Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
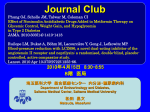
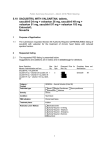
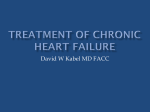
“Out of the Water” An update on emerging heart failure therapies Robert Mohapatra, MD, MPH, FACC September 10, 2016 Disclosures • Honarariums received for participating in speaker programs for Novartis and Amgen Heart Failure – A Growing Global Concern Prevalence and Incidence Overall 2.1% prevalence: 5.1M heart failure patients in 20101 825,000 people ≥ 45 years of age are newly diagnosed each year with HF1 15M heart failure patients in the ESC 51-member countries2 Mortality – For AHA/ACC stage C/D patients diagnosed with HF: • 30% will die in the first year.3-5 • 60% will die within 5 years.5 • Overall 2-3% prevalence2 HF prevalence in the US is projected to increase 46% from 2012 to 2030, resulting in > 8M people ≥ 18 years of age with HF.6 1. 2. 3. 4. 5. 6. AHA 2014 Statistics at a Glance, 2014 The European Society of Cardiology, ESC HF Guideline, 2008 Curtis et al, Arch Intern Med, 2008. Roger et al. JAMA, 2004. Cowie et al, EHJ, 2002. Heidenreich PA et al. Circ Heart Failure 2013. Heart Failure Is Associated with High Hospitalization and Readmission Rates • In 2010, there were 1 million hospitalizations in the US with HF as the principal diagnosis1 – • Average length of hospital stay – – • Hospitalization rate did not change significantly from 20001 Approximately 5 days (US)2 11 days (Europe)3 HF is also associated with high readmission rates: – ~25% all-cause readmission within 30 days and ~50% within 6 months4,5 Graph from www.health.org.uk. Bridging the gap: Heart Failure, 2010. Data from Organization for Economic Cooperation and Development, 2009. 1. 2. 3. 4. 5. CDC NCHS National Hospital Discharge Survey, 2000-2010 Yancy et al. JACC, 2006. Cleland et al. EuroHeart, 2003. Krumholz HM, et al. Circ Cardiovas Qual Outcomes 2009. Wexler DJ, et al. Am Heart J 2001. Economic Burden of HF Will Continue to Rise Through 2030* The AHA estimates that the total medical costs for HF are projected to increase to $70B by 2030 a 2-fold increase from 2013.1 • 50% of the costs are attributed to hospitalization.2 Graph: Heidenreich PA, et al. Circulation Heart Failure 2013. *Study projections assumes HF prevalence remains constant and continuation of current hospitalization practices 1. Heidenreich PA, et al. Circulation Heart Failure 2013. 2. Yancy CW, et al. Circulation 2013. Economic Risks of HF Readmissions in the US Medicare’s Hospital Readmissions Reduction program penalizes hospitals that have above average all-cause readmissions within 30 days following HF discharge. 22.7% national average 30-day readmissions rate1,2 Percent withholding of all inpatient Medicare payments will increase to up to 3% by 2015 and beyond.3 Fiscal Year 2013 2014 2015+ % payment withholding up to 1% up to 2% up to 3% 1. Dharmarajan K, et al. JAMA. 2013;309(4):355-363. 2. Linden A, Adler-Milstein J. Health Care Finance Rev. 2008;29(3):1-11. 3. CMS Hospitals Readmissions Reductions Program of the Patient Protection and Affordable Care Act (PPACA), 2010. Worsening Heart Failure Leading to HF Hospitalizations Contributes to Disease Progression With each subsequent HF-related admission, the patient leaves the hospital with a further decrease in cardiac function. Graph adapted from: Gheorghiade MD, et al. Am J. Cardiol. 