Half-Life
5 alive)
10
Years
0%
246
8
10
Years
100*
-
eluded from this analysis because they had normal pretreatment
AFP and HCG values (Table 1), had longer survival compared
to all of the 266 patients (Table 1) with initial marker elevation
(log rank x2 —4.5, P = 0.03). This supports the notion that
80*
Satisfactory
(102
pts,
HCG
85 alive)
60*
•f 40*
o
o
¿
Fig. 3. A. survival for 118 good risk patients according to abnormal or
satisfactory decay of AFP and HCG after initiation of chemotherapy (log rank
test, x2 = 3 1.67, l d.f., P < 0.000 1). B, survival for 80 poor risk patients according
to abnormal or satisfactory decay of AFP and HCG after initiation of chemo
therapy (log rank test, x2 = 10.57. I d.f.. P = 0.0012).
I
'"•"'
Prolonged
j (29 pts,
HCG Half-Life
7 alive)
20*
O*
10
Years
Fig. 2. A. survival for 145 patients with initially elevated AFP according to
abnormal or satisfactory decayof AFP after initiation of chemotherapy (log rank
test, x! = 21.74, l d.f., P < 0.0001). fi, survival for 131 patients with initially
elevatedHCG according lo abnormal or satisfactory decayof HCG after initiation
of chemotherapy (log rank test. x2 = 64.02.1 d.f.. P < 0.0001).
patients selected for inclusion in the analysis because they had
initially elevated AFP or HCG values had a worse prognosis.
Cox regression analysis was used to derive independent prog
nostic variables for survival. In this analysis, survival was always
measured from the date of the second marker value after the
seventh day of treatment. Twenty-two of the 198 patients
studied were excluded from the Cox regression. All of these
patients had a normal value for the first marker assay after the
seventh day but did not have a second marker assay before the
90th day. CR proportions for the 176 patients included in the
Cox regression are shown in Table 4.
The Cox model yielded NORMALIZE as the most signifi
cant prognostic factor among the variables considered and
RISK as a second independent prognostic factor. None of the
other variables entered the Cox model, and these 2 prognostic
variables did not have a significant interaction. The final model
was
(Fig. 2). Fourteen patients had prolonged half-life of one marker
but satisfactory values for the other. Seven of these 14 patients
(50%) achieved a CR, but only 4 remained continuously alive
and free of disease after therapy. Thus, patients who had only
Mt)
= 1.29 NORMALIZE
+ 1.41 RISK
(B)
log
one abnormal marker, while the other was satisfactory, had a
poor prognosis. Therefore, analyses of marker half-lives of both
This model has an overall x2 (score statistic) of 76.15, 2 d.f.,
HCG and AFP should be considered complementary. In addi
tion, prolonged marker half-life identified a group of patients
and a P< 0.0001.
with shorter survival within both the good risk and poor risk The model yields four prognostic groups of patients. Kaplan(Fig. 3) patient subgroups.
Meier plots of survival for these groups are displayed in Fig. 4.
Seventy-five patients with NSGCT, who were otherwise ex- The survival curves are very similar to those for the original
5907
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.
HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
100%
Good
Markers
Good
Markers,
&
Risk
80*
n
c/1
6056
~
o
o.
o
40*
CL
20*
Poor
Risk
Bad
Markers,
Good
Risk
Bad
Markers,
Poor
Risk
4
6
10
Years
Fig. 4. Survival for 176 patients included in the Cox regression analysis
according to abnormal or satisfactory decay of AFP and HCG and good or poor
risk patient group. Includes 92 good risk patients with satisfactory markers (85
alive). 42 poor risk patients with satisfactory markers (25 alive), 9 good risk
patients with prolonged AFP or HCG half-lives (3 alive), and 33 poor risk patients
with prolonged AFP or HCG half-lives (9 alive).
198 patients as shown in Fig. 3. For patients in the same RISK
group (good or poor risk), the relative risk of dying for those
with prolonged marker half-life compared to those with satis
factory markers was 3.63. This means that there was >3-fold
risk of death for those whose elevated markers did not decline
appropriately. For patients in the same NORMALIZE group,
the risk of dying for poor risk patients relative to good risk
patients was 4.10. This implies approximately a 4-fold risk of
death for poor risk patients compared to good risk patients.
After inspection of the coefficients in Equation B, the hy
pothesis that the two coefficients were equal was generated.
