Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
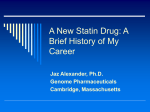
Return to October 2001 Table of Contents REVIEW ARTICLE Statin myopathies: pathophysiologic and clinical perspectives Steven K. Baker, MSc, MD Mark A. Tarnopolsky, MD, PhD From the Department of Medicine, Division of Neurology and Rehabilitation, McMaster University Medical Centre, McMaster University, Hamilton, Ont. Medical subject headings: anticholesteremic agents; arteriosclerosis; coenzymes; hydroxymethyl-CoA reductase inhibitors; hypercholesterolemia; lipids and antilipemic agents; lovastatin; muscular disease; pravastatin; rhabdomyolysis; simvastatin; ubiquinone (Original manuscript submitted Aug. 21, 2001; received in revised form Aug. 23, 2001; accepted Aug. 28, 2001.) Clin Invest Med 2001;24(5):258-72. © 2001 Canadian Medical Association Introduction The sequelae of atherosclerotic vascular disease contribute significantly to the burden of illness in developed nations. In Canada an estimated 36% of all deaths result from cardiovascular disease (CVD).1 Antilipemic agents have proven to be particularly advantageous in both primary and secondary prevention of CVD sequelae.2–4 Among the various lipid-lowering medications the 3-hydroxy-3methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors, (HMGRI or “statins”) have emerged as the dominant class for the treatment of hypercholesterolemia.5 In addition to their ability to lower serum cholesterol by inhibiting a rate-limiting enzyme in the cholesterol biosynthetic pathway, statins have also been shown to target a variety of cellular processes that modify endothelial function, inflammatory responses, plaque stabilization and thrombogenesis.6,7 Relevant to these functions are the findings that acute statin therapy decreases the incidence of symptomatic ischemia in patients with acute coronary syndromes8 and may suppress recurrent transient ischemic attacks.9 These newly discovered properties make statins particularly attractive agents for the acute and long-term treatment of CVD be258 cause they target multiple pathways that ultimately converge in atherothrombotic events. The use of statins in the treatment of lipid-related disorders is therefore expected to rise. Generally, the statins have a benign side-effect profile and are well tolerated. The most serious adverse effects arise from cell damage in liver and skeletal muscle. Increases in serum transaminases of hepatic origin are dose dependent and occur with a reported frequency of approximately 1%, whereas myotoxicity, defined as myalgias and elevated serum creatine kinase values (>10 times the upper limit of normal), occurs in 0.1% of patients.5 Although hepatotoxicity is more common, myotoxicity may pose a larger risk for sarcolemmal disruption (i.e., rhabdomyolysis) and can lead to myoglobinuria and acute renal failure.10–13 The incidence of myopathies is low, but the increasing use of statins implies that more physicians will encounter this clinical entity. Attempting to understand the pathophysiology of statins is of particular importance given the withdrawal of cerivastatin from the market in August 2001 owing to an unacceptable incidence of rhabdomyolysis and death. This review will consider the potential etiologies of statin myopathies in relation to altered cholesterol biosynthesis and muscle physiology. Clin Invest Med • Vol 24, no 5, octobre 2001 Statin myopathies Pathophysiologic considerations HMG-CoA reductase and statin biochemistry Unique among lipid-lowering drugs, statins impair cholesterogenesis by selectively targeting the ratelimiting enzyme, HMG-CoA reductase by reversible competitive inhibition. This enzyme catalyzes the conversion of HMG-CoA to mevalonate, an intermediate, which in turn gives rise to numerous metabolites (Fig. 1). Pharmacologic inhibition of HMG- Acetate Acetyl-CoA CoA reductase results in reduced cholesterol synthesis and transcriptional upregulation of HMG-CoA reductase (i.e., impaired feedback inhibition) and may increase the expression of hepatic low-density lipoprotein (LDL) receptors.14 This increases the fractional catabolic rate of plasma LDL and therefore lowers serum cholesterol.14 Hormonal control of HMG-CoA reductase is exerted by 4 agents: (1) glucagon, which opposes insulin’s transcriptional effect and phosphorylates the enzyme thereby reducing its activity; (2) thyroid Acetoacetyl-CoA HMG-CoA Statins Mevalonate-5-PP CoQ10 Isopentyl-PP Mevalonate-5-P Prenylated proteins Geranylgeranyl-PP Geranyl-PP Mevalonate Farnesyl-PP Squalene Dolichols Cholestadien-3β-ol *2 *3 Lathosterol Desmosterol Lanosterol Squalene-2,3-epoxide 7-Dehydrocholesterol Cholesterol Fig. 1: The biosynthetic pathways for mevalonate and its distal metabolites. Statin drugs selectively impair the rate-limiting enzyme, β-hydoxy-β-methylglutaryl-coenzyme A reductase, which decreases cholesterol production. Farnesyl-pyrophosphate (PP) gives rise to geranylgeranyl-PP, the compound responsible for donating 10 isoprenoid tail units to coenzyme Q (CoQ10). There are 3 nonenzymatic steps (*3) between lanosterol and cholestadien-3β-ol and 2 steps (*2) between this molecule and desmosterol. Overall, 14 steps (enzymatic + nonenzymatic) separate mevalonate from cholesterol, whether it is formed from desmosterol or 7-dehydrocholesterol. This lack of propinquity to the targeted substrate causes pleiotropic metabolic effects in skeletal myocytes. Clin Invest Med • Vol 24, no 5, October 2001 259 Baker and Tarnopolsky hormone, which increases enzyme activity through enhanced transcription and mRNA stability; (3) glucocorticoids, which destabilize; and (4) estrogen, which stabilizes HMG-CoA reductase mRNA.15 Interestingly, hypothyroidism has been hypothesized to potentiate the myotoxic effects of statins.16–18 Although there have been no reports on myopathic interactions between glucocorticoids and statins, steroids may possibly contribute to muscle damage in organ transplant recipients receiving combination immunosuppresive and lipid-lowering therapy.19,20 Five drugs — atorvastatin, fluvastatin, lovastatin, pravastatin and simvastatin — are currently marketed in North America; a sixth, cerivastatin, has recently been withdrawn. Lovastatin, pravastatin and simvastatin are all fungal derivatives and share the same hydronaphthalene ring structure. Simvastatin is a semisynthetic methylated analogue of lovastatin. Pravastatin is a purified metabolite of mevastatin, the original HMG-CoA reductase inhibitor that was never marketed.21–25 Atorvastatin, cervistatin and fluvastatin are synthetic.26 Each statin molecule has a moiety resembling hydroxymethylglutaric acid. The open, hydroxy acid, conformation is active whereas the closed, lactone, conformation is inactive. Hepatic hydrolysis at alkaline pH decyclizes and hence activates the lactone prodrugs lovastatin, atorvastatin and simvastatin.27 Extensive first-pass metabolism limits the systemic bioavailability of the HMGRIs and accounts for the rapid clearance of statins, excepting atorvastatin.2 (Atorvastatin undergoes hepatic metabolism to active metabolites, which, together with the parent compound, have a half-life of about 15 hours.) The hepatic microsomal cytochrome P450 isoenzyme system (CYP) is responsible for the complex metabolism of the HMGRIs. After hydrolysis, the lactone prodrugs lovastatin,28 and simvastatin,28 cerivastatin,29 and atorvastatin 30 are primarily oxidized by CYP3A4. Fluvastatin is predominately (50%–80%) inactivated by CYP2C9, but recent evidence suggests that CYP3A4 and CYP2C8 also contribute to its biotransformation.31 Cerivastatin is also partially oxidized by CYP2C8.29 The multiple CYP isoenzyme pathways open to both cervistatin and fluvastatin may afford increased protection against potential myotoxic interactions when coadministered drugs compete with or antagonize CYP isozymes.32 260 Cholesterol biosynthesis and the isoprenoids The inhibition of HMG-CoA reductase by the HMGRIs is approximately 14 steps and 9 to 10 enzymatic reactions removed from the terminal step(s) in cholesterologenesis (mediated by 