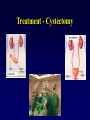
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
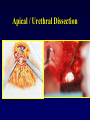
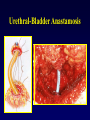
Urologic Oncology Raj S. Pruthi, M.D. Division of Urologic Surgery The University of North Carolina at Chapel Hill Question 1 • Which of the following is true regarding prostate ca.? – – – – Common cancer with high mortality Common cancer with low mortality Uncommon cancer with high mortality Uncommon cancer with low mortality Question 2 • What is the most common symptom of localized prostate ca.? – – – – Hematuria Urinary sx’s -- frequency,nocturia Bony pain No symptoms Question 3 • Prostate ca. screening should begin at age… – – – – 80 65 50 30 Question 4 • The following are common treatments of prostate ca. except – – – – surgery radiation chemotherapy castration Question 5 • The following groups have an increased relative risk of prostate ca. Development, except…. – – – – family history Americans African-Americans h/o STDs Question 6 • The most common factor associated with bladder cancer develoment in the U.S. is… – family history – h/o STDs – industrial exposure -- aniline dyes/aromatic amines – smoking Question 7 • The most symptom of bladder cancer is… – – – – no symptoms hematuria recurrent UTIs bony pain Question 8 • Bladder cancer is most commonly… – – – – adenocarcinoma squamous cell ca. transitional cell ca. clear cell ca. Question 9 • Renal cell carcinoma – is a “transitional cell ca” cell type – has a very benign course / does not typically require any treatment – typically requires a nephrectomy for localized disease – is very responsive to radiation therapy Question 10 • Testicular cancer…. – is rarely curable – is resistant to chemotherapy – commonly presents a painless testicular lump – is most common in men over age 40 Prostate Cancer • 200,000 new cases per year -- 1st • 40,000 deaths per year -- 2nd • Lifetime risk = 1 in 8 Presentation • 1950 – 28% localized – 72% locally-extensive / metastatic • 2000 – 80% localized (no symptoms) – 20% locally-extensive / metastatic Prostate Cancer: Symptoms • Localized (curable) = NONE! • Locally-extensive = voiding symptoms • Metastatic = bony pain – spine, pelvis, ribs, skull, long bones (prostate cancer patients may have BPH) Risk Factors • • • • Age Ethnicity Family History Geographic Variation Age • 95% occur ages 45 - 90 • exponential increase after age 50 age <40 40-59 60-79 risk 1 in 10,000 1 in 100 1 in 8 Ethnicity Relative risk (# / 100,000) • African Americans • White Americans • Japanese Americans 90 50 20 • Native Japanese 5 Geographic Variation HIGH MEDIUM LOW Family History • 10 % are familial • Most occur in patients < age 55 • Those with family hx have higher risk: – 1 relative – 2 relatives – 3 relatives 2X 5X 11X Detection » PSA (prostate specific antigen) » DRE (digital rectal exam) Detection: PSA • • • • serine protease bound and free forms produced by prostate tissue only produced by benign and malignant cells – not cancer specific • cancer produces higher levels PSA PSA: Elevation » » » » CANCER Enlarged prostate (BPH) Prostatitis Prostate infarct Ø DRE Ø Bicycle riding, sexual activity, etc. Screening • YEARLY AFTER AGE 50 • YEARLY AFTER AGE 40 – African-Americans – Family History Detection • Abnormal DRE OR • Abnormal PSA BIOPSY TRUS / PNBx Pathology • Adenocarcinoma • Spread by direct extension, perineural invasion, lymphatics • Found in peripheral zone • Spread to – seminal vesicles – lymph nodes – bones Pathology: Grade • Gleason score ( 2-10) – 2-6 = low grade – 7 = intermediate – 8-10 = high grade • Important prognostic info. • High grades = aggressive cancers Pathology: Stage A B C D1 D2 PSA or TURP detected Nodule on Prostate Extends beyond Prostate Spread to LNs Distant Spread (bones) T1 T2 T3,T4 N+ M+ Treatment • Nothing - “Watchful Waiting” • Surgery - “Radical Prostatectomy” • Radiation – “External Beam Radiation” – “Brachytherapy” • Hormone - “Androgen Ablation” Treatment Options • T1, T2 surgery, radiation (ebRT, brachy), watchful waiting • T3, T4 radiation (ebRT), hormones • N+, M+ hormones Radical Prostatectomy Radical Prostatectomy Radical Prostatectomy