Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Original article
1327
Main results of the losartan versus amiodipine (LOA) study on
drug tolerability and psychological general well-being
Björn Dahlöf, Lars H. Lindholm*, Shane Carney †, Pertti J. Pentikäinen‡ and
Jan Östergren § for the LOA Study group
Objective To compare two losartan regimens (with and
without hydrochlorothiazide) and amiodipine in treating
mild-to-moderate hypertension regarding their bloodpressure-lowering effect, drug tolerability and quality of
life.
Design A 12-week, randomized, double-blind, parallelgroup, multi-centre study. After 4 weeks of placebo,
patients with a diastolic blood pressure (DBP) in the
range 95-115 mmHg were allocated randomly to be
administered 50 mg losartan (increased to 100 mg if the
DBP was 90 mmHg or more after 6 weeks), 50 mg
losartan (plus 12.5 mg hydrochlorothiazide under the
above conditions), or 5 mg amiodipine (increased to 10
mg under the above condition). The tolerability of the
treatment and the quality of life were evaluated by
spontaneous reporting, active questioning and the
Psychological General Well-Being (PGWB) index.
Study population In total 898 hypertensives, mainly
referred from primary health care (mean age 57.8 years)
of whom 52% were men.
Results Administration of 50 mg losartan (plus 1 2.5
hydrochlorothiazide if necessary) and of 5 mg amiodipine
(or 10 mg if necessary) lowered the blood pressure as
well as or better than did 50 mg losartan (or 100 mg if
necessary). The incidence of any discomfort' and
'swollen ankles' increased with amiodipine but not with
losartan treatment. The opposite was found for 'dizziness
upon standing'. The incidence of drug-related adverse
events and the number of patients withdrawn from
therapy were higher with amiodipine than they were with
losartan treatment. The PGWB index at week 12
indicated that improvements from baseline had occurred
in some domains for the losartan groups whereas it
remained unchanged for the amlodipine group.
Conclusion Both losartan and amiodipine were effective
in lowering the blood pressure and were tolerated well.
Administration of 50 mg losartan (plus 12.5 mg
hydrochlorothiazide if necessary) and of 5 mg amlodipine
(or 10 mg if necessary) lowered the blood pressure
equally well or better than did 50 mg Iosartan (or 100 mg
if necessary). Drug-related adverse effects and
withdrawal from the study were more common for the
amlodipine group. The clinical significance of the
improvements in the PGWB index with losartan needs to
be studied further.
Journal of Hypertension 1997, 15:13 27-1335
Keywords: amlodipine, general well-being, hypertension, losartan,
tolerability, quality of life
From the Clinical Trial Unit, Department of Medicine, Sahlgrenska University
Hospital/Östra, Göteborg, Sweden, the *Department of Community Health
Sciences, Lund University, Lund, Sweden, the †Division of Medicine, John
Hunter Hospital, University of Newcastle, Australia, the ‡ Department of
Medicine, Helsinki University. Helsinki, Finland, and the §Department of
Medicine, Karolinska Hospital, Stockholm, Sweden.
Sponsorship: Financial support was provided by Merck & Co. Inc.
Requests for reprints to Dr Lars H. Lindholm, Department of Community
Health Sciences, Lund University, Helgeandsgatan 16, S-223 54 Lund,
Sweden.
Received 20 February 1997 Revised 1 July 1997
Accepted 2 July 1997
© Rapid Science Publishers
ISSN 0263-6352
Introduction
Pharmacological treatment of arterial hypertension is one
area in medicine that has shown remarkable progress
and development during recent decades. This-is true not
only with regard to the number of efficacious and
generally well-tolerated antihypertensive drugs that
have become available but also to the substantial
documentation of a clinically relevant reduction in
cardiovascular morbidity and mortality brought about
by antihypertensive drug treatment [1]. We now have a
choice of effective blood-pressure-lowering agents
with better and better drug
tolerability. β-Blockers and diuretics are the drug classes
so far shown to reduce cardiovascular morbidity and
mortality risk [2,3] but have at the same time been
linked to a number of well-known side effects [1,4].
'Newer' treatment regimens have been shown to be
tolerated well in general by hypertensive patients but
have also been associated with specific side effects [e.g.
calcium antagonists with ankle oedema [1,5,6],
angiotensin converting enzyme (ACE) inhibitors with
coughing [7,8] and
-blockers with orthostatic
hypotension [1]]. Members of one of the newest
antihypertensive classes of drugs avail-
1328 Journal of Hypertension 1997, Vol 15 No 11
able, namely the selective angiotensin II antagonists, have
shown promising results in terms of their improved drug
tolerability, few drug-specific side effects and satisfactory
blood-pressure-lowering effects [9-11].
Table 1
Needless to say, the ultimate goal for the treatment of
high blood pressure is to prevent or delay cardiovascular
disease. This has not yet been established to be achieved
in hypertensives for most of the 'newer' blood-pressurelowering drugs (α-blockers, ACE inhibitors, calcium
antagonists and selective angiotensin II antagonists),
however. One prerequisite for a satisfactory effect on the
blood pressure is that the patient be compliant and ingest
his or her medication as prescribed. A large follow-up
survey in the United Kingdom showed that less than 50%
of the patients were continuing their initial antihypertensive therapy after 6 months [12]. There are of course
many reasons for a patient to discontinue drug therapy
for a chronic disease. A lack of effect is one, drug-related
side effects and an impaired quality of life are others. It
is believed generally that the 'newer' drugs, having fewer
side effects, maintain general well-being better than do blockers and diuretics [13]. This is likely to lead to
better patient compliance.