This hypothesis was tested and confirmed. This meant that a
Cox model could be generated with a single independent vari
able taking the value 0 for good risk patients with markers
normalizing appropriately, the value 1 for good risk patients
with markers not normalizing appropriately or poor risk pa
tients with markers normalizing appropriately, and the value 2
for poor risk patients whose markers were not normalizing
appropriately. There was then a relative risk of dying of 3.82
for one of these groups relative to the adjacent better one. This
model is not reported in more detail because it was suggested
only by the results of the first Cox regression analysis and lacks
clinical applicability.
Similar results were found when Cox regression was under
taken separately in the good and poor risk patient subgroups.
These analyses were limited by small numbers of patients.
NORMALIZE was the only variable to enter the model for
poor risk patients and NORMALIZE and LDH were the only
variables for good risk patients.
of individual prognostic variables, decision algorithms used
internationally to classify good and poor risk patients have
generally recognized baseline tumor marker levels and bulk of
disease as the most important predictive factors for response
(19). These pretreatment prognostic factors have been used to
decide what treatment program should be recommended for an
individual patient.
Exploration of possible prognostic features evident only after
the initiation of chemotherapy has been limited. Almost all
current treatment programs await assessment of response after
the completion of 3 or 4 cycles of chemotherapy before deci
sions regarding further treatment are considered. Assessment
of response frequently involves surgical exploration and resec
tion of residual disease in the retroperitoneum and chest.
Several studies of fewer patients have suggested that a pro
longed half-life of marker decline may have prognostic impli
cations (15, 18, 21, 33). The therapeutic usefulness of this
information has, however, remained ill defined. The data in this
report demonstrate that prolonged decay of markers compared
to expected biological half-life is a powerful predictor of failure
to respond and poor survival. Patients in whom a prolonged
marker half-life was identified had a CR proportion of 31% and
most patients achieving CR subsequently relapsed. Only 5 of
42 patients (12%) remained alive and free of disease >24
months from the start of treatment. It is possible that some of
the long-term survivors were salvaged from chemotherapyresistant malignancy by complete resection of residual malig
nancy after chemotherapy. Abnormal marker decline identified
a poor prognosis subset of patients within both good and poor
risk patient groups.
Cox regression analysis selected prolonged marker decay as
the most significant predictor of limited survival. The only
other independent prognostic factor for survival was good or
poor risk patient category. The risk categorization was in turn
derived from the primary site (all extragonadal tumors consid
ered poor risk) and a mathematical formula which uses pretreat
ment HCG, LDH, and the number of sites of metastatic disease
to predict the chance of achieving a CR. No other potential
prognostic factor entered the model. This result indicates the
importance of prolonged marker half-life as a predictor of poor
survival. It also confirms that our existing risk stratification,
which was derived from a logistic regression analysis of re
sponse, also predicts survival more powerfully than individual
pretreatment variables and independently of the analysis of
marker half-life. This substantiates the hypothesis that posttreatment clinical variables can complement pretreatment risk
stratification.
Can the prognostic implications of marker half-life analysis
be used to the patients' advantage? Once a treatment program
has been initiated, why not wait until response is assessed at
the completion of therapy? While these questions require eval
uation in prospective studies, there are strong theoretical rea
DISCUSSION
sons to suggest that an early change of chemotherapy regimen
may be of benefit to those patients identified with a poor
This study shows that assessment of the decline of serum
prognosis. The median time to classification of patients accord
tumor markers after the initiation of chemotherapy is a pow
ing to marker half-life in this study was 33 days after the start
erful prognostic tool. The identification and utilization of prog
nostic factors has made possible the rational development of of treatment. This is much briefer than the 3-6 months usually
treatment programs for germ cell tumors. Clinical trials for required to assess response. An early change to a more intensive
patients with a good prognosis have demonstrated that fewer regimen may avoid the problem of cumulative toxicities from
cycles of treatment (6, 31) and fewer cytotoxic agents (5) can chemotherapy and the potential development of chemotherapy
resistance. For example, good risk patients may benefit from a
be used without jeopardizing response proportions and survival
change to a more intensive chemotherapy combination contain
outlook. The aims of trials for patients with a poor prognosis
ing ifosfamide. Poor risk patients with abnormal marker halfhave been to increase the frequency of CR without intolerable
toxicity (23, 32). Although disagreement exists over the weight
life may benefit from a change to therapy such as high dose
5908
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.