7-dehydrocholesterol reductase and desmosterol reductase). Furthermore, mevalonic acid, the immediate product of HMG-CoA reductase, is a pivotal precursor intermediate which gives rise to the vital isoprenoids en route to cholesterol. It is not surprising, therefore, that inhibiting this important biosynthetic pathway causes pleiotropic metabolic consequences33,34 (Fig. 1). Prenylation is a fundamental element of posttranscriptional lipid modification of proteins and other compounds and affects their function. Some of the known isoprenoids include the following: (1) isopentyladenosine, required for transfer RNA synthesis; (2) dolichols, required for glycoprotein synthesis; (3) heme A, a polyisoprenoid component of the electron transport chain; and (4) ubiquinone, a polyisoprenylated quinoid cofactor of the electron transport chain, which accepts electrons from complexes I and II.6,35,36 The predominant form of coenzyme Q in human is coenzyme Q10, containing 10 isoprenoid units in the tail, whereas the predominant form in rodents is coenzyme Q9, with 9 isoprenoid units in the tail. The covalent addition of either farnesyl (15-carbon) or geranylgeranyl (20-carbon) isoprenoids to conserved cysteine residues on the C-terminus of important regulatory proteins enables both membrane association and protein–protein interactions.37 It is estimated that over 1% of mammalian cellular proteins are isoprenylated.38 Isoprenylated proteins have been implicated in smooth muscle cell migration and proliferation,33 and skeletal muscle cell growth and differentiation.39–42 These conclusions were borne out of experiments in which statin treatment impaired cell development in culture, whereas the coapplication of mevalonate or its distal metabolites (i.e., farnesol or geranylgeraniol) reversed many of the inhibitory cellular effects of statins.41,43 The identification of prenylated proteins involved in signal transduction and cell cycle progression (i.e., laminin B, ras proto-oncogene, Rho-related proteins and the γ-subunit of heterotrimeric GTPbinding proteins) supports the dependency of these processes on the mevalonate pathway. Clin Invest Med • Vol 24, no 5, octobre 2001 Statin myopathies Statins and altered muscle physiology Spectrum of myotoxic reactions to statin drugs Various hypotheses have been proposed to explain the relationship between statin therapy and the spectrum of muscle dysfunction manifested by myalgia, myopathy and rhabdomyolysis. Although each demonstrates unique merits none has sufficiently elucidated the underlying pathophysiology, which remains speculative.39,42,44–46 Myalgias are clinically defined by any combination of muscle weakness, tenderness or pain either in a proximal or regional pattern. Clinically, patients often describe a cramping feeling in the muscle. The serum creatine kinase (CK) activity can be normal or only trivially elevated. In addition to myalgic complaints, patients with HMGRI-related myopathy may have CK activity values more than 10 times the upper limit of normal for a given reference laboratory (i.e., >2200 U/L for males and >1500 U/L for females).47 Light and electron microscopic histomorphometric features of statin-induced myopathy are listed in Table 1.48 Altered myofibre architecture with evidence of necrosis has been observed in experimental rodent models of statin myopathy, where exposure to suprapharmacologic doses accelerates myotoxicity,48,49 and in humans exposed to therapeutic doses.50–52 Rhabdomyolysis, an acute degeneration of skeletal muscle, is a potentially fatal condition due to the toxic effects of myoglobinemia/myoglobinuria on the renal tubules. Nephrotoxicity is largely mediated by the Fenton (Fe2+ + H2O2 → Fe3+ + OH• + OH–) and Haber–Weiss (O2•– + H2O2 → O2 + OH• + OH–) reactions as myoglobin provides ferrous iron, which serves as a catalyst for the generation of harmful reactive oxygen species. Interestingly, reactive oxygen species have also recently been implicated in the pathophysiology of contrast-agent-induced renal dysfunction,53–55 a condition in which N-acetylcysteine pre-supplementation (600 mg × 2 d) was shown to be nephroprotective.56 Whether the acute administration of antioxidants, at the onset of rhabdomyolysis, favourably alters the expression of renal damage is unknown but deserves investigation. Serum CK activity values are greatly elevated but cannot be used to differentiate rhabdomyolysis from Clin Invest Med • Vol 24, no 5, October 2001 myopathy. Possible complications arising from rhabdomyolysis and consequent acute tubular necrosis include hypocalcemia, hyperkalemia, metabolic acidosis, hyperuricemia, disseminated intravascular coagulation, cardiomyopathy and respiratory embarrassment.56 Ubiquinone and the development of statin myopathy Much interest has focused on the role of ubiquinone in the development of statin myopathy.57–63 This potential etiology has biologic rationale as coenzyme Q10 is an essential cofactor of the electron transport chain.56 Coenzyme Q10 is a lipophilic compound composed of redox active quinoid moieties as well Table 1: Histomorphologic changes in mammalian skeletal muscle after pharmacologic doses of statins (lovastatin, 1 mg/g body weight for 30 days). Microscopy Change Light Increased variability in fibre diameter Myofibre splitting Increased numbers of internal nuclei Perimysial fibrosis Coarsening of intermyofibrillar membranous network Clumping of intermyofibrillar membranous material Diffuse decrease in NADH dehydrogenasestaining in non-necrotic myofibres Myofibre necrosis with macrophage invasion Hypercontracted fibres Relative sparing of slow-twitch oxidative fibres with earlier involvement of fast-twitch glycolytic fibres Electron 2 types of mitochondrial alterations: • fragmented inner mitochondrial membrane (IMM) or absent or effaced mitochondrial cristae ± replacement of cristae with fine granular material; outer mitochondrial membrane (OMM) intact • spared IMM and matrix; redundant and thickened OMM ± circular loops formed by OMM material Myeloid figures in degenerating mitochondrial membranes Dilated cisterns of the sarcoplasmic reticulum normal transverse tubules Increased presence of vacuoles Intermyofibrillar and subsarcolemmal accumulations of abnormal mitochondria Small zones of Z-band streaming Adapted from Waclawik AJ, Lindal S, Engel AG. Experimental lovastatin myopathy. J Neuropathol Exp Neurol 1993;52:542-9. Biopsies were taken from Lewis rat gastrocnemius muscles on days 5, 10, 12, 14 and 30. Therefore, selected features from the above list were not observed in each animal. Longer treatment was associated with worsening disease. 261 Baker and Tarnopolsky as a hydrophobic prenylated tail that provides the physiochemical properties enabling mobility within the phospholipid bilayer of the inner mitochondrial membrane. Coenzyme Q10 is found in complexes I and II of the electron transport chain (ETC) where it undergoes 2 sequential 1 electron reductions by flavoproteins, first to the semiubiquinone radical and then to ubiquinol. 