Men (%)
53
53
52
Age (years)
Aged < 65 years (%)
Aged 65-74 years (%)
Aged > 74 years (%)
Caucasians (%)
Severity of hypertension
Mild (DBF 95-105 mmHg) (%)
Moderate
(DBF 106-115 mmHg) (%)
Laboratory values
Blood glucose (mmol/l)
Serum cholesterol (mmol/l)
Serum triglycerides (mmol/l)
57.8
71
24
5
98
57.9
57.8
Large prospective studies concerning cardiovascular
morbidity and mortality are under way comparing calcium
antagonists, ACE inhibitors and angiotensin II antagonists
with β-blockers and diuretics [14]. While awaiting the
outcome of these trials, we could and probably should
evaluate the effects on intermediate (surrogate) endpoints
of the 'newer' antihypertensive drugs as well as their
impact on tolerability and general well-being. For many
years, drug tolerability was evaluated only with structured
interviews on specific symptoms (e.g. tiredness, ankle
oedema and coughing). Studies on the quality of life and
well-being really began to evolve with the publication of
a comparison of captopril, propranolol and methyldopa by
Croog e.t al. [15] in 1986 using, among other things, a
psychological general well-being (PGWB) index.
Compositions of the study groups at baseline
A
Losartan
monotherapy
(n = 300)
B
Losartan
plus HCTZ
(n = 300)
C
Amlodipine
monotherapy
(n = 298)
70
22
8
100
72
23
5
100
68
72
74
29
26
24
5.5
6.1
1.7
5.4
6.1
5.6
6.1
1.6
1.7
HCTZ, hydrochlorothiazide; DBF, diastolic blood pressure.
At baseline, the groups did not differ regarding age,
sex distribution, heart rate (73-74 beats/min), and prevalences of other diseases such as cardiovascular disease
(16-23%), diabetes mellitus (6-7%), musceloskeletal
disease (39-41%), neurological and psychiatric disorders
including migraines and headaches (25-26%) and respiratory diseases (20-22%). Blood pressure values at baseline are given in Table 2 and the severity of hypertension
and blood lipid levels in Table 1. The vast majority of
the patients was recruited from primary health care. The
six key exclusion criteria (of 22 applied) were that we
excluded women of childbearing age, those with significant renal impairment, those who had suffered myocardial
infarction within the last 6 months, those who had angina
pectoris, those who had congestive heart failure, those
who were being administered β-blockers and oth
antihypertensive drugs and those who had previous.,
been treated with angiotensin II antagonists and calcium
antagonists.
Study design
The overall aim of the present study was to compare two
losartan treatments [with and without hydrochlorothiazide
(HCTZ)] and amlodipine in treating mild-to-moderate
hypertension concerning their blood-pressure-lowering
effect, drug tolerability and the quality of life using the
PGWB index.
Study population and methods
In total, 898 patients with mild-to-moderate hypertension
were included in the study; 637 (71%) came from Sweden,
150 (17%) from Australia and 137 (12%) from Finland.
Their baseline characteristics are given in Table 1; 52%
were men. The men were aged 56.3 ± 1 1 . 4 years
(mean ± SD) and the women 59.5 ± 9.9 years; almost all
were Caucasians.
The study was a 12-week, multi-centre (63 centres),
randomized, double-blind, double-dummy, parallel-group
trial. After 4 weeks of placebo, patients with a diastolic
blood pressure in the range 95-115 mmHg when they
were seated were allocated randomly to be administered
either 50 mg losartan (groups A and B) or 5 mg amlodipine
(group C) in a ratio of 2 : 1. If the diastolic blood pressure
remained above 90 mmHg after 6 weeks of therapy,
100 mg losartan was administered to subjects in group A,
50 mg losartan plus 12.5 mg HCTZ to subjects in
group B and 10 mg amlodipine to subjects in group C for
the remaining 6 weeks of the study. All of the drugs were
administered once a day, in the morning. Patients who
had been being administered blood-pressure-lowering
drug treatment at the time of their recruitment went
without antihypertensive drugs for a minimum of 7 days
before starting the placebo period.
Quality of life during losartan treatment Dahlöf et al.
1329
Table 2 Systolic blood pressures (SBP) and diastolic blood pressure (DBP) of sitting patients at baseline and
during week 12
Treatment groups
Baseline
(mmHg)
Week 1 2
(mmHg)
Mean change
from baseline
(mmHg)
95% Confidence
interval (mmHg)
Significance
(P)
161.9 ±16.4
148.3 ± 17.7
-13.6
-1 5.0 to -1 1 .9
< 0.001
160.5 ±17.0
143.4 ± 16.6
-17.1
-18.5 to -15.7
< 0.001
160.3 ± 15.8
143.5±13.8
-16.8
-18.3 to -15.2
< 0.001
102.6 ± 5.9
92.3 ± 8.2
-10.3
-11.1 to -9.4
< 0.001
101.8 ± 5.6
90.4 ± 7.2
-11.4
-12.2 to -10.6
< 0.001
101.8 ± 5.6
89.3±17.1
-12.5
-13.3 to -11.8
< 0.001
SBP
Losartan monotherapy (A)
(n = 298)
Losartan plus HCTZ (B)
(n = 300)
Amlodipine monotherapy (C)
(n = 298)
DBP
Losartan monotherapy (D)
(n = 298)
Losartan plus HCTZ (E)
(n = 300)
Amlodipine monotherapy (F)
(n = 298)
Values are expressed as means±SD. HCTZ, hydrochlorothiazide. Between-group comparisons: A versus B, P<0.001; A versus C,
P=0.003; B versus C, NS; D versus E, P= 0.022; D versus F, P< 0.001; E versus F, NS.