HALF-LIFE
OF SERIAI
TIMOR
MARKER
chemotherapy with autologous stem cell support. The latter
option is currently the subject of prospective evaluation in a
clinical trial at Memorial Hospital.
Previous reports have suggested the value of monitoring
tumor marker half-life (15, 18, 21, 33-35). The majority of
these studies have compared the marker levels prior to chemo
therapy with the level at the time of the second cycle of
treatment. Some studies have found this to be useful (21). while
others have not (34). The likely reason for this discrepancy, and
the potential flaw in this methodology, is that such an analysis
fails to consider an initial increase in serum tumor marker
levels which may occur at the initiation of chemotherapy. This
phenomenon has been well described and is unpredictable, in
that some patients have no increase while others may have
elevations up to 600% of baseline (18, 20). This elevation makes
comparisons of half-lives calculated from marker values meas
ured prior to and immediately after treatment unreliable. In
this study, the first marker value considered was always taken
after the seventh day of treatment. In our experience, the peak
in marker levels occurred prior to this time. In addition, some
published reports have monitored only HCG (21 ). This analysis
demonstrates that both HCG and AFP can be useful individ
ually and when used together provide increased accuracy.
Two criticisms of this study are that all data were collected
retrospectively and that marker values were often measured
infrequently during initial treatment. Patients treated in the
last 10 years were included and markers were less regularly
measured a decade ago. We were unable to measure marker
half-life for each patient using many data points but, instead,
restricted the analysis to the potentially less accurate method
of measuring it from 2 points only. Of the 156 patients with
"satisfactory markers," 132 were classified by the fact that their
markers had returned to normal values rather than by measure
ment of the half-life of marker decay. Nonetheless, it is clear
that analysis of marker values after initiation of chemotherapy
provides powerful prognostic information. It is likely that the
most accurate method of assessing marker decline would be by
measurement of multiple elevated values after the first week of
treatment, with measurement of a best fit half-life applied to
the data. This does not require excessively complicated analysis,
because the calculations can be easily performed in a number
of currently available personal computer programs. These re
sults have led us to consider the more complex decline in LDH.
It is possible that further prognostic information may be dis
cerned from the decline in LDH, particularly in patients with
initially normal AFP and HCG values.
This study demonstrates that prolonged decay of AFP or
HCG after chemotherapy identifies patients unlikely to achieve
CR or long-term survival. These patients may benefit from an
early change in treatment. We recommend that all patients with
NSGCT receiving chemotherapy be monitored with weekly
assays for AFP and HCG until these markers have normalized.
Patients enrolled in clinical trials should be prospectively mon
itored to confirm the significance of prolonged marker half-life.
Patients who are not receiving treatment in a clinical trial and
who are found to have an abnormal decay of markers should be
referred to a major treatment center so that a change to more
intensive therapy can be considered.
REFERENCES
1. Bosl. G. J.. Geller. N. L., Cirrincione, C.. Vogelzang, N. J.. Kennedy. B. J..
Whitmore. W. F.. Jr., Vugrin. D.. Scher, H.. Nisselbaum. J.. and Golbcy. R.
B. Multivariatc analysis of prognostic variables in patients with metastatic
testicular cancer. Cancer Res., 43: 3403-3407. 1983.
DECLINE
IN NS(.< I
Geller, N. L., Bosl. G. J., and Chan, E. Y. Prognostic factors for relapse
after complete response in patients with metastatic germ cell tumors. Cancer
(Phila.). 63: 440-445, 1989.
Toner, G. C., Lin, S-Y.. Geller. N. L.. Ochoa, M., and Bosl. G. J. Survival
and prognostic features of extragonadal and poor risk nonscminomatous
germ cell tumors. Proc. Am. Assoc. Cancer Res.. 30: 259. 1989.
Bosl. G. J., Geller. N. L., and Chan, E. Y. W. Stage migration and the
increasing proportions of complete responders in patients with advanced
germ cell tumors. Cancer Res.. 48: 3524-3527. 1988.
Bosl, G. J.. Geller. N. L., Bajorin. D.. Leitner, S. P., Yagoda. A.. Golbcy. R.
B.. Scher. H.. Vogelzang. N. J.. Auman, J.. Carey, R., et al. A randomized
trial of etoposide -t- cisplatin versus vinblastine + bleomycin + cisplatin +
cyclophosphamide + dactinomycin in patients with good-prognosis germ cell
tumors. J. Clin. Oncol.. 6: 1231-1238, 1988.