6,35,36 Ubiquinol reduces cytochromes b and c of complex III and so provides the necessary electron carrier system for reduced nicotinamide adenosine dinucleotide (NADH)- and reduced flavin adenosine dinucleotide (FADH2)linked substrates to aerobically generate ATP, the universal cellular energy currency. Coenzyme Q10 also serves as an important antioxidant in both mitochondria and lipid membranes.64,65 Apoptosis, which can be induced by statins in cultured myoblasts66,67 is inhibited by coenzyme Q10.68 Additionally, coenzyme Q10 decreases oxidative DNA damage in human lymphocytes.56 Further evidence of the potential utility of coenzyme Q10 for the treatment of statin myopathy derives from studies demonstrating both biochemical and clinical efficacy of quinone supplementation in patients with primary69–72 and secondary (i.e., cardiomyopathy)56,73–75 coenzyme Q10 deficiency states and other forms of mitochondrial disorders.76 Given the preponderance of evidence supporting the therapeutic efficacy of coenzyme Q10 in various conditions, the question is not whether coenzyme Q10 supplementation benefits patients who are ubiquinone-deficient, but whether statin therapy induces such a secondary deficiency state. Shortly after the development of selective inhibitors of HMG-CoA reductase experimental evidence accrued demonstrating impaired ubiquinone synthesis in various cell types.77,78 Clinical reports describing the efficacy of coenzyme Q10 supplementation in patients with statin myopathy soon followed.79,80 The first case described a physically active 48-year-old physician who experienced fatigue and proximal myalgias and had elevated CK levels (1400 U/L) 2 to 3 weeks after starting lovastatin (20 mg OD). Despite withdrawal of the drug, his symptoms persisted for 6 months, at which time he began taking low-dose coenzyme Q10 (30 mg OD). Within a few days his symptoms abated, and he resumed strenuous activities without difficulty.80 The 262 second case report described a 63-year-old woman who required hospital admission 8-months after starting simvastatin (20 mg OD) for a constellation of symptoms and laboratory abnormalities that resembled a MELAS (mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes) syndrome. Her clinical findings included diffuse muscle weakness, bilateral ptosis, external ophthalmoplegia, cognitive dysfunction and mild aphasia. Laboratory investigations revealed rhabdomyolysis (CK >20 000 U/L), hyperlacticacidemia (5.1 mmol/L; normal <2.2 mmol/L) and ragged-red fibres with abundant pleiomorphic mitochondria and a reduced muscle coenzyme Q10 concentration ([Q10]) (13.1 mg/g; normal 15.5–21.7 mg/g)81–83 on skeletal muscle biopsy. A 3-month trial of oral coenzyme Q10 (250 mg OD) ameliorated weakness and ophthalmoplegia, renormalized muscle [Q10] and eliminated ragged-red fibres.79 Interestingly, consecutive etofibrate and clofibrate treatment provoked a mitochondrial myopathy5 and valproate, an antiepileptic agent that inhibits mitochondrial fatty acid oxidation, reportedly triggered a MELAS syndrome in a woman who was later found to harbour the A3243G transition mutation.84 Although this 63year-old did not have the A-to-G substitution at nucleotide 3243 it is quite conceivable that she harboured another defect since none of the other mutations (>50) were sought. These observations raise the possibility that pharmacologic inhibitors of mitochondrial metabolism may unmask latent mitochondrial dysfunction and manifest overt disease. Coenzyme Q10 improved the lactate/pyruvate (L/P) ratios in some patients with mitochondrial myopathies and increased oxygen consumption in a patient with MELAS.76,85,86 Related to this, De Pinieux and colleagues,57 found increments in the L/P ratios of patients treated with statins compared to hyperand normocholesterolemic controls (19.0 v. 15.9 and 13.1, respectively). The statin group was not supplemented with coenzyme Q10 to determine if blood lactate levels could be restored to normal. The high lactate levels were presumed to be secondary to a statin-induced alteration of ubiquinone biosynthesis and thus (ETC) function. Significantly, serum ubiquinone was lower in the statin group than the hypercholesterolemic controls but unchanged comClin Invest Med • Vol 24, no 5, octobre 2001 Statin myopathies pared to the healthy controls (0.75 v. 0.69 mg/L) who had normal L/P ratios. The etiologic importance of ubiquinone was therefore questionable. Numerous investigations have confirmed that statins reduce serum ubiquinone concentrations.57,60,62,87–89 Circulating lipoproteins appear to be the predominant carrier proteins for ubiquinone in both animals90 and humans.91,92 Laaksonen and associates 88 found reductions in serum and LDL ubiquinone approximately proportional to reductions in serum LDL cholesterol after 4 weeks of statin treatment. In contrast, another study found that whereas short-term (4-wk) statin treatment did not change serum ubiquinone-to-LDL ratios, long-term treatment (12 wk) caused a significant decrement in serum LDL (–25%) relative to serum coenzyme Q10 (–52%). Whether long-term statin treatment increases the likelihood of secondary ubiquinone deficiency is not entirely clear, but this seems unlikely as a subsequent study found no differences in serum ubiquinone-to-LDL ratios after 6 months of simvastatin therapy (i.e., 0.49 before v. 0.50 after).87 In fact, one study reported an elevated serum ubiquinone-toLDL ratio after HMGRI treatment.56 Of greater theoretical importance is the effect of statins on intramuscular coenzyme Q10 content for biosynthetic alterations in this tissue should provide a more precise index of deranged metabolism. Only one study has found depleted muscle ubiquinone, which appeared to be commensurate with the extent of muscle damage.79 Paradoxically, in the few muscle biopsy studies performed to date, ubiquinone concentrations were increased after HMGRI treatment in rodents 56 and humans. 87,88 These results suggest that HMGRIs do not cause physiologically significant perturbations in muscle coenzyme Q10 synthesis. However, none of the patients in whom muscle biopsies were performed experienced any symptoms of myotoxicity. It is tempting to speculate that only those patients who express a latent mitochondriopathic diathesis or partial defect in coenzyme Q10 synthesis will become clinically symptomatic with the administration of statin drugs. This notion is supported by the finding that lovastatin while impairing the incorporation of [3H]acetate and [14C]tyrosine into ubiquinone failed to impair the activities of succinate-cytochrome c reductase and Clin Invest Med • Vol 24, no 5, October 2001 succinate dehydrogenase in murine neuroblastoma cells. Additionally, polarographic measurements of oxygen consumption in state 3 (i.e., electron transport chain saturation) and in an uncoupled state in both muscle homogenate and isolated mitochondria were normal.93 Therefore, even in the context of quantified decreases in ubiquinone synthesis mitochondrial respiration was preserved. However, this was an acute treatment effect in vitro and may not parallel chronic in vivo changes. Laaksonen and colleagues87 confirmed this with measurements of highenergy phosphates in skeletal muscle. Both ATP and creatine phosphate levels were unaffected by therapeutic doses of simvastatin. Recently, simvastatin treatment was associated with a reduction in blood ATP levels even though tissue ATP concentration ([ATP]) 7was not affected.94 Considering that muscle, by virtue of its mass and metabolic activity, is a major contributor to the blood ATP pool it is unclear what causes the fall in [ATP]. One possibility may be that statins cause membrane destabilization resulting in functional impairment of the ATP binding cassettes (i.e., ATP transport proteins) and decreased egression of ATP. Therefore, constrained ATP synthesis coupled with decreased membrane ATP transport may account for reduced blood [ATP] with paradoxically normal tissue [ATP]. This requires experimental confirmation. Ubiquinone is an important antioxidant in biological systems. 