Patients were examined during clinical visits during
weeks -4 (the start of the placebo run-in period), 0
(random allocation to treatment), 3, 6, 9 and 12. A
routine clinical examination was performed during all of
the visits. Blood chemistry determinations and urine
analyses were performed during weeks -4, 0, 6 and 12
(data not given). The blood pressure (the mean of two
recordings) and heart rate were recorded at trough
(i.e. 24 h after the latest morning dose). The blood
pressure was recorded after the subject had sat for at
least 5 min and after the patient had stood for 2 min.
Cuffs were of appropriate size and the blood pressure
was measured with the arm on which the measurement
took place supported at heart level.
Adverse events and drug tolerability were monitored
during all visits. The tolerability was evaluated by use of
a structured interview consisting of one general
question to be answered by 'yes' or 'no' ('Have you felt
any kind of discomfort since your last visit?') and 24
questions on specific symptoms to be answered in the
same way. The structured interview had previously
been evaluated [16). Moreover, during each visit the
number of adverse events considered drug-related ones
by the investigator was recorded, as was the number of
patients who had discontinued their participation in the
study because of adverse events.
During each visit, the global symptom score was
computed by giving a score equal to zero when a
symptom was absent and a score equal to unity when
a symptom was present and then summing the scores
obtained for each of the 24 symptoms. If a patient
did not answer three or more questions, the global
symptom score for that patient was set to 'missing'.
The PGWB index was used to evaluate changes in
quality of life [17,18]. The patients filled in this
questionnaire at home on the day before visits during
weeks -4, 0, 6 and 12 and brought the
questionnaire to the investigator in a sealed
envelope. The PGWB index comprises 22 questions
(range 22-132 points) divided into six domains
(anxiety, depressed mood, positive well-being, selfcontrol, general health and vitality). The PGWB
index has been used in several previous studies and,
in contrast to most other scales, includes both positive
and negative aspects. It is not intended to discriminate
between psychiatric cases and healthy subjects [13].
All of the patients had given their informed consent
to participate in the study and the study was approved
by research ethics committees of the University
Hospitals of Goteborg, Helsinki and Newcastle
(Australia).
Statistical analysis
To address the tolerability objective further, the area
under the curve (AUC0-12 weeks) was calculated for each
patient during the 12 week treatment period using the
trapezoidal method. The AUC0-12weeks measured was standardized for time of follow-up by dividing by the
number of days that the patient was monitored. It was
calculated as the area between the curve (change from
baseline in global symptom score versus time) and the
abscissa (time axis). The area below the abscissa (time
axis) was considered negative and the area above was
considered positive.
The efficacy and tolerability analyses were performed
using an intention-to-treat approach, including all
patients for whom we had efficacy and tolerability data
both at baseline and for during treatment; additional
analyses based on a per-protocol approach were also
performed but gave no further insight (data not given).
The comparability of the three treatment groups with
respect to patient characteristics was assessed by use of
the x2 test for the dichotomous variables and the
Kruskal-Wallis test for the ordered categorical variables.
Baseline efficacy variables (the global symptom score
and the blood pressure of seated subjects) were
analysed by analysis of variance
1330 Journal of Hypertension 1 997, Vol 1 5 No 11
including the treatment and investigators as factors.
Within-group tests of the change from baseline in blood
pressure, symptom score and effect on the quality of life
were based on a two-sided Student's t test. The betweengroup comparisons were performed in two steps. A closed
testing procedure of Bauer [19] was used to address-the
multiplicity issue.''When the overall treatment effect was
significant at the level P<0.05 according to analysis of
"arian.ce, three pairwise treatment comparisons were
performed on the basis of a least-squares analysis of the
means. The differences between treatment groups were
estimated in a pair-wise fashion in terms of the difference
in least squares and its associated 95% confidence interval
(CI).
Within-group changes in the incidence of patients
suffering any kind of discomfort (from- the general
questioning) and in the incidence of patients with each
symptom separately were assessed by the McNemar test.
Between-treatment comparisons were performed in two
Steps, as described above. Pairwise treatment comparisons
were carried out by means of a logarithmic-linear model.
The incidence of patients having drug-related adverse
experiences and patients discontinuing the study was
compared • between groups in a pairwise fashion using
Fisher's exact test. For the global symptom score, with a
sample size of 898 patients; the study had a 90% power
of detecting a between-treatment difference of 0.59 units
in the area under the curve, if such a difference existed.
Results
Blood pressure and heart rate
The blood pressure (of sitting patients) was lowered
significantly in members of all of the groups. After 6 weeks
(monotherapy) amlodipine treatment had reduced the
blood pressure by 13.8 ± 12.2/9.9 ± 6.4 mmHg (mean ±
SD) in comparison with 12.7 ± 12.1/8.5 ± 6.6 mmHg for
losartan treatment; in a pairwise comparison the difference between the groups was 0.9/1.3 mmHg (95% CI 0.7 to 2.6/0.4-2.2). After 6 weeks, 33% of the patients
in the losartan group and 40% of those being administered amlodipine had a diastolic blood pressure below
90 mmHg (P = 0.012).
The lowering of the blood pressure attained during week
12 is shown in Table 2. The results observed for the blood
pressure of standing patients were comparable to those
obtained for the blood pressure of seated patients (data
not given). After 6 weeks, 61% of the, patients in the
50 mg losartan group (group A) had been transferred to
the higher dose of 100 mg. The corresponding perce ages
in the 50 mg losartan and 12.5 mg HCTZ (group bj and
amlodipine (group C) groups were 62 and 56%, respectively (NS). Administration of 50 mg losartan (plus
12.5 mg HCTZ if necessary) and of 5 mg amlodipine
(or 10 mg if necessary) reduced the blood pressure equally
well. Administration of 50 mg losartan (or 100 mg if necessary), however, was not so effective as were the other two
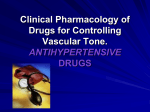
treatments (Table 2). This is also shown in Figure 1, in
which the percentages of patients who responded to treatment are given for the three treatment groups. The heart
rate did not change significantly for any group (data not
given). Subgroup analyses by country, sex, age group,
and degree of hypertension gave no further insight (data
not given).
