Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
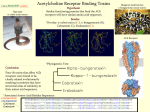
PHARMACOLOGY Dr. Husam Aldeen Salim Alnajar Atropine • Characteristics of Atropine • Source – Atropa belladonna • Chemical nature – An alkaloid ANTIMUSCARINIC AGENTS BELLADONNA ALKALOIDS • ATROPINE • SCOPOLAMINE TX: USED WHEN A REDUCTION OF PARASYMATHETIC TONE IS DESIRABLE • PREOP TO REDUCE SALIVATIONS / BRONCHIAL SECRETIONS • REDUCE INTESTINAL MOTILITY • TREAT OVERACTIVE BLADDER • OPHTHALMOLOGICAL EXAMINATIONS • PREVENTING MOTION SICKNESS • TREAT ASTHMA • TREAT POISONING BY AChE INHIBITOR Effect Of Atropine in Relation to Dosage ... • DOSE EFFECT • 0.5 mg Slight decline in heart rate • Some dryness of mouth • Inhibition of sweating • DOSE EFFECT • 1.0 mg Definit dryness of mouth • Thirst • Inreased heart rate, sometimes preceded by slowing • Mild dilatation of pupil • DOSE EFFECT • 2.0 mg Rapid heart rate • Palpitation • Marked dryness of mouth • Dilated pupils • Some blurring of near vision • DOSE • 5.0 mg EFFECT All the previous symptoms are marked • Difficulty in speaking and swallowing Restlessness and fatigue • • • • Headache Dry hot skin Difficulty in micturition Reduced intestinal peristalsis • DOSE • 10 mg • and more • • • • • • • EFFECT Previous symtoms are more marked Pulse, rapid and weak Iris practically obliterated Vision very blurred Skin flushed, hot, dry, and scarlet Ataxia Restlessness and excitement Hallucinations and delirium Coma ATROPINE: OVERVIEW OF TOXIC ACTIONS DRY AS A BONE HOT AS A PISTOL RED AS A BEET BLIND AS A BAT MAD AS A HATTER Therapeutic Uses of Antimuscarinic Agents • Cardiovascular System - atropine is generally used for the following cases – Sinus or nodal bradycardia in cases of excessive vagal tone associated with myocardial infarct – Hyperactive carotid sinus (syncope and severe bradycardia) – Second degree heart block • Gastrointestinal Tract – Peptic ulcers • M1 muscarinic receptor antagonists such as pirenzepine and telenzepine are used – Spasticity of the g.i. tract – Excessive salivation associated with heavy metal poisoning and parkinsonism – Production of partial blockade of salivation in patients unable to swallow • Urinary Bladder – Reverse spasm of the ureteral smooth muscle (renal colic) – Increase bladder capacity in cases of enuresis • Reduce urinary frequency in cases of hypertonic bladder • Central Nervous System – Parkinson’s disease – Motion sickness – Anesthesia, to inhibit salivation – Prevent vagal reflexes induced by surgical manipulation of organs • Posioning by inhibitors of acetylcholinesterase • Mushroom poisoning due to muscarine • In conjunction with inhibitors of acetylcholinesterase when they are used to promote recovery from neuromuscular blockade after surgery • Prevent vagal reflexes induced by surgical manipulation of visceral organs Drugs of Other Classes With Antimuscarinic Activity • Tricyclic antidepressants – Imipramine – Amitriptyline – Protriptyline • Phenothiazine Antipsychotic Agents – Chlorpromazine & Thioridazine • H1 Histamine receptor blocking agents – Diphenhydramine – Promethazine – Chlorpheniramine – Cyproheptadine Contraindications to the Use of Antimuscarinic Agents • • • • Narrow angle glaucoma Hypertrophy of the prostate gland Atony of the bladder Atony of the G.I. Tract Adrenergic Receptors NE 1, 2, 1 CNS ACh C T ACh ACh L S ACh SM CNS ACh C T ACh M N ACh N L S ACh SM N CNS ACh C T ACh M N ACh NE N L S NE ACh SM N CNS ACh C T ACh M N 1 ACh NE N L S NE 1 2 ACh SM N CNS ACh C T ACh M N 1 ACh NE N L N S NE 1 EPI ACh 2 ACh SM N EPI 1, 2, 1, 2 NE 1, 2, 1 Adrenergic Receptors Differences between autonomic and somatic nerves Autonomic: - Innervates all organs/glands except skeletal muscle - Synapses located in ganglions outside cerebrospinal axis - Extensive peripheral plexuses - Postganglionic nerves are not myelinated - Some level of spontaneous activity without intact innervation Somatic: - Innervates only skeletal muscle - Synapses within CNS - Does not form peripheral plexuses - myelinated - Denervation results in paralysis, atrophy Differences between functions of the parasympathetic and sympathetic nervous system Parasympathetic: - Conservation of energy - Urine output increased - Salivation increased - Bradycardia - Respiration reduced - Vasodilator predominance - Blood pressure reduced - GI motility and secretions increased - Renal blood flow increased Sympathetic: - Expenditure of energy - Tachycardia - Vasoconstrictor predominance - Blood pressure increased - Renal blood flow decreased - Urine output decreased - Salivation reduced - Respiration increased - GI motility and secretions reduced EFFECTS OF STIMULATING MUSCARINIC RECEPTORS SITE HEART VASCULATURE AIRWAYS IRIS (SLUDE) EFFECT BRADYCARDIA VASODILATION BRONCHOSPASM MIOSIS BLADDER INCREASED URINATION GI TRACT INCREASED GI MOTILITY SALIVARY GLANDS INCREASED SALIVATION LACRIMAL GLANDS INCREASED TEARS SWEAT GLANDS INCREASED SWEATNG EFFECTS OF STIMULATING ADRENERGIC RECEPTORS 1 contractile force heart rate 2 vasodilation, TPR 1, 2 vasoconstriction TPR EFFECTS OF STIMULATING ADRENERGIC RECEPTORS SITE HEART VASCULATURE AIRWAYS IRIS EFFECT TACHYCARDIA (1) VASODILATION (2) VASOCONSTRICTION (1, 2) BRONCHORELAXATION (2) MYDRIASIS (2) BLADDER DECREASED URINATION (2) GI TRACT DECREASED GI MOTILITY (2) UTERUS RELAXATION (2) Dual Innervation Exceptions - blood vessels (only sympathetic) Predominant Tone Primarily parasympathetic NS Exceptions - blood vessels (sympathetic) - sweat glands (sympathetic cholinergic) Predominate Autonomic Tone Site Predominate Tone Arterioles Veins Sympathetic (adrenergic) Sympathetic (adrenergic) Heart Iris Ciliary muscle GI tract Urinary bladder Salivary glands Parasympathetic (cholinergic) Parasympathetic (cholinergic) Parasympathetic (cholinergic) Parasympathetic (cholinergic) Parasympathetic (cholinergic) Parasympathetic (cholinergic) Sweat glands Sympathetic (cholinergic) PRESYNAPTIC POSTSYNAPTIC NE - predominately removed from synapse via re-uptake 1 Metabolic Removal Re-uptake 2 Re-uptake 1 NE synthesis COMT MAO NE NE / (-) 2 Receptor Binding Action 1 contractile force heart rate renin release 2 1, 2 vasodilation, TPR vasoconstriction TPR MIXED ADRENERGIC AGONISTS Norepinephrine 1, 2, 1 Epinephrine 1, 2, 1, 2 Dopamine DA, 1, 1 MIXED ADRENERGIC AGONISTS Norepinephrine Epinephrine (1, 2, 1) (1, 2, 1, 2) Tx: ● Asthma (but there are better drugs) ● Anaphylactic shock, ● Cardiogenic shock ● Prolong action of local anesthetics ● Topical hemostatic agent Dopamine (DA, 1, 1) Tx: ● CHF ALPHA AGONISTS - Phenylephrine (1) - Methoxamine (1) - Oxymetazoline (1 and 2 in periphery) - Tetrahydrozoline (1) - Naphazoline (1) - Ephedrine/Pseudoephedrine - Clonidine (1) (2, Tx site of action is CNS) BETA AGONISTS Non-selective 1/2 – Isoproterenol Selective 2 – Albuterol – Terbutaline Selective 1 – Dobutamine – Metaproterenol – Isoetharine – Bitolterol – Ritodrine Adrenergic Antagonists CNS ACh C ACh M N T ACh NE N L N S X X1 NE EPI X ACh 2 ACh SM N 1 ALPHA ANTAGONISTS Nonselective 1 and 2 receptor antagonists - Phenoxybenzamine - Phentolamine Used in pts with pheochromocytoma Selective 1 receptor antagonists - Prazosin - Terazosin (water soluble) Used Tx as antihypertensive agents Effects of Alpha-Receptor Blockade on Vascular Smooth Muscle Tone VSMC Re-uptake 1 NE NE 1 Vasoconstriction (-) 2 Phentolamine - 1 and 2 blockade Prozosin - 1 blockade Vasodilation Vasodilation BETA ANTAGONISTS ● Non-selective 1, 2 ● ‘Cardio’- Selective 1 Propranolol Atenolol Nadolol Metropolol Esmolol Timolol Pindolol Carteolol Acebutolol (ISA) Intrinsic Sympathomimetic Activity ● Non-selective 1, 2, 1 Labetalol Carvedilol INDIRECT ACTING ADRENERGIC AGONISTS Tyramine (dietary substance) Uptake Blockers • Cocaine • Tricyclic Antidepressants Cocaine PRESYNAPTIC POSTSYNAPTIC Re-uptake 1 NE NE / Receptor Binding Action Cocaine PRESYNAPTIC POSTSYNAPTIC Re-uptake 1 cocaine NE X NE / Receptor Binding Action Neuronal Blockers • Guanethadine Inhibits NE release, also causes NE depletion, and can damage NE neurons • Reserpine Depletes NE stores by inhibiting vesicular uptake of NE, NE then metabolized by intra-neuronal MAO Monoamine Oxidase (MAO) Inhibitors • Pargyline • Tranylcypromine Tyramine (or other drugs that promote NE release) may cause markedly increased blood pressure in patients taking MAO inhibitors