6,95 Statins reduce concentrations of lipophilic antioxidants (i.e., α-tocopherol, β-carotene and lycopene) found in LDL particles.87 As with coenzyme Q10, this effect is thought to be mediated by a primary drop in serum lipoproteins.56 Lankin and associates96 found that pravastatin intensified in vivo free radical oxidation of LDL particles in patients with myocardial ischemia and that ubiquinone supplementation suppressed lipid peroxidation. Ischemia is a potent generator of free radicals 97,98 and ubiquinone has been well described as an antiischemic cardioprotectant;99–103 therefore it is unclear to what extent exogenous coenzyme Q10 attenuated ischemia- or statin-related oxidative stress. The contribution of ubiquinone to the development of statin myopathy is unclear. This is because definitive experiments correlating mitochondrial respiratory chain enzymology to muscle coenzyme [Q10] 263 Baker and Tarnopolsky and indices of oxidative stress (i.e., malondialdehyde, 8-iso-prostaglandinF 2α , 8-hydroxy-2′deoxyguanosine) in patients with and without statin myopathy is lacking. Effects of statins on membrane function and calcium regulation Statins have been reported to affect skeletal muscle K+ ¯ Cl PIP Na + Ca 2+ ↑Na+ PLCγ1 P membrane physiology not only through changes in cholesterol content,94 which alters membrane fluidity,2 but also through changes in (1) membrane electrical properties (which appears to be a secondary phenomenon),2,104,105 (2) Na+-K+ pump density,106 (3) excitationcontraction coupling,107 and (4) cell surface receptor signal transduction cascades.66,108 Fig. 2 provides a composite summary of the hypothetical multifactorial etiopathogenesis of statin-induced myotoxicity. ↓ GCl– DAG + IP3 ↑[Ca ]i 2+ Ca2+ Ca2+ Ca2+ Transverse tubule ↓ Q10 → ? ↓ ATP → E dysFx → ROS Ca ? ↑ O2•– 2+ SR ↓ Chol/PL ratio Sarcomere Fig. 2: A comprehensive schematic diagram of the proposed mechanisms of statin myopathy. Decreased chloride conductance (GCl–) potentially destabilizes membrane electrical potential and increases susceptibility to myotonic afterdepolarizations, which may elevate intracellular calcium ([Ca2+]i) through increased sarcoplasmic reticulum (SR) Ca2+ release. Furthermore, [Ca2+]i may be augmented from increased activity of the Na+Ca2+ exchanger as a secondary response to increased intracellular [Na+], which accrues as a result of decreased Na+-K+ pump density. SR Ca2+ ATPase function may be impaired by statins therefore impairing the reuptake of free sarcoplasmic Ca2+. Statins induce the phosphorylation (P) of the γ1 subunit of phospholipase C (PLCγ1) causing phosphodiesterase activation and the conversion of phosphatidylinositol 4,5-bisphosphate (PIP) to diacylglycerol (DAG) and inositol 1,4,5-trisphosphate (IP3). Receptors on the SR for IP3 mediate Ca2+ release (Note, the IP3 receptors predominate in the junctional SR but are depicted in the longitudinal SR for clarity). Decrements in the membrane cholesterol-to-phospholipid (Chol/PL) ratio may also contribute to disruption of integral membrane protein function. Decreased synthesis of ubiquinone (Q10) may lead to both decreased ATP production and reduced free radical scavenging. E dysFx = energy dysfunction, ROS = reactive oxygen species. 264 Clin Invest Med • Vol 24, no 5, octobre 2001 Statin myopathies Cholesterol’s role in membrane chloride conductance was first evidenced in patients treated with clofibrate who presented with acute muscular syndromes characterized by muscle cramping, weakness, stiffness and myopathic changes.109,110 Clofibrate produces electrophysiologic myotonia in rats, an effect completely attributable to a drug-induced decline in membrane chloride conductance.56 In experiments by Pierno and colleagues104,105 pravastatin was shown to have no effect on electromyographic activity or membrane chloride conductance whereas simvastatin caused dose-dependent reductions in the latter. Furthermore, decreased action potential amplitudes were recorded in simvastatin-treated rats, suggestive of decreased sodium channel function, and glybenclamide attenuated the increased potassium channel conductance, suggestive of reduced flux through the ATP-sensitive K+ channel. The latter finding was hypothesized to be attributable to decreased muscle ubiquinone and ATP, leading to channel opening; however, as discussed above, this remains inconclusive. Sarcolemmal Na+–K+ ATPase activity is partly determined by the cholesterol environment in which it is expressed.111,112 Reductions in membrane cholesterol impair pump function whereas elevated cholesterol levels augment pump function.113 Lovastatin, through mechanisms unrelated to changes in membrane cholesterol, decreased sarcolemmal Na+–K+ ATPase density and pump current in skeletal and cardiac muscle.106 This was accompanied by a coordinated rise in sarcoplasmic Na+ concentration. Parenteral administration of mevalonate reversed these effects. Although unsubstantiated, increased intracellular Na+ could invoke Ca2+ influx via the Na+–Ca2+ antiport and cause myofibre necrosis or apoptosis.56 Excitation-contraction coupling is the process by which a sarcolemmal action potential is propagated down the transverse tubules and converted into a calcium release signal through the interaction between L-type calcium channel dihydropyridine receptors and sarcoplasmic reticulum (SR) ryanodine receptors at the triadic junctions.4 A second messanger signal from inositol 1,4,5-trisphosphate (IP3) is also involved in modulating SR Ca2+ release in skeletal muscle.114,115 Simvastatin significantly reduced the mechanical threshold of rat skeletal muscle in a Clin Invest Med • Vol 24, no 5, October 2001 dose-dependent fashion.99 The voltage threshold for contraction is made more negative (closer to the resting potential) by any process, either physiologic or pharmacologic, that increases cytosolic Ca2+ concentration ([Ca2+]).56 Either increased SR Ca2+ release or decreased SR Ca2+ATPase (SERCA) activity can be responsible for elevated cytosolic [Ca2+]. High concentrations of simvastatin in rat L6 myoblasts caused transient elevations in cytosolic [Ca2+] and eventual membranolysis.56 Parallel findings were recorded in cultured rat skeletal muscle satellite cells superfused with simvastatin.116 In this study, neither mevalonic acid nor cholesterol could abolish simvastatin’s effect, and membrane lipid composition was unchanged, suggesting that the effect was not mediated through an inhibition of HMG-CoA reductase. Simvastatin caused similar increases in intracellular [Ca2+] in cardiomyocytes.84 Recently, tyrosine phosphorylation of the γ1 subunit of phospholipase C (PLC) has been inculpated as a critical step in cell death signalling in L6 myoblasts.108 Tyrosine phosphorylation of PLC-γ1 stimulates catalytic activity, causing coordinated increments in IP3 and intracellular [Ca2+]. Interestingly, aging is associated with decreased SERCA activity.117,118 Aging is also coupled to the accumulation of mitochondrial DNA mutations, leading to impaired ETC function and the generation of reactive oxygen and nitrogen species.119 The SERCA2 isoform appears to be relatively resistant to oxidative damage,2,56 whereas the fast-twitch isoform, SERCA1, is particularly vulnerable to oxidative modification at targeted cysteine residues.56 If statins do increase the oxidative burden in skeletal muscle, the SERCA1 protein may be susceptible and thus contribute to the deranged Ca2+ homeostasis. Whether oxidative factors are related to the statinmediated early and selective mitochondrial swelling and fibre necrosis commonly observed in type II fibres (i.e., fast-twitch fibres)48,56 is not known. Drug interactions and 3-hydroxy-3-methylglutaryl CoA-reductase inhibitor therapy The concomitant administration of HMGRIs with other medications poses a significant risk for the development of myotoxicity. As already discussed, CYP3A4 is the predominant isoform responsible for 265 Baker and Tarnopolsky HMGRI biotransformation. Current evidence suggests that the muscle damage is precipitated through inhibition of CYP3A4 with secondary elevations in serum HMGRI levels. 81,120–122 For example, erythromycin,121,122 azole antifungals,4,56 cyclosporin A (CsA),56 mibefradil2 and nefazadone3 are all oxidized by CYP3A4 and have been associated with myopathy or rhabdomyolysis when taken with lipophilic HMGRIs (Table 2). Indeed, the pharmacokinetics of pravastatin, a hydrophilic HMGRI with non-CYP450-dependent metabolism and fluvastatin, which relies on the CYP2C9 isoform for biotransformation, are only modestly affected by the co-administration of CsA.31,123 CsA is unique in that it augments serum statin levels via 2 mechanisms. First, CsA competitively inhibits the CYP3A4 isozyme and increases blood levels of lovastatin, simvastatin and cervistatin. Fluvastatin is less affected by CsA due to alternative metabolism. Notably, HMGRIs tend not to affect the pharmacokinetics of CsA since CsA has a greater affinity for CYP3A4 and since its serum concentrations are approximately 10-fold higher.4 Second, CsA is known to induce cholestasis in humans.56 Smith and colleagues124 demonstrated that the cholestatic effect of CsA increased muscle HMGRI levels (up to 13- fold) and resulted in light microscopic changes including myofibre necrosis, interstitial edema and inflammatory cell infiltration. Interestingly, periodic acid-Schiff staining revealed decreased glycogen content in type IIb fibres, which were most sensitive to the myotoxic effects of HMGRIs. Decreased availability of glycolytic substrate and increased reliance on β-oxidation, in aerobically deficient cells, compounded by the possible statin-mediated impaired ETC function (i.e., decreased ubiquinone synthesis) may suppress myocyte viability. Mevalonate but not coenzyme Q10 supplementation ameliorated the myopathy suggesting that the toxic effect was not due to deficiency of the latter. 