Symptoms
After 12 weeks 'any discomfort' was reported by 33.1%
of the patients in the amlodipine group in comparison
with 23.3% at baseline (P = 0.002). The correspondin-
Fig. 1
Categories (l-lll) of response to antihypertensive treatment during week 12 for the diastolic blood pressures of seated patients. HCTZ,
hydrochlorothiazide; I, diastolic blood pressure <90 mmHg; II, diastolic blood pressure 90 mmHg and reduced by 10 mmHg; III, neither
I nor II.
Quality of life during losartan treatment Dahlöf et al.
1331
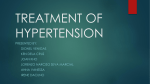
Fig. 2
Changes in incidence of individual symptoms and 95% confidence intervals during week 1 2 for (a) 50 or 100 mg losartan versus 5 or
10 mg amlodipine and (b) 50 mg losartan plus 12.5mg hydrochlorothiazide if necessary versus 5 or 10mg amlodipine.
percentages for losartan monotherapy were 22.5 and
23.2% (NS) and those for losartan plus HCTZ therapy
were 23.5 and 19.8% (NS). The symptom 'swollen
ankles' was reported by 30.6% of the patients in the
amlodipine group in comparison with 8.4% at baseline
(P < 0.001). The corresponding percentages for losartan
monotherapy were 7.0 and 7.0% (NS) and those for
losartan plus HCTZ therapy were 8.4% after treatment
and 10.0% at baseline (NS). The symptom 'swollen
ankles' was reported by 15.2% of the patients in the
amlodipine group already after 6 weeks, which was a
significant increase from baseline (P = 0.003).
'Dizziness upon standing' was more prevalent during
week 12 than it was at baseline among patients in both
losartan groups; 10.1 versus 6.0% for the losartan-alone
group. (P= 0.028) and 17.1 versus 9.0% for the losartan
plus HGTZ group (P = 0.001). The symptom 'dizziness
upon standing' was reported by 10.2% of patients in the
losartan group(s) as early as after 6 weeks, which was a
significant increase from baseline (P = 0.027). When
the 53 patients in the losartan group who reported
'dizziness upon standing' during week 12 were analysed
further we could not find any difference in lowering of
the blood pressure or in heart rate, with the patients
sitting and standing, compared with those of other
patients. We also considered age, sex and the
percentage increased doses, but this gave no further
insight (data not given). There was no increase in
prevalence of the symptom 'dizziness upon standing'
among patients in the amlodipine group during the
study.
In Figure 2(a) the changes in incidence of individual
symptoms and 95% CI during week 12 are given
for 50 or 100 mg losartan versus 5 or 10 mg amlodipine;
in Figure 2(b), the corresponding values are given for 50
mg losartan plus 12.5 mg hydrochlorothiazide if
necessary versus 5 or 10 mg amlodipine. A 'global
score' based on the 24 symptoms, integrating data from
all of the visits, revealed no differences between the
three treatment groups (Fig. 3). Finally, there were
more patients with drug-related adverse events in the
amlodipine group and more patients withdrew from
that group because of adverse events than occurred for
either of the losartan groups (Table 3).
Quality of life
The evaluation of the quality of life in terms of the
PGWB score revealed improvements for patients in the
losartan groups after 12 weeks in comparison with
baseline for
1332 Journal of Hypertension 1997, Vol 15 No 11
Fig. 3
Tables Patients whose Psychological General Well-Being Index
score improved, did not change and worsened in total score by
week 12 compared with baseline
Treatment groups
Losartan monotherapy (A) (n
= 298) Losartan plus HCTZ
(B) (n = 300) Amlodipine
monotherapy (C) (n = 298)
Improved (%)
60
No change
(%) Worsened (%)
8
6
33
6
54
39
50
44
HCTZ, hydrochlorothiazide. Between-group comparisons; A versus B, NS; A
versus C, P= 0.011; B versus C, NS.
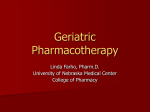
Fig. 4
Evaluation of tolerability in terms of the global symptom score
(0—24) and treatment group (mean changes from bassline): —
losartan monotherapy; - • -, losartan plus hydrochlorothiazide if
necessary; ..... , amlodipine monotherapy.
Table 3 Drug-related adverse experiences and patients
withdrawn from the study due to adverse experiences
A
B
C
Losartan
Completed the study (%)
Drug-related adverse experiences
(°/o)
Withdrawn due to adverse
experiencea (%)
monothera Losartan
plus HCTZ
py
(n = 300)
(n=300)
94
92
Amlodipine
monotberapy
(n = 298)
(n = 298)
89
22
24
3 6* * † † †
2
5
8*† †
HCTZ, hydrochlorothiazide. *P<0.06, **P = 0.01, versus B;
P= 0.001, versus A.
††
The total Psychological General Weil-Being (PGWB) index score
plotted for the visits (weeks -4, 0, 6 and 1 2) and treatment
groups: —-, losartan monotherapy (n = 267); ------ , losartan plus
hydrochlorothiazide it necessary; ..... , amlodipine monotherapy
(n = 259); only data for patients for whom we had a total score
value for each visit are shown.