Einhorn, L. H., Williams, S. D.. Loehrer, P. J., Birch, R.. Drasga, R., Omura,
G., and Greco, F. A. Evaluation of optimal duration of chemotherapy in
favorable-prognosis disseminated germ cell tumors: a Southeastern Cancer
Study Group protocol. J. Clin. Oncol., 7: 387-391, 1989.
Motzer. R.. Geller. N., Bajorin. D.. Scher. H.. Tan. C.. Hen. H.. Sogani. P..
Fair. W.. Morse. M.. Russo. P.. and Bosl, G. Salvage chemotherapy for germ
cell tumor patients: prior complete response as an important prognostic
variable (Abstract). Proc. Am. Soc. Clin. Oncol.. 9: 141, 1990.
Motzer, R. J.. Cooper, K.. Geller, N. L., Pfister, D. G.. Lin, S-Y., Bajorin.
D.. Scher. H. !.. Herr. H.. Fair. W.. Morse. M., Sogani. P.. Whitmore. W.,
and Bosl. G. J. Carboplatin + etoposide + bleomycin for patients with poor
risk germ cell tumors. Cancer (Phila.). 65: 2465-2470. 1990.
9. Bajorin. D.. Katz. A.. Chan. F.. Geller. N.. Vogelzang. N., and Bosl, G. J.
Comparison of criteria for assigning germ cell tumor patients to "good risk"
and "poor risk" studies. J. Clin. Oncol.. 6: 786-792. 1988.
10. Bosl. G. J., Geller, N. L., Cirrincione, C., Nisselbaum, J., Vugrin. D.,
11.
12.
13.
14.
15.
16.
17.
Whitmore. W. F.. Jr.. and Golbey. R. B. Serum tumor markers in patients
with metastatic germ cell tumors of the testis: a ten year experience. Am. J.
Med.. 75: 29-35. 1983.
Lange. P. H.. and Fraley. E. E. Serum alpha-fetoprotein and human chorionic
gonadotropin in the treatment of patients with testicular tumors. L'rol. Clin.
North. Am.. 4: 393-406. 1977.
Bosl. G. J., Lange. P. H.. Fraley. E. E., Goldman. A., Nochomovitz, L. E.,
Rosai, J., Waldmann. T. A.. Johnson. K.. and Kennedy. B. J. Human
chorionic gonadotropin and alphafetoprotein in the staging of nonseminomatous testicular cancer. Cancer (Phila.). 47: 328-332. 1981.
Bosl. G. J.. Lange. P. H.. Nochomovitz, L. E., Goldman, A.. Fraley. E. E.,
Rosai. J.. Johnson. K.. and Kennedy. B. J. Tumor markers in advanced
nonseminomatous testicular cancer. Cancer (Phila.). 47: 572-576, 1981.
Loehrer. P. J., Sr.. Williams. S. D.. and Einhorn, L. H. Tcsticular cancer:
the quest continues. J. Nati. Cancer. Inst., 80: 1373-1382. 1988.
Lange. P. H.. Vogelzang. N. J., Goldman. A.. Kennedy. B. J.. and Fraley, E.
E. Marker half-life analysis as a prognostic tool in testicular cancer. J. Imi.
128: 708-711. 1981.
Gillin. D.. and Boesman. M. Serum »-fetoprotein. albumin and vglobulin
in the human conceptus. J. Clin. Invest.. 45: 1826-1838. 1966.
Wehmann. R. E., and Nisula. B. C. Metabolic and renal clearance rates of
purified human chorionic gonadotropin. J. C'lin. Invest.. 68: 184-194. 1981.
18. Vogelzang, N. J.. Lange. P. H.. Goldman. A.. Vessela. R. H.. Fraley. E. E.,
and Kennedy. B. J. Acute changes of »-fetoprotein and human chorionic
gonadotropin during induction chemotherapy of germ cell tumors. Cancer
Res.. «.-4855-4861. 1982.
19. Vogelzang, N. J. Prognostic factors in metastatic testicular cancer. Int. J.
Andrò!.. IO: 225-237. 1987.
20. Horwich, A., and Peckham, M. J. Transient tumor marker elevation follow
ing chemotherapy for germ cell tumors of the testis. Cancer Treat. Rep.. 70:
1329-1331, 1986.
21. Picozzi. V. J., Freiha, F. S.. Hannigan, J. F., and Torti, F. M. Prognostic
significance of a decline in serum human chorionic gonadotropin levels after
initial chemotherapy for advanced germ-cell carcinoma. Ann. Intern. Med..