124 Interestingly, HMGRIs in certain experimental situations can induce apoptosis,66 and CsA inhibits the mitochondrial permeability transition pore (MPT) by preventing the binding of cyclophilin-D to the adenine nucleotide transporter (a component of the MPT).125,126 Therefore, it appears that, in the appropriate physiologic condition(s), the deleterious effects of HMGRIs overwhelm the protective effects CsA. Alternatively, HMGRI-mediated myofibre necrosis may not proceed through an MPTmediated pathway. Furthermore, CsA independently causes muscle dysfunction, characterized by Table 2: Various drugs metabolized by the human cytochrome P450 mixed oxidase isoenzyme system CYP1A2 CYP2C9 CYP2C19 CYP2D6 CYP2E1 Acetominophen Alprenolol Diazepam Amitriptyline Chloroxazone Caffeine Diclofenac Ibuprofen Bufaralol Ethanol Clozapine Mephenytoin Codeine Halothane Fluvastatin Phenacetin N-DMDZP MethylPB Debrisoquine Paracetamol Theophylline Tolbutamide Omeprazole Desipramine (S)-Warfarin Proguanil Dextromethorphan Phenytoin Encainide Flecainide Imipramine Metoprolol Mibefradil Nortriptyline Perhexiline Perphenazine Propafenone Propranolol Sparteine Thioridazine Timolol CYP3A4 Atorvastatin Cervistatin CsA Erythromycin Felodipine Lidocaine Lovastatin Mibefradil Midazolam Nefazodone Nifedipine Quinidine Simvastatin Triazolam Verapamil (R)-Warfarin N-DMDZP = N-desmethyldiazepam, MethylPB = methylphenobarbital, CsA = Cyclosporin A, (S)- and (R)-Warfarin = enantiomers of warfarin. Note, azole antifungals (itraconazole, fluconazole, ketoconazole and miconazole), the selective serotonin reuptake inhibitors (fluvoxamine, fluoxetine and sertraline) and cimetidine inhibit both the CYP2C and CYP3A4 isoforms. Quinidine, non-dihydropyridine calcium channel blockers and grapefruit inhibit the CYP3A4 isozyme. Trimethoprim-sulfamethoxazole, omeprazole, and amiodarone impair 2C activity. Rifampin and phenobarbitol induce CYP2C and CYP3A4. Carbamazepine and phenytoin also induce CYP3A4. Modified from Corsini A, Bellosta S, Baetta R, Fumagalli R, Paoletti R, Bernini F. New insights into the pharmacodynamic and pharmacokinetic properties of statins. Pharmacol Ther 1999;84:413-28, with permission from Elsevier Science. 266 Clin Invest Med • Vol 24, no 5, octobre 2001 Statin myopathies reduced muscle capillary density, mitochondrial respiration and endurance capacity.56 The other major HMGRI drug interaction occurs with hypolipemic agents such as fibric acid derivatives127–129 and niacin.47,128 Although fibrates can impair hepatic function the interaction appears to be more pharmacodynamic than pharmacokinetic.32 A plausible mechanism may be attributed to dual membrane-cholesterol lowering effects that result in increased sarcolemmal fluidity and subsequent destabilization.130,131 Conclusions and clinical approach From the current literature there are a few conclusions that can be made regarding the use of statins and myopathy. First, myalgias and cramps are the most frequent muscle-related side effects of statin therapy, while true myopathy is much less common (approximately 0.1 %). Second, there are several medications in which the potential for myotoxic interactions with statins is increased (i.e., CsA, erythromycin, fibric acid derivatives, niacin). Third, there are a few pre-existing conditions in which statins should not be used, such as untreated hypothyroidism, muscle coenzyme Q10 deficiency, mitochondrial cytopathies (except with coenzyme Q10 supplementation) and in patients in whom myopathy was documented with a statin (not absolute — see below). Fourth, the exact mechanism of action of the statins causing myopathy is unclear but may involve any or all of the following; coenzyme Q10 depletion, altered excitation-contraction coupling, decreased membrane fluidity, decreased sarcolemmal ionic flux and altered Ca2+ modulation. Currently there is insufficient evidence with which to propose a definitive clinical pathway for the care of patients with muscle symptoms who are taking statins; however, there are some guidelines that may be of benefit to the clinician as outlined below. In clinical practice, there are several scenarios that may arise in patients treated with statins; asymptomic hyperCKemia, myalgias with normal CK activity; myalgias with hyperCKemia; and the use of statins in patients with pre-existing neuromuscular disease. Prior to starting statin therapy it is important to measure baseline CK activity, thyroid-stimulating Clin Invest Med • Vol 24, no 5, October 2001 hormone level and liver enzymes at least once. In the absence of symptoms, there is no evidence to suggest that routine monitoring of plasma CK activity is of benefit. However, this is occasionally done in asymptomatic people and found to be elevated. In such a case, if the CK is less than 3 times the upper limit of normal and the physical examination and routine blood chemistry values are normal (complete blood count, thyroid-stimulating hormone and electrolytes levels), further evaluation is usually not revealing. In the case of myalgias or cramps (or both) associated with normal CK activity the clinician must consider other causes, and a physical examination and some blood tests (above tests plus measurement of plasma magnesium and calcium) may reveal a cause. If no cause is found, then the patient and the clinician must decide whether the symptoms warrant a discontinuance of therapy. Analgesics or antiinflammatory agents or even a brief trial of coenzyme Q10 (60 mg twice daily for 2 mo) may be considered. In the case of myalgias with hyperCKemia (assuming the baseline CK was normal), it is important to consider that another acquired myopathy may have developed and investigations may include a history, physical examination, blood chemistry measurements (thyroid-stimulating hormone, electrolytes, antinuclear antibody, complete blood count) and electromyography and nerve-conduction studies. Consideration may be given to a neuromuscular disease consult and possible a muscle biopsy, depending on the scenario. If the CK is greater than 10 times the upper limit of normal, screening for rhabdomyolysis and renal function is indicated, including measurement of uric acid, urine myoglobin, potassium, creatinine, bicarbonate and blood urea nitrogen. If renal dysfunction is found, the patient should be admitted to hospital and the nephrology department consulted. If there is no renal dysfunction, the statin therapy should be stopped and the patient should be followed up clinically and biochemically until resolution. At this point, the decision to switch to a hydrophilic statin (pravastatin) or another agent, or to avoid hypocholesterolemic medications requires careful assessment of the risk:benefit ratio of each decision. The role for coenzyme Q10 in treatment and prophylaxis is unclear; however, the case reports mentioned above suggest that at least in a 267 Baker and Tarnopolsky subgroup of patients, this may be of benefit. In general, the only patients with neuromuscular disorders who should not be given statins are those with untreated hypothyroidism, a rare form of myopathic coenzyme Q10 deficiency (6 cases reported worldwide) and patients with mitochondrial cytopathies76 (although treatment may be considered if simultaneous coenzyme Q10 is given in the latter group).85 With the recent interest in the rhabdomyolysis attributed to cerivastatin, it is hoped that further research into statin-induced myotoxicity will ensue and that more definitive clinical guidelines and a deeper understanding of the pathogenesis will emerge. References 1. The changing face of heart disease and stroke in Canada 2000. Executive summary. Ottawa: Health Canada. Available: www.hc-sc.gc.ca/hpb/lcdc/bcrdd /hdsc2000/index.html. Accessed Aug. 31, 2001. 2. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344: 1383-9. 3. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trial investigators. N Engl J Med 1996;335:1001-9. 4. Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med 1995;333:1301-7. 5. Maron DJ, Fazio S, Linton MF. Current perspectives on statins. Circulation 2000;101:207-13. 6. Beyer RE. An analysis of the role of coenzyme Q in free radical generation and as an antioxidant. Biochem Cell Biol 1992;70:390-403. 7. Rosenson RS, Lowe GD. Effects of lipids and lipoproteins on thrombosis and rheology. Atherosclerosis 1998;140:271-80. 8. Schwartz GG, Olsson AG, Ezekowitz MD, Ganz P, Oliver MF, Waters D, et al. Effects of atorvastatin on early recurrent ischemic events in acute coronary syndromes: the MIRACL study: a randomized controlled trial. JAMA 2001;285:1711-8. 9. Alberts MJ. Suppression of recurrent transient ischemic attacks by a statin agent. Neurology 2001;56: 531-2. 10. Dromer C, Vedrenne C, Billey T, Pages M, Fournie B, 268 Fournie A. [Rhabdomyolysis due to simvastin. Apropos of a case with review of the literature]. Rev Rhum Mal Osteoartic 1992;59:281-3. 11. Keogh A, Macdonald P, Kaan A, Aboyoun C, Spratt P, Mundy J. Efficacy and safety of pravastatin vs simvastatin after cardiac transplantation. J Heart Lung Transplant 2000;19:529-37. 12. Oldemeyer JB, Lund RJ, Koch M, Meares AJ, Dunlay R. Rhabdomyolysis and acute renal failure after changing statin-fibrate combinations. Cardiology 2000;94: 127-8. 13. Ozdemir O, Boran M, Gokce V, Uzun Y, Kocak B, Korkmaz S. A case with severe rhabdomyolysis and renal failure associated with cerivastatin-gemfibrozil combination therapy — a case report. Angiology 2000; 51:695-7. 14. Ma PT, Gil G, Sudhof TC, Bilheimer DW, Goldstein JL, Brown MS. Mevinolin, an inhibitor of cholesterol synthesis, induces mRNA for low density lipoprotein receptor in livers of hamsters and rabbits. Proc Natl Acad Sci U S A 1986;83:8370-4. 15. Ness GC, Chambers CM. Feedback and hormonal regulation of hepatic 3-hydroxy-3-methylglutaryl coenzyme A reductase: the concept of cholesterol buffering capacity. Proc Soc Exp Biol Med 2000;224:8-19. 16. Gascon Ramon G, Bertomeu Blanch F, Meneu Montoliu V, Fenollosa Tamarit MD. [Unnoticed hypothyroidism and myopathy due to lipid-lowering drugs]. Aten Primaria 2001;27:442-3. 17. Hung YT, Yeung VT. Hypothyroidism presenting as hypercholesterolaemia and simvastatin-induced myositis. Hong Kong Med J 2000;6:423-4. 18. Pia Iglesias G, Garrido Sanjuan JA, Gonzalez Gonzalez C, Sesma Sanchez P. [Antilipemic agents, hypothyroidism, and rhabdomyolysis]. Rev Clin Esp 2000;200: 236-7. 19. Maltz HC, Balog DL, Cheigh JS. Rhabdomyolysis associated with concomitant use of atorvastatin and cyclosporine. Ann Pharmacother 1999;33:1176-9. 20. Rodriguez JA, Crespo-Leiro MG, Paniagua MJ, Cuenca JJ, Hermida LF, Juffe A, et al. Rhabdomyolysis in heart transplant patients on HMG-CoA reductase inhibitors and cyclosporine. Transplant Proc 1999; 31:2522-3. 21. Bradford RH, Shear CL, Chremos AN, Dujovne CA, Franklin FA, Grillo RB, et al. Expanded Clinical Evaluation of Lovastatin (EXCEL) study results: two-year efficacy and safety follow-up. Am J Cardiol 1994;74: 667-73. 22. Frishman WH, Rapier RC. Lovastatin: an HMG-CoA reductase inhibitor for lowering cholesterol. Med Clin North Am 1989;73:437-48. 23. Haria M, McTavish D. Pravastatin: a reappraisal of its pharmacological properties and clinical effectiveness in the management of coronary heart disease. Drugs Clin Invest Med • Vol 24, no 5, octobre 2001 Statin myopathies 1997;53:299-336. 24. Lennernas H, Fager G. Pharmacodynamics and pharmacokinetics of the HMG-CoA reductase inhibitors. Similarities and differences. Clin Pharmacokinet 1997; 32:403-25. 25. Plosker GL, McTavish D. Simvastatin: a reappraisal of its pharmacology and therapeutic efficacy in hypercholesterolaemia. Drugs 1995;50:334-63. 26. Plosker GL, Wagstaff AJ. Fluvastatin: a review of its pharmacology and use in the management of hypercholesterolaemia. Drugs 1996;51:433-59. 27. Sirtori CR, Manzoni C, Lovati MR. Mechanisms of lipid-lowering agents. Cardiology 1991;78:226-35. 28. Cheng H, Rogers JD, Sweany AE, Dobrinska MR, Stein EA, Tate AC, et al. Influence of age and gender on the plasma profiles of 3-hydroxy-3-methylglutarylcoenzyme A (HMG-CoA) reductase inhibitory activity following multiple doses of lovastatin and simvastatin. Pharm Res 1992;9:1629-33. 29. Muck W. Rational assessment of the interaction profile of cerivastatin supports its low propensity for drug interactions. Drugs 1998;56(Suppl 1):15-23. 30. Stern RH, Gibson DM, Whitfield LR. Cimetidine does not alter atorvastatin pharmacokinetics or LDL-cholesterol reduction. Eur J Clin Pharmacol 1998;53:475-8. 31. Fischer V, Johanson L, Heitz F, Tullman R, Graham E, Baldeck JP, et al. The 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor fluvastatin: effect on human cytochrome P-450 and implications for metabolic drug interactions. Drug Metab Dispos 1999;27: 410-6. 32. Corsini A, Bellosta S, Baetta R, Fumagalli R, Paoletti R, Bernini F. New insights into the pharmacodynamic and pharmacokinetic properties of statins. Pharmacol Ther 1999;84:413-28. 33. Bellosta S, Bernini F, Ferri N, Quarato P, Canavesi M, Arnaboldi L, et al. Direct vascular effects of HMGCoA reductase inhibitors [review]. Atherosclerosis 1998;137Suppl:S101-9. 34. Rosenson RS, Tangney CC. Antiatherothrombotic properties of statins: implications for cardiovascular event reduction. JAMA 1998;279:1643-50. 35. Do TQ, Schultz JR, Clarke CF. Enhanced sensitivity of ubiquinone-deficient mutants of Saccharomyces cerevisiae to products of autoxidized polyunsaturated fatty acids. Proc Natl Acad Sci U S A 1996;93:7534-9. 36. Ernster L, Dallner G. Biochemical, physiological and medical aspects of ubiquinone function. Biochim Biophys Acta 1995;1271:195-204. 37. Zhang FL, Casey PJ. Protein prenylation: molecular mechanisms and functional consequences. Annu Rev Biochem 1996;65:241-69. 38. Brown MS, Goldstein JL. Drugs used in the treatment of hyperlipoproteinemias. In: Gilman AG, Rall TW, Clin Invest Med • Vol 24, no 5, October 2001 Nies AL, Taylor P, editors. The pharmacologic basis of therapeutics. Oxford: Pergamon Press; 1991. p. 874-96. 39. Flint OP, Masters BA, Gregg RE, Durham SK. HMG CoA reductase inhibitor-induced myotoxicity: pravastatin and lovastatin inhibit the geranylgeranylation of low-molecular-weight proteins in neonatal rat muscle cell culture. Toxicol Appl Pharmacol 1997;145:99-110. 40. Flint OP, Masters BA, Gregg RE, Durham SK. Inhibition of cholesterol synthesis by squalene synthase inhibitors does not induce myotoxicity in vitro. Toxicol Appl Pharmacol 1997;145:91-8. 41. Matzno S, Yamauchi T, Gohda M, Ishida N, Katsuura K, Hanasaki Y, et al. Inhibition of cholesterol biosynthesis by squalene epoxidase inhibitor avoids apoptotic cell death in L6 myoblasts. J Lipid Res 1997;38:1639-48. 42. van Vliet AK, Negre-Aminou P, van Thiel GC, Bolhuis PA, Cohen LH. Action of lovastatin, simvastatin, and pravastatin on sterol synthesis and their antiproliferative effect in cultured myoblasts from human striated muscle. Biochem Pharmacol 1996;52:1387-92. 43. Raiteri M, Arnaboldi L, McGeady P, Gelb MH, Verri D, Tagliabue C, et al. Pharmacological control of the mevalonate pathway: effect on arterial smooth muscle cell proliferation. J Pharmacol Exp Ther 1997;281: 1144-53. 44. Emmerich J, Aubert I, Bauduceau B, Dachet C, Chanu B, Erlich D, et al. Efficacy and safety of simvastatin (alone or in association with cholestyramine). A 1year study in 66 patients with type II hyperlipoproteinaemia. Eur Heart J 1990;11:149-55. 