P=0.01,
Table 4 Evaluation of quality of life with the Psychological
General Well-Being index (mean change from baseline by
week 12)
Domain
Anxiety
Depressed mood
Positive well-being
Self-control
General health
Vitality
Total score
A
Losartan
monotherapy
0.76
(P< 0.001)
0.25
(P= 0.042)
0.72
( P < 0 .0 0 1 )
0.14
(NS)
0.13
(NS)
0.47
(P = 0.01)
2.44
(P< 0.001)
B
Losartan plus
HCTZ
0.38
C
Amlodipine
monotherapy
0.33
(P= 0.044)
-0,04
(NS)
0.27
(NS)
0.04
(NS)
0.35
(P = 0.004)
0.42
(P= 0.035)
1.65
(P =0. 01 5)
(NS)
-0.09
(NS)
0,05
(NS)
0.14
(NS)
-0.20
(NS)
0.23
(NS)
0.5
(NS)
HCTZ, hydrochlorothiazide. Pair-wise between-group comparisons: for positive
well-being; overall between-group, P = 0.015; A versus B, P= 0.057; A
versus C, P = 0.005; B versus C, NS; and for general health, overall
between-group, P= 0.009; A versus B, NS; A versus C, P= 0.097; B versus
C, P= 0.002.
several domains (Table 4), whereas the quality of life
remained unchanged for all domains for patients in the
amlodipine group. The total score after 12 weeks was
110.0 versus 107.5 at baseline for the losartan monotherapy group (P< 0.001) and 109.8 versus 108.1 at baseline (P = 0.002) for the losartan plus HCTZ group. The
corresponding values for the amlodipine group were 108.7
and 108.2, respectively. The proportions of patients whose
total score improved, did not change, and worsened are
given in Table 5; for the three treatment groups, improvements were seen for 60, 54 and 50% of the patients,
respectively. The changes in total score during the study
(visits during weeks -4, 0, 6 and 12) are shown in Figure
4. Only data for patients for whom we had a total score
value for each visit were included. The data correspond
to 267 patients for losartan monotherapy, 261 for losartan
plus HCTZ if necessary and 259 for amlodipine
monotherapy; if data were missing for weeks 0 and 12,
data from weeks -4 and 6, respectively were carried
forwards. The slight improvement in total score from the
visit during week -4 to the visit during week 0 (during
placebo) was statistically significant (mean change 0.8,
P= 0.037).
Quality of life during losartan treatment Dahlöf et al.
After 6 weeks, the change in total score from
baseline was -0.14 (95% CI -1.07 to 0.79) for losartan
and 0.65 (-0.73 to 2.03) for amlpdipine; further
subgroup analyses have not been carried out. The Pvalue for the between-group comparison was 0.380.
Discussion
This study, which was intended to evaluate the differences among the effects of two losartan regimens (with
and without hydrochlorothiazide) and amlodipine
therapy in treating mild-to-moderate hypertension in
terms of their blood-pressure-lowering effects,
tolerability and effects on the quality of life, measured
in terms of PGWB, could be of interest for several
reasons. First, it was a -fairly large study comparing a
new drug, namely an angiotensin II antagonist, with a
well-tolerated, long-acting dihydropyridine, of
established properties. Smaller studies have shown
previously that losartan (with or without the addition
of hydrochlorothiazide) is tolerated better than and is as
effective as many other antihyper-tensive regimens [911,20-24]. Second, the vast majority of the patients was
recruited from primary health care and hence our
patients, were likely to have been representative of
hypertensives in the general population. Third, the
tolerability and quality of life were evaluated by using
several methods, namely spontaneous reporting, active
questioning and validated questionnaires. Fourth, and
maybe most importantly, patients who had previously
been treated with angiotensin II antagonists and calcium
antagonists were excluded from the study in order not
to bias any of the treatment groups.
Blood pressures measured at trough were reduced
equally well by administration of 5 mg amlodipine (or
10 mg if necessary) as they were by 50 mg losartan
(plus HCTZ if necessary) and better than they were
with losartan monotherapy. This was also evident
from the difference in the number of patients for
whom we attained the target diastolic blood pressure
of below 90 mmHg. In a previous smaller study, a
combination of 50 mg losartan and 12.5-25 mg HCTZ
had been found equally effective in lowering the blood
pressure as 5-10 mg amlodipine plus 12.5 mg HCTZ
[24]. On the other hand, losartan mono-therapy
compared favourably with the use of other dihydropyridines (nifedipine gastrointestinal therapeutic
system and felodipine extended release) regarding its
blood-pressure-lowering efficacy [9,25]. However,
amlodipine, possibly partly because of its long half life,
is somewhat more effective than is felodipine extended
release when the blood pressure is recorded 23-25 h
after administration of the dose [26J. That the addition
of 12.5 mg hydrochlorothiazide to 50 mg losartan
improved the blood pressure control was not at the
expense of reduced treatment tolerability and changes
in quality of life.
The usefulness of an antihypertensive medication
depends on the balance between efficacy and
tolerability,
1333
so the evaluation of a therapeutic regimen should
consist of valid measurements of both of these
variables. In the present study, among the patients
administered initially amlodipine, compared with
losartan-treated patients, there was a significantly
higher proportion of individuals answering 'yes' to the
question 'Have you felt any kind of discomfort since
the last visit?'. The difference between losartan and
amlodipine monotherapies was just below 10%, with a
wide confidence interval but separated from zero. A
similar pattern could be seen in the percentage of
patients who withdrew from the study due to adverse
effects; again significantly fewer patients withdrew
with losartan (2%) than did with amlodipine (8%).