Puboprostatic Ligs. / DVC Apical / Urethral Dissection Lateral Pedicles Seminal Vesicles Bladder Neck Bladder Neck Preservation Urethral-Bladder Anastamosis Prostate Specimen Radical Prostatectomy Bladder Cancer • • • • 40,000 cases per year 10,000 deaths per year 2nd most common urologic malignancy males:females = 3:1 Pathology • Transitional cell ca. = 90% • Squamous cell ca. = 8% • Adenoca. = 2% Etiology • Enviromental factors – – – – – cigarettes carcinogenic aromatic amines cyclophosphamide pelvic irradiation schistosomiasis Stage A A B C D confined to epithelium invade submucosa invade muscle Extends perivesicle fat Spread to LNs, Distant Ta T1 T2, 3a T3bc,4 N+M+ Signs / Symptoms • Hematuria • Irritative voiding sx’s Diagnosis • • • • Cystoscopy Urine Cytology IVP / CT TURBT Treatment • Superficial (Ta,T1) – TURBT +/intravesical therapy • Muscle-invasive (T2,3a) – cystectomy • Metastatic – chemotherapy Treatment - Cystectomy Upper tract TCCa • Renal pelvis / ureter • Dx: IVP, cytology, ureteroscopy • Rx: – Nephroureterectomy – partial (distal) ureterctomy – laser ablation • F/U: Bladder surveillence Renal Cell Carcinoma • 20,000 new cases per year • 10,000 deaths per year • males:females = 2:1 Pathology • Adenocarcinoma • arise from proximal tubule • spread via direct extension, lymphatics, hematogenous • Spread to: – LNs, lung, bone, liver Signs / Symptoms • Hematuria • Flank pain • Flank mass • Incidentally discovered Diagnosis • CT scan with / without contrast – heterogeneous, enhancing mass • Renal ultrasound • MRI • IVP Stage I II III IV confined to kidney confined to Gerotas renal vein, v. cava , LNs Adj.orgs, distant met T1,T2 T3a T3bc,N+ T4, M+ Treatment • T1, T2, T3 – radical nephrectomy – cavotomy/extract tumor thrombus for T3b,c • T4,N+,M+ – immunotherapy (+/- nephrectomy) Tumor Thrombus Tumor Thrombus Radical Nephrectomy Patient positioning: Flank Radical Nephrectomy Partial nephrectomy Incisions Radical Nephrectomy Radical Nephrectomy Partial nephrectomy Hilar Vessels Renal Vein Renal Artery Incisions Renal Tumors • • • • • RCCa Angiomyolipoma Oncocytoma Renal pelvic TCCa Complex renal cysts Survival (5-year) • • • • I = 75% II = 65% III = 40% IV = 10% Testicular Carcinoma • 5,000 new cases per year • 1,000 deaths per year • Most common solid tumor of young adult men (age 20-40) Pathology • 95% germ cell tumors – – – – – seminoma embryonal cell ca. choriocarcinoma teratocarcinoma yolk sac tumors • 5% interstitial cell tumors (Sertoli, Leydig) Pathology • Rapidly growing tumors • Metastasize early – retroperitoneal, mediastinal LNs – lungs,liver,brain,bones • Tumor markers – beta-HCG – alpha-fetoprotein Staging • T=tumor • T1 = confined to testis • T2 = invades tunica alb. • T3 = invades cord / scrotum • N=lymph nodes • N1 = < 2cm • N2 = 2 - 5 cm • N3 = > 5 cm • M = distant metastasis Signs / Symptoms • Painless testicular mass – considered malignant • virilization, gynecomastia • secondary hydrocele • retroperitoneal mass Treatment • • • • Radical orchiectomy Retroperitoneal lymph node dissection Radiation Chemotherapy All treatments highly effective Survival • Seminoma = 98% • Non-seminoma = 95% Penile cancer • Uncommon in U.S. • Rare in circumcised (at birth) men Pathology • Squamous cell ca. • CIS – Erythroplasia of Queyrat / Bowens disease • Chronic inflammation, phimosis Signs / Symptoms • Penile lesion / mass / ulcer on glans, foreskin, shaft • Secondary infection may co-exist • May be hidden by phimosis • Inguinal lymph nodes Treatment • Excisional bx • Partial vs. total penectomy • Inguinal lymph node dissection • Radiation and chemotherapy have limited efficacy / palliative Survival • Localized (confined to penis) = 80% • Inguinal lymph nodes = 30% • Distant metastasis < 5% Adrenal tumors • • • • • • Cysts Adenomas Myolipomas Adenocarcinomas Pheochromocytomas Aldosteronoma Adrenocortical Ca. • • • • • > 6 cm in size > 50% functional Highly malignant Dx = CT, MRI, serum/urine chemistries Rx – adrenalectomy – mitotane Pheochromocytoma • Hypersecretion of E, NE – htn, palpitations, diaphoresis • 10% are: – malignant, bilateral, extra-adrenal • Dx: CT, MRI, serum/urine chemistries • Rx = surgical excision