100: 183-186.1984.
22. Bosl. G. J.. Gluckman. R.. Geller, N. L.. Golbey. R. B.. Whitmore. W. F..
Jr.. Herr. H.. Sogani, P., Morse. M., Martini. N., Bains. M.. and McCormack. P. V'AB-6: an effective chemotherapy regimen for patients with
germ cell tumors. J. Clin. Oncol.. 4: 1493-1499. 1986.
23. Bosl. G. J., Geller, N. L.. Vogelzang, N. J.. Carey. R.. Auman. J.. Whitmore.
W. F., Herr, H.. Morse. M., Sogani, P., and Chan, E. Alternating cycles of
etoposide plus cisplatin and VAB-6 in the treatment of poor-risk patients
with germ cell tumors. J. Clin. Oncol., 5: 436-440. 1987.
24. Vaitukaitis. J. L.. Braunstein. G. D., and Ross, G. T. A radioimmunoassay
which specifically measures human chorionic gonadotropin in the presence
of human leutinizing hormone. Am. J. Obstet. Gynecol.. 113: 751-758,
1972.
25. Zar. J. H. Biostatistical Analysis. Englewood Cliffs. NJ: Prentice Hall Inc..
1974.
26. Kaplan. E. L.. and Meier. P. Nonparametric estimation from incomplete
observations. J. Am. Slat. Assoc., 53:457-481. 1958.
27. Mantel. N. Evaluation of survival data and two new rank order statistics
arising in its consideration. Cancer Chemother. Rep.. 50: 163-170, 1966.
28. Kalbfleisch. J. D.. and Prentice. R. L. The Statistical Analysis of Failure
Time Data. New York: John Wiley & Sons, 1980.
29. Droz, J. P., Kramar. A.. Ghosn. M., Piot, G., Rey, A., Theodore. C., Wibault,
P.. Court. B. H.. Perrin. J. L.. Travagli. J. P.. Bellet. D., Caillaud. J. M.,
Pico. J. L.. and Hayal. M. Prognostic factors in advanced nonscminomalous
5909
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.
HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
lesticular cancer. A multivarialc logistic regression analysis. Cancer (Phila.).
62- 564-568 1988
30. SUGI Supplemental Library User's Guide. 1987 ed.. pp. 269-293. 437-466.
f
Mf~. CAS i« i»i„„
lasi
vary,iNi..jv\.>insiiiuii.ini..,
ITO/.
31. Einhorn. L. H.. Williams. S. D.. Trôner. M.. Birch. R., and Greco. F. A. The
chemotherapy regimen in the treatment of poor prognosis nonseminomatous
germ-cell tumors. J. Clin. Oncol., 6: 10.11-1040, 1988.
-"•Thompson. D. K.. and Haddow. J. E. Serial monitoring of serum alphafetoprotem
and chononic gonadotropm in males with germ cell tumors.
.-,
/ph'i.\^?.iii^nift'^Qio"7Q
,4 Horwjch A' and Peckham. M. J. Serum tumor regression rate following
role of maintenance therapy in disseminated tcsticular cancer. N. Engl. J.
Med..J05: 727-731. 1981.
32. Ozols. R. F.. Ihde. D. C.. Lineham. W. M.. Jacob. J.. Ostchega. Y.. and
Young. R. C. A randomized trial of standard chemotherapy r a high-dose
chemotherapy for malignant teratoma. Eur. J. Cancer. Clin. Oncol.. 20:
1463-1470. 1984.
35. Carl. J. Drug-resistance patterns assessed from tumor marker analysis. J.
Nail. Cancer. Ina., SI: 1631-1639. 1989.
5910
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.
Serum Tumor Marker Half-Life during Chemotherapy Allows
Early Prediction of Complete Response and Survival in
Nonseminomatous Germ Cell Tumors
Guy C. Toner, Nancy L. Geller, Claire Tan, et al.
Cancer Res 1990;50:5904-5910.
Updated version
E-mail alerts
Reprints and
Subscriptions
Permissions
Access the most recent version of this article at:
http://cancerres.aacrjournals.org/content/50/18/5904
Sign up to receive free email-alerts related to this article or journal.
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Department at [email protected].
To request permission to re-use all or part of this article, contact the AACR Publications
Department at [email protected].
Downloaded from cancerres.aacrjournals.org on June 11, 2017. © 1990 American Association for Cancer Research.