When the patients were questioned actively regarding
specific symptoms, an expected increase in the
symptom of swollen ankles was reported with
amlodipine but not with losartan. The increased
incidence of swollen ankles with amlodipine was already
evident after 6 weeks (a 6.8% increase versus baseline),
that is, with the lower dose of the drug. The increase
was even more pronounced after 12 weeks (a 22.2%
increase versus baseline). Ankle oedema or swelling
of the ankles is a well-established side effect of calcium
antagonists [1,5,6] that is not seen with losartan; this has
previously been established (e.g. in comparisons with
nifedipine gastrointestinal system [25] and amlodipine
[24]). An unexpected increase in reporting of 'dizziness
upon standing' was evident among patients in both of
the losartan groups, with a tendency towards a higher
reported incidence among patients in the group who
also needed to be administered hydrochlorothiazide. We
have no valid explanation for this finding. Those
patients reporting 'dizziness upon, standing' did not have
any orthostatic fall in blood pressure or increase in
heart rate on standing.
Symptoms and side effects of antihypertensive
therapy can be multi-dimensional and influence the
patient's physical state, emotional well-being, sexual
and social functioning and cognitive functioning, and
thus affect his or her quality of life negatively.
Furthermore, this could have implications for
compliance and the patient's motivation to submit to
long-term therapy [12,27,28].
Measurements of the quality of life and well-being
are very important but have been a much neglected
area, mainly due to the lack of good, validated
measurement scales. Unfortunately, many studies have
been open or single-blinded ones with undocumented
methods, lacking control groups and concerning small
unselected populations. This study fulfils most of the
methodological requirements put forward for studies of
the quality of life (i.e. the trial was randomized, blinded
and had a parallel-group design with an adequate
sample size and a 12-week follow-up [13]). The
questionnaire used had been validated in many
previous studies and was developed to provide a
reproducible measure of subjective well-being
1334
Journal of Hypertension 1997, Vol 15 No 11
or distress. The PGWB instrument has been documented
extensively in terms of its reliability and validity [17,18].
The improvement in PGWB index before randomization,
when previous therapy was discontinued (Fig. 4), is interesting and probably reflects 'hidden' side effects of the
chronic therapy being administered before the study [29],
The general well-being, assessed in terms of the PGWB
index total score, at baseline was slightly higher than that
of the general population, indicating that we had an
asymptomatic hypertensive population; it was thus comparable to other studies of the quality of life [13]. During
the study, there was a significant improvement from
baseline in several domains with losartan (Table 4) but
nor with amlodipine. In the between-group analyses, only
two domains (positive well-being and general health)
exhibited significant differences, both in favour of losartan
treatment (Table 4). The proportion of patients whose
total score had improved by week 12 was 60% for the
group being administered losartan monotherapy and 50%
for those being administered amlodipine monotherapy (P
= 0.011, Table 5). The corresponding percentage for
patients in the group in which 62% of the patients had
been administered supplementary treatment with
hydrochlorothiazide from week 6 was 54% (NS).
Does this mean that a patient administered losartan in
this study actually felt better than 'normal'? That is not
our conclusion, but it is possible that the patients administered losartan felt better than did those administered
amlodipme. This could have been due to the fact that a
lowering of blood pressure equates to an improvement in
well-being, whereas more symptoms equates to a worsening in well-being. If this were true, the result of this
study would be that the balance in this regard is more
favourable for losartan treatment than it is for arniodipine
treatment.
One could argue that the sequence of treatment could
have influenced the quality of life and that the mere fact
of being in a study could have changed a patient's quality
of life for the better. We believe, however, that this could
not have favoured any of the groups in this randomized
study in which members of all groups were subjected to
the same procedures.
The absence of a change in PGWB index for amlodipinetreated patients is compatible with previous reports that
calcium antagonists have no positive or adverse effect on
the well-being and quality of life of patients [24,25,30-33].
Only high-dose nifedipine has affected well-being negatively and contributed to a high withdrawal rate due to
complaints of symptoms [16,34]. Furthermore, in another
study comparing amlodipine and captopril, the conclusion
drawn was that both drugs maintained the patient's
quality of life equally well [35].
Previously reported maximum interdrug differences in
general well-being score between therapies, assessed in
terms of the PGWB, have been of the order of 3 -4
between enalapril and atenolol [36], captopril and methyldopa [15], captopril and verapamil [29] and captopril and
propranolol [15]. Here, we observed a numerical difference (P.= 0.058) of 1.9 between losartan and amlodipine
monotherapies after 12 weeks.
In summary, after 12 weeks' treatment, 50 mg losartan
with 12.5 mg HCTZ added after 6 weeks (in 62% of cases)
was equally effective at lowering the blood pressure as
was 5 mg amlodipine increased to 10 mg (in 56% of cases).
Both of these regimens were superior to 50 mg losartan
increased to l00 mg (in 61% of cases). Both the losartan
and the amlodipine regimens were safe and tolerated we
but there were fewer adverse effects and withdrawals from
the study for the losartan groups than there were for the
amlodipine group. Moreover, losartan scored better in
some domains of PGWB than did amlodipine. The clinical significance of this observation, however, needs to be
studied further.