45. Israeli A, Raveh D, Arnon R, Eisenberg S, Stein Y. Lovastatin and elevated creatine kinase: results of rechallenge. Lancet 1989;1:725. 46. Reaven P, Witztum JL. Lovastatin, nicotinic acid, and rhabdomyolysis. Ann Intern Med 1988;109:597-8. 47. Tobert JA. Efficacy and long-term adverse effect pattern of lovastatin. Am J Cardiol 1988;62:28J-34J. 48. Waclawik AJ, Lindal S, Engel AG. Experimental lovastatin myopathy. J Neuropathol Exp Neurol 1993; 52:542-9. 49. Fukami M, Maeda N, Fukushige J, Kogure Y, Shimada Y, Ogawa T, et al. Effects of HMG-CoA reductase inhibitors on skeletal muscles of rabbits. Res Exp Med (Berl) 1993;193:263-73. 50. Chucrallah A, De Girolami U, Freeman R, Federman M. Lovastatin/gemfibrozil myopathy: a clinical, histochemical, and ultrastructural study. Eur Neurol 1992; 32:293-6. 51. Kogan AD, Orenstein S. Lovastatin-induced acute rhabdomyolysis. Postgrad Med J 1990;66:294-6. 52. Spach DH, Bauwens JE, Clark CD, Burke WG. Rhabdomyolysis associated with lovastatin and erythromycin use. West J Med 1991;154:213-5. 269 Baker and Tarnopolsky 53. Bakris GL, Lass N, Gaber AO, Jones JD, Burnett JC Jr. Radiocontrast medium-induced declines in renal function: a role for oxygen free radicals. Am J Physiol 1990;258:F115-20. 54. Baliga R, Ueda N, Walker PD, Shah SV. Oxidant mechanisms in toxic acute renal failure. Am J Kidney Dis 1997;29:465-77. 55. Yoshioka T, Fogo A, Beckman JK. Reduced activity of antioxidant enzymes underlies contrast mediainduced renal injury in volume depletion. Kidney Int 1992;41:1008-15. 56. Mosieniak G, Figiel I, Kaminska B. Cyclosporin A, an immunosuppressive drug, induces programmed cell death in rat C6 glioma cells by a mechanism that involves the AP-1 transcription factor. J Neurochem 1997;8:1142-9. 57. De Pinieux G, Chariot P, Ammi-Said M, Louarn F, Lejonc JL, Astier A, et al. Lipid-lowering drugs and mitochondrial function: effects of HMG-CoA reductase inhibitors on serum ubiquinone and blood lactate/pyruvate ratio. Br J Clin Pharmacol 1996;42:333-7. 58. Elmberger PG, Kalen A, Lund E, Reihner E, Eriksson M, Berglund L, et al. Effects of pravastatin and cholestyramine on products of the mevalonate pathway in familial hypercholesterolemia. J Lipid Res 1991; 32:935-40. 59. Folkers K, Langsjoen P, Willis R, Richardson P, Xia LJ, Ye CQ, et al. Lovastatin decreases coenzyme Q levels in humans. Proc Natl Acad Sci U S A 1990;87: 8931-4. 60. Ghirlanda G, Oradei A, Manto A, Lippa S, Uccioli L, Caputo S, et al. Evidence of plasma CoQ10-lowering effect by HMG-CoA reductase inhibitors: a doubleblind, placebo-controlled study. J Clin Pharmacol 1993;33:226-9. 61. Kaplan L, Fearn J, Laskarewski P, Stein E. Serum ubiquinone Q10 levels: effect of cholesterol lowering drugs [abstract]. Clin Chem 1990;36:963. 62. Thibault A, Samid D, Tompkins AC, Figg WD, Cooper MR, Hohl RJ, et al. Phase I study of lovastatin, an inhibitor of the mevalonate pathway, in patients with cancer. Clin Cancer Res 1996;2:483-91. 63. Willis RA, Folkers K, Tucker JL, Ye CQ, Xia LJ, Tamagawa H. Lovastatin decreases coenzyme Q levels in rats. Proc Natl Acad Sci U S A 1990;87:8928-30. 64. Forsmark-Andree P, Lee CP, Dallner G, Ernster L. Lipid peroxidation and changes in the ubiquinone content and the respiratory chain enzymes of submitochondrial particles. Free Radic Biol Med 1997;22:391-400. 65. Noack H, Kube U, Augustin W. Relations between tocopherol depletion and coenzyme Q during lipid peroxidation in rat liver mitochondria. Free Radic Res 1994;20:375-86. 66. Mutoh T, Kumano T, Nakagawa H, Kuriyama M. Involvement of tyrosine phosphorylation in HMG-CoA 270 reductase inhibitor-induced cell death in L6 myoblasts. FEBS Lett 1999;444:85-9. 67. Nakagawa H, Mutoh T, Kumano T, Kuriyama M. HMG-CoA reductase inhibitor-induced L6 myoblast cell death: involvement of the phosphatidylinositol 3kinase pathway. FEBS Lett 1998;438:289-92. 68. Kagan T, Davis C, Lin L, Zakeri Z. Coenzyme Q10 can in some circumstances block apoptosis, and this effect is mediated through mitochondria. Ann N Y Acad Sci 1999;887:31-47. 69. Artuch R, Colome C, Vilaseca MA, Pineda M, Campistol J. [Ubiquinone: metabolism and functions. Ubiquinone deficiency and its implication in mitochondrial encephalopathies. Treatment with ubiquinone]. Rev Neurol 1999;29:59-63. 70. Musumeci O, Naini A, Slonim AE, Skavin N, Hadjigeorgiou GL, Krawiecki N, et al. Familial cerebellar ataxia with muscle coenzyme Q10 deficiency. Neurology 2001;56:849-55. 71. Rotig A, Appelkvist EL, Geromel V, Chretien D, Kadhom N, Edery P, et al. Quinone-responsive multiple respiratory-chain dysfunction due to widespread coenzyme Q10 deficiency. Lancet 2000;356:391-5. 72. Sobreira C, Hirano M, Shanske S, Keller RK, Haller RG, Davidson E, et al. Mitochondrial encephalomyopathy with coenzyme Q10 deficiency. Neurology 1997;48:1238-43. 73. Judy WV, Stogsdill WW, Folkers K. Myocardial preservation by therapy with coenzyme Q10 during heart surgery. Clin Investig 1993;71:S155-61. 74. Manzoli U, Rossi E, Littarru GP, Frustaci A, Lippa S, Oradei A, et al. Coenzyme Q10 in dilated cardiomyopathy. Int J Tissue React 1990;12:173-8. 75. Sole MJ, Jeejeebhoy KN. Conditioned nutritional requirements and the pathogenesis and treatment of myocardial failure. Curr Opin Clin Nutr Metab Care 2000;3:417-24. 76. Abe K, Fujimura H, Nishikawa Y, Yorifuji S, Mezaki T, Hirono N, et al. Marked reduction in CSF lactate and pyruvate levels after CoQ therapy in a patient with mitochondrial myopathy, encephalopathy, lactic acidosis and stroke-like episodes (MELAS). Acta Neurol Scand 1991;83:356-9. 77. Mortensen SA, Leth A, Agner E, Rohde M. Doserelated decrease of serum coenzyme Q10 during treatment with HMG-CoA reductase inhibitors. Mol Aspects Med 1997;18Suppl:S137-44. 78. Nambudiri AM, Ranganathan S, Rudney H. The role of 3-hydroxy-3-methylglutaryl coenzyme A reductase activity in the regulation of ubiquinone synthesis in human fibroblasts. J Biol Chem 1980;255:5894-9. 79. Chariot P, Abadia R, Agnus D, Danan C, Charpentier C, Gherardi RK. Simvastatin-induced rhabdomyolysis followed by a MELAS syndrome. Am J Med 1993;94: 109-10. Clin Invest Med • Vol 24, no 5, octobre 2001 Statin myopathies 80. Walravens PA, Greene C, Frerman FE. Lovastatin, isoprenes, and myopathy. Lancet 1989;2:1097-8. 81. Arnadottir M, Eriksson LO, Thysell H, Karkas JD. Plasma concentration profiles of simvastatin 3hydroxy-3-methyl-glutaryl-coenzyme A reductase inhibitory activity in kidney transplant recipients with and without ciclosporin. Nephron 1993;65:410-3. 82. Ihara Y, Namba R, Kuroda S, Sato T, Shirabe T. Mitochondrial encephalomyopathy (MELAS): pathological study and successful therapy with coenzyme Q10 and idebenone. J Neurol Sci 1989;90:263-71. 83. Nishikawa Y, Takahashi M, Yorifuji S, Nakamura Y, Ueno S, Tarui S, et al. Long-term coenzyme Q10 therapy for a mitochondrial encephalomyopathy with cytochrome c oxidase deficiency: a 31P NMR study. Neurology 1989;39:399-403. 84. Lam CW, Lau CH, Williams JC, Chan YW, Wong LJ. Mitochondrial myopathy, encephalopathy, lactic acidosis and stroke-like episodes (MELAS) triggered by valproate therapy. Eur J Pediatr 1997;156:562-4. 85. Abe K, Matsuo Y, Kadekawa J, Inoue S, Yanagihara T. Effect of coenzyme Q10 in patients with mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS): evaluation by noninvasive tissue oximetry. J Neurol Sci 1999;162:65-8. 86. Chan A, Reichmann H, Kogel A, Beck A, Gold R. Metabolic changes in patients with mitochondrial myopathies and effects of coenzyme Q10 therapy. J Neurol 1998;245:681-5. 87. Laaksonen R, Jokelainen K, Laakso J, Sahi T, Harkonen M, Tikkanen MJ, et al. The effect of simvastatin treatment on natural antioxidants in low-density lipoproteins and high-energy phosphates and ubiquinone in skeletal muscle. Am J Cardiol 1996; 77:851-4. 88. Laaksonen R, Jokelainen K, Sahi T, Tikkanen MJ, Himberg JJ. Decreases in serum ubiquinone concentrations do not result in reduced levels in muscle tissue during short-term simvastatin treatment in humans. Clin Pharmacol Ther 1995;57:62-6. 89. Ponchaut S, Van Hoof F, Veitch K. Valproate and cytochrome c oxidase deficiency. Eur J Pediatr 1995; 154:79. 