Acknowledgements
We would like to acknowledge the co-ordination efforts
of the monitors and especially Dr Hans Bostrom, Merck
Sharp & Dohme (Sweden). We would also like to express
our sincere thanks to Mrs Cecile Dubois, Brussels, for her
dedicated work with the statistical analyses. Moreover, we
would like to acknowledge the following investigators
who participated in the study:
in Australia Eddy Bajrovic (West Perth), Michael Beckoff
(Murray Bridge), Bruce Jackson (Preston), Anthony
Johnson (Brisbane), Jeffrey Karrasch (Kippa Ring), John
Kelly (Kogarah), Patrick Phillips (Adelaide), Craig Smee
(Dickson), Andrew Tonkin (Heidelberg), Anne Tonkin
(Adelaide), Judith Whitworth (Kogarah), Leigh Wilson
(Adelaide) and Roger Wyndham (Sydney), in Finland
Mikael Hedenborg (Helsinki), Antti Jounela (Oulu),
Leena Lahdenne (Helsinki), Urpo Laisi (Helsinki), Maini
Leinonen (Mantsala), Jarmo Lumme (Oulu),' Tapio
Ropponen (Helsinki), Raimo Siloaho (Pieksamaki), Jukka
Ulkuniemi (Kiiminki), Mauno Vanhala (Pieksamaki), and
in Sweden Jan Alvang (Trollhattan), Mats Andersson
(Vannas), Per Andren (Vaxjo), Jan-Axel Axelsson (Boras),
Anders Berglund (Borlange), Eva-Pia Darsbo (Ostersund),
Gunnar Ekblad (Lidkoping), Mark Flfast (Ytterby),
Ulla Eriksson (Upplands Vasby), Lars Froberg (Hoganas),
Peter Gadd (Norrahammar), Carin Hallendal (Han inge), Per Hauschildt (Skillingaryd),. Samy Hellerstedt
(Kallhall), Thomas Hermansson (Haninge), Ingalill
Hildebrand (Linkoping), Christer Hjortsberg (Helsingborg), Sofia Hollenberg (Upplands Vasby), Bernt
Johansson (Horndal), Anders Juhlin (Tyringe), AnnChristine Knutsson (Angelholm), Magnus Karegard
(Kristianstad), Inger Larsbrink (Vasterhaninge), Hakan
Quality of life during losartan treatment Dahlöf et al.
Larsson (Byske), Lars Larsson (Trollhättan), Åsa Larsson
(Trollhattan), Mikael Lilja (Husum), Lena Linden
(Tullinge), Anders Lindh (Åkersberga), Christina Lithner
(Krokom), Peter Nilsson (Dalby), Niels Norgaard
(Hoganas), Birgitta Strang-Olander (Malmö), Ivar LundOlseri (Snndviken), Birger Ossiansson (Vaxjö), Eva Pavek
(Knivsta). Karel Pavek (Uppsala), Lars Nygaard Pedersen
(Helsingborg), Mats Persson (Umea), Hillevi BlomPfeiffer (Upplands Väsby), Tom Roffey (Lidköping),
Bengt Silfverhielm (Ytterby), Anita Spjuth (Trollhättan),
Christina Storm (Sandviken), Dag Stromberg (Stockholm), Bo Sundqvist (Vannäs), Ulf Svensson (Lidkoping),
Peter Ten brock (Tumba), Bengt-Olov Tengmark (Kista),
Gunilla Vatnaland (Ängelholm), Niels Voergaard
(Solleftea), Per Wendell (Haninge), Mats Wernerson
(Norrköping), Lena Westerberg (Sandviken), Bo Westerdahl (Trollhattan), Kerstin Westergren (Sandviken), Evert
Zetterberg (Sandviken), Ingemar Zettergren (Sandviken),
Kristina Åresund (Sandviken) and Birgitta Örtelind
(Hisingsb'acka).
References
1
2
3
A
5
6
7
8
9
10
11
12
13
14
15
Hansson L, Svensson A, Dahlof B, Eggertsen R: Drug treatment of
hypertension. In Handbook of Hypertension. Edited by Robertson JIS.
Amsterdam: Elsevler; 1992, 15:655-708.
Collins R, Peto R, MacMahon S, Herbert P, Fiebach NH, Eberlein KA,
et al.: Blood pressure, stroke and coronary heart disease. Part 2,
short-term reductions in blood pressure: overview of randomised
drug trials in their epidemiological context. Lancet 1990, 335:
827-839.
MacMahcn S, Rodgers A: The effects of antihypertensive treatment on
vascular disease: reappraisal of the evidence in 1994. J Vase Med Biol
1993, 4:265-271.
Report of Medical Research Council Working Party on mild to moderate
hypertension: Adverse reactions to bendoflumethiazide .and propranolol
for the treatment of mild hypertension. Lancet 1981, ii:539-543.
Hansson L, Dahlof B. Treatment of hypertension with calcium
antagonists. In Clinical Aspects of Calcium Entry Blockers. Edited by van
Zwieten PA. Basel: Karger; 1989, 2:103-124..
Gustafsson D: Microvascular mechanisms involved in calcium
antagonist edema formation. J Cardiovasc Pharmacol 1987, 10
(suppl 0:3121-5131.
Karlberg BE: Cough and inhibition of the renin-angiotensin system.
J Hypertens 1993, 11 (suppl):S49-S52.
Fletcher AE, Palmer AJ, Bulpi't CJ: Cough with angiotensin converting
enzyme inhibitors: how much of a problem? J Hypertens 1994,
7:416-424.
Goldberg Al, Dunlay MC, Sweet CS: Safety and tolerability of losartan
potassium, an angiotensin II receptor antagonist, compared with
felodipine ER and angiotensin converting enzyme inhibitors for
the treatment of systemic hypertension. Am J Cardiol 1995, 75:
793-795.
Carr AA, Prisant LM: Losartan: first of a new class of angiotensin
antagonists for the management of hypertension. J din Pharmacol
1996, 36:3-12.
Goa KL. Wagstaff AJ: Losartan potassium: a review of its
pharmacology, clinical and tolerability in the management of
hypertension. Drugs 1996, 51:820-845.
Jones IK, Gorkin L, Lian JF, Staffa JA, Fletcher AP: Discontinuation of and
changes in treatment after start of new courses of antihypertensive
drugs: a study of a United Kingdom population. BMJ 1995,
311:293-295.
Hjemdal P, Wiklund IK: Quality of life on antihypertensive drug therapy:
scientific endpoint or marketing exercise? J Hypertens 1992,
10:1437-1446.
Wanda G, Grassi G: Considerations on current and future trials in
hypertension. Blood Pressure 1996, 5:327-332;
Croog SH, Levine S, Testa MA, Brown B, Bulpitt CJ, Jenkins D, et al.:
The effects of antihypertensive therapy on quality of life. N Engl J Med
1986 314:1657-1664.
1335
16 Os I, Bratland B, Dahlof B, Gisholt K, Syvertsen JO, Tretli S: Lisinopril or
nifedipine in essential hypertension? A Norwegian multicenter study
on efficacy, tolerability and quality of life in 828 patients. J Hypertens
1991, 9:1097-1104.
1 7 Dupuy HJ: Psychological General Weil-Being (PGWB) index:
assessment of quality of life in clinical trials of cardiovascular
therapies. Edited by Wenger NK, Mattson ME, Furberg CF, Elinson J.
New York: Le Jacq Publishing Inc.; 1984:170-183.
18 Wiklund I, Karlberg J: Evaluation of quality of life in clinical trials.
Selecting QoL measures. Contr din Trials 1991, 12
(suppl):S204-S216.
19 Bauer P: Multiple testing in clinical trials. Statist Med 1991,
10:871-890.
20 Weber MA, Neutel JM, Smith DGH: Controlling blood pressure
throughout the day: issue in testing a new antihypertensive agent.
J Hum Hypertens 1995, 9 (suppl 5):S29-S35.
21 MacKay JH, Arcuri KE, Goldberg Al, Snapinn SM, Sweet CS: Losartan
and low-dose hydrochlorothiazide in patients with essential
hypertension. Arch Intern Med 1996, 156:278-285,
22 Ruilope LM, Simpson RL, Toh J, Arcuri KE, Goldberg Al, Sweet CS:
Controlled trial of losartan given concomitantly with different doses of
hydrochlorothiazide in hypertensive patients. Blood Pressure 1996,
5:32-40.
23 Dahlof B, Keller SE, Makris L, Goldberg Al, Sweet CS, Lim NY: Efficacy
and tolerability of losartan potassium and atenolol in patients with
mild to moderate essential hypertension. Am J Hypertens 1995,
8:578-583.
24 Oparil S, Barr E, Elkins M, Liss C, Vrecenak A, Edeiman J: Efficacy,
tolerability and effects on quality of life of losartan, alone or with
hydrochlorothiazide versus amlodipine, alone or with
hydrochlorothiazide in patients with essential hypertension. Clin
Therapeutics 1996, 18:608-625.
25 Weir MR, Elkins M, Liss C, Vrecenak AJ, Barr E, Edeiman JM: Efficacy,
tolerability and quality of life of losartan alone or with
hydrochlorothiazide versus nifedipine GITS in patients with essential
hypertension. Clin Therapeutics 1996, 18:411-428.
26 Hoegholm A, Wiinberg N, Rasmussen E, Nielsen PE: Comparative effects
of amlodipine and felodipine ER on office and ambulatory blood
pressure in patients with mild to moderate hypertension. J Hum
Hypertens 1995, 9 (suppl 1):S25-S28.
27 Luscher TF, Vetter H, Sigenthaler W, Vetter W: Compliance in
hypertension: facts and concepts. J Hypertens 1935, 3 (suppl
1):S3-S9.
28 Perry HM Jr, Came! GH: Survival of treated hypertensive patients as a
function of compliance and control, J Hypertens 1984, 2 (suppl
3):S197-S199.
29 Dahlof B, Andren L, Eggertsen R, Jern S, Svensson A, Hansson L:
Potentiation of the antihypertensive effect of enalapril by randomised
addition of different doses of hydrochlorothiazide. J Hypertens 1985,
3 (suppl 3):S483-S486.
30 Croog SH, Kong BW, Levine S, Weir MR, Baume RM, Saunders £:
Hypertensive black men and women. Quality of life and effects of
antihypertensive medications. Arch Intern Med 1990, 150:1733-1741.
31 Fletchei AE, Chester PC, Hawkins CM, Latham AN, Pike LA, Bulpitt CJ:
The effects of verapamil and propranolol on quality of life in
hypertension. J Hum Hypertens 1989, 3:125-130.
32 Zachariah PK, Brobyn R, Kann J, Levy B, Margolis R,; McMahon FG,
et al.: Comparison of quality of life on nitrendipine and propranolol. J
Cardiovasc Pharmacol 1988, 12 (suppl 4):S29-S35.
33 Fletcher AE, Bulpitt CJ, Chase DM, Collins WC, Furberg CD, Goggin TK,
et al.: Quality of life with three antihypertensive treatments. Cilazapril,
atenolol, nitrendipine. Hypertension 1992, 19:499-507,
34 Testa MA, Hollenberg NK, Anderson RB, Williams GH: Assessment of
quality of life by patient and spouse during antihypertensive therapy
with atenolol and nifedipine gastrointestinal therapeutic system.
Am J Hypertens 1991, 4:363-373.
35 Omvik P, Thaulow E, Herland OB, Eide I, Midha R, Tuner RR: Doubleblind parallel, comparative study on quality of life during treatment
with amlodipine or enalapril in mild or moderate hypertensive patients:
a multicentre study. J Hypertens 1993, 11:103-113.
33 Applegate WB, Phillips HL, Schnaper H, Sheperd AMM, Schocken D, Luhr
JC, et al.: A randomised controlled trial of the effects of three
antihypertensive agents on blood pressure control and quality of life in
older women. Arch Intern Med 1991, 151:1817-1823.