90. Elmberger PG, Kalen A, Brunk UT, Dallner G. Discharge of newly-synthesized dolichol and ubiquinone with lipoproteins to rat liver perfusate and to the bile. Lipids 1989;24:919-30. 91. Johansen K, Theorell H, Karlsson J, Diamant B, Folkers K. Coenzyme Q10, alpha-tocopherol and free cholesterol in HDL and LDL fractions. Ann Med 1991;23: 649-56. 92. Laaksonen R, Ojala JP, Tikkanen MJ, Himberg JJ. Serum ubiquinone concentrations after short- and long-term treatment with HMG-CoA reductase inhibitors. Eur J Clin Pharmacol 1994;46:313-7. Clin Invest Med • Vol 24, no 5, October 2001 93. Maltese WA, Aprille JR. Relation of mevalonate synthesis to mitochondrial ubiquinone content and respiratory function in cultured neuroblastoma cells. J Biol Chem 1985;260:11524-9. 94. Caliskan S, Caliskan M, Kuralay F, Onvural B. Effect of simvastatin therapy on blood and tissue ATP levels and erythrocyte membrane lipid composition. Res Exp Med (Berl) 2000;199:189-94. 95. Beyer RE. The participation of coenzyme Q in free radical production and antioxidation. Free Radic Biol Med 1990;8:545-65. 96. Lankin VZ, Tikhaze AK, Kaminnaia VI, Kaminnyi AI, Konovalova GG, Kukharchuk VV. [Intensification in vivo of free radical oxidation of low density lipoproteins in plasma from patients with myocardial ischemia treated by HMG-CoA-reductase pravastatin and suppression of lipid peroxidation by ubiquinone Q10]. Biull Eksp Biol Med 2000;129:176-9. 97. Peters O, Back T, Lindauer U, Busch C, Megow D, Dreier J, et al. Increased formation of reactive oxygen species after permanent and reversible middle cerebral artery occlusion in the rat. J Cereb Blood Flow Metab 1998;18:196-205. 98. Piantadosi CA, Zhang J. Mitochondrial generation of reactive oxygen species after brain ischemia in the rat. Stroke 1996;27:327-31. 99. Chello M, Mastroroberto P, Romano R, Bevacqua E, Pantaleo D, Ascione R, et al. Protection by coenzyme Q10 from myocardial reperfusion injury during coronary artery bypass grafting. Ann Thorac Surg 1994;58: 1427-32. 100. Crestanello JA, Kamelgard J, Lingle DM, Mortensen SA, Rhode M, Whitman GJ. Elucidation of a tripartite mechanism underlying the improvement in cardiac tolerance to ischemia by coenzyme Q10 pretreatment. J Thorac Cardiovasc Surg 1996;111:443-50. 101. Hano O, Thompson-Gorman SL, Zweier JL, Lakatta EG. Coenzyme Q10 enhances cardiac functional and metabolic recovery and reduces Ca2+ overload during postischemic reperfusion. Am J Physiol 1994;266: H2174-81. 102. Singh RB, Wander GS, Rastogi A, Shukla PK, Mittal A, Sharma JP, et al. Randomized, double-blind placebo-controlled trial of coenzyme Q10 in patients with acute myocardial infarction. Cardiovasc Drugs Ther 1998;12:347-53. 103. Sunamori M, Tanaka H, Maruyama T, Sultan I, Sakamoto T, Suzuki A. Clinical experience of coenzyme Q10 to enhance intraoperative myocardial protection in coronary artery revascularization. Cardiovasc Drugs Ther 1991;5(Suppl 2):297-300. 104. Pierno S, De Luca A, Tricarico D, Ferrannini E, Conte T, D’Alo G, et al. Experimental evaluation of the effects of pravastatin on electrophysiological parameters of rat skeletal muscle. Pharmacol Toxicol 1992;71:325-9. 271 Baker and Tarnopolsky 105. Pierno S, De Luca A, Tricarico D, Roselli A, Natuzzi F, Ferrannini E, et al. Potential risk of myopathy by HMG-CoA reductase inhibitors: a comparison of pravastatin and simvastatin effects on membrane electrical properties of rat skeletal muscle fibers. J Pharmacol Exp Ther 1995;275:1490-6. 106. Gray DF, Bundgaard H, Hansen PS, Buhagiar KA, Mihailidou AS, Jessup W, et al. HMG CoA reductase inhibition reduces sarcolemmal Na(+)-K(+) pump density. Cardiovasc Res 2000;47:329-35. 107. Pierno S, De Luca A, Liantonio A, Camerino C, Conte Camerino D. Effects of HMG-CoA reductase inhibitors on excitation-contraction coupling of rat skeletal muscle. Eur J Pharmacol 1999;364:43-8. 108. Mutoh T, Kumano T, Nakagawa H, Kuriyama M. Role of tyrosine phosphorylation of phospholipase C gamma1 in the signaling pathway of HMG-CoA reductase inhibitor-induced cell death of L6 myoblasts. FEBS Lett 1999;446:91-4. 109. Katsilambros NJ, Braaten J, Ferguson B, Bradley R. Muscular syndrome after clofibrate. N Engl J Med 1972;286:1110-1. 110. Sekowski I, Samuel P. Clofibrate-induced acute muscular syndrome. Am J Cardiol 1972;30:572-4. 111. Cornelius F. Functional reconstitution of the sodium pump. Kinetics of exchange reactions performed by reconstituted Na/K-ATPase. Biochim Biophys Acta 1991;1071:19-66. 112. Yeagle PL. Modulation of membrane function by cholesterol. Biochimie 1991;73:1303-10. 113. Moghadasian MH. Clinical pharmacology of 3hydroxy-3-methylglutaryl coenzyme A reductase inhibitors. Life Sci 1999;65:1329-37. 114. Chu A, Stefani E. Phosphatidylinositol 4,5-bisphosphate-induced Ca2+ release from skeletal muscle sarcoplasmic reticulum terminal cisternal membranes. Ca2+ flux and single channel studies. J Biol Chem 1991;266:7699-705. 115. Tarnopolsky MA, Hicks A, Winegard K. The effects of lithium on muscle contractile function in humans. Muscle Nerve 1996;19:311-8. 116. Veerkamp JH, Smit JW, Benders AA, Oosterhof A. Effects of HMG-CoA reductase inhibitors on growth and differentiation of cultured rat skeletal muscle cells. Biochim Biophys Acta 1996;1315:217-22. 117. Margreth A, Damiani E, Bortoloso E. Sarcoplasmic reticulum in aged skeletal muscle. Acta Physiol Scand 1999;167:331-8. 118. Yamaguchi M, Hanahisa Y, Murata T. Expression of calcium-binding protein regucalcin and microsomal Ca2+-ATPase regulation in rat brain: attenuation with increasing age. Mol Cell Biochem 1999;200:43-9. 119. Beal MF. Aging, energy, and oxidative stress in neurodegenerative diseases. Ann Neurol 1995;38:357-66. 272 120. Kantola T, Kivisto KT, Neuvonen PJ. Effect of itraconazole on the pharmacokinetics of atorvastatin. Clin Pharmacol Ther 1998;64:58-65. 121. Kantola T, Kivisto KT, Neuvonen PJ. Erythromycin and verapamil considerably increase serum simvastatin and simvastatin acid concentrations. Clin Pharmacol Ther 1998;64:177-82. 122. Muck W, Ochmann K, Rohde G, Unger S, Kuhlmann J. Influence of erythromycin pre- and co-treatment on single-dose pharmacokinetics of the HMG-CoA reductase inhibitor cerivastatin. Eur J Clin Pharmacol 1998; 53:469-73. 123. Olbricht C, Wanner C, Eisenhauer T, Kliem V, Doll R, Boddaert M, et al. Accumulation of lovastatin, but not pravastatin, in the blood of cyclosporine-treated kidney graft patients after multiple doses. Clin Pharmacol Ther 1997;62:311-21. 124. Smith PF, Eydelloth RS, Grossman SJ, Stubbs RJ, Schwartz MS, Germershausen JI, et al. HMG-CoA reductase inhibitor-induced myopathy in the rat: cyclosporine A interaction and mechanism studies. J Pharmacol Exp Ther 1991;257:1225-35. 125. Halestrap AP, Connern CP, Griffiths EJ, Kerr PM. Cyclosporin A binding to mitochondrial cyclophilin inhibits the permeability transition pore and protects hearts from ischaemia/reperfusion injury. Mol Cell Biochem 1997;174:167-72. 126. Halestrap AP, Kerr PM, Javadov S, Woodfield KY. Elucidating the molecular mechanism of the permeability transition pore and its role in reperfusion injury of the heart. Biochim Biophys Acta 1998;1366:79-94. 127. Duell PB, Connor WE, Illingworth DR. Rhabdomyolysis after taking atorvastatin with gemfibrozil. Am J Cardiol 1998;81:368-9. 128. Garnett WR. Interactions with hydroxymethylglutarylcoenzyme A reductase inhibitors. Am J Health Syst Pharm 1995;52:1639-45. 129. Miller DB, Spence JD. Clinical pharmacokinetics of fibric acid derivatives (fibrates). Clin Pharmacokinet 1998;34:155-62. 130. London SF, Gross KF, Ringel SP. Cholesterol-lowering agent myopathy (CLAM). Neurology 1991;41: 1159-60. 131. Pierce LR, Wysowski DK, Gross TP. Myopathy and rhabdomyolysis associated with lovastatin-gemfibrozil combination therapy. JAMA 1990;264:71-5. Reprint requests to: Dr. Mark A. Tarnopolsky, Department of Medicine (Neurology and Rehabilitation), Rm. 4U4, McMaster University Medical Center, Hamilton ON L8N 3Z5; fax 905 521-2656, [email protected] Clin Invest Med • Vol 24, no 5, octobre 2001