2005 Sacubitril/Valsartan ® (Entresto ) HFrEF Pathophysiology The SNS and RAAS Are Overexpressed SNS2,4 Neurohormonal activation via SNS and RAAS signaling may exacerbate the failing heart and trigger lethal ventricular arrhythmias1,2 α1, β1, β2 receptors Epinephrine Norepinephrine HF SYMPTOMS & PROGRESSION Vasoconstriction RAAS activity Heart rate Contractility The RAAS and SNS are overexpressed1,2,4 RAAS2,3,4 Ang II AT1R Vasoconstriction Blood pressure Sympathetic tone Vasopressin Aldosterone Hypertrophy Fibrosis Ang II, angiotensin II; AT1R, angiotensin II type 1 receptor; HF, heart failure; NPs, natriuretic peptides; SNS, sympathetic nervous system; RAAS, renin-angiotensin-aldosterone system. 1. Tomaselli GF, Zipes DP. Circ Res. 2004;95(8):754-763. 2. Kemp CD, Conte JV. Cardiovasc Pathol. 2012;21(5):365-371. 3. Mangiafico S et al. Eur Heart J. 2013;34:886-893. 4. Hasenfuss G, Mann DL. Pathophysiology of heart failure. In: Mann DL et al, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 10th ed. Philadelphia, PA: Elsevier; 2015 9 HFrEF Pathophysiology Role of Endogenous Compensatory Peptides Endogenous Compensatory Peptides (ECPs)2-4 NPR-A, NPR-B, B2, calcitonin receptor-like receptor SNS1,4 NPs, Bradykinin, ADM Vasodilation Blood pressure Sympathetic tone Natriuresis/diuresis Vasopressin Aldosterone Fibrosis Hypertrophy α1, β1, β2 receptors Epinephrine Norepinephrine HF SYMPTOMS & PROGRESSION Vasoconstriction RAAS activity Heart rate Contractility RAAS1,2,4 Ang II The effects of RAAS and SNS are balanced by the counterregulatory effects of ECPs, including NPs, bradykinin, and adrenomedullin2-4 AT1R Vasoconstriction Blood pressure Sympathetic tone Vasopressin Aldosterone Hypertrophy Fibrosis ADM, adrenomedulin; Ang II, angiotensin II; AT1R, angiotensin II type 1 receptor; ECPs, endogenous compensatory peptides; HF, heart failure; NPs, natriuretic peptides; SNS, sympathetic nervous system; RAAS, renin-angiotensin-aldosterone system. 1. Kemp CD, Conte JV. Cardiovasc Pathol. 2012;21(5):365-371. 2. Mangiafico S et al. Eur Heart J. 2013;34:886-893. 3. Nathisuwan S, Talbert RL. Pharmacotherapy. 2002;22:27-42. 4. Hasenfuss G, Mann DL. Pathophysiology of heart failure. In: Mann DL et al, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 10th ed. Philadelphia, PA: Elsevier; 2015. 10 HFrEF Pathophysiology Existing Therapies Endogenous Compensatory Peptides2-4 NPR-A, NPR-B, B2, calcitonin receptor-like receptor α1, β1, β2 receptors Epinephrine Norepinephrine NPs, Bradykinin, ADM Vasodilation Blood pressure Sympathetic tone Natriuresis/diuresis Vasopressin Aldosterone Fibrosis Hypertrophy 1,4 1 SNS SNS β-blockers5 Vasoconstriction RAAS activity Heart rate Contractility HF SYMPTOMS & PROGRESSION RAAS inhibitors (ACEI, ARB, MRA)5 1,2,4 1,22,4 RAAS RAAS RAAS Ang IIII AT1R Vasoconstriction Blood pressure Sympathetic tone Vasopressin Aldosterone Hypertrophy Fibrosis ACEI, angiotensin-converting enzyme inhibitor; ADM, adrenomedulin; Ang II, angiotensin II; ARB, angiotensin II receptor blocker; AT1R, angiotensin II type 1 receptor; ECPs, endogenous compensatory peptides; HF, heart failure; MRA, mineralocorticoid receptor antagonists; NPs, natriuretic peptides; SNS, sympathetic nervous system; RAAS, renin-angiotensin-aldosterone system. 1. Kemp CD, Conte JV. Cardiovasc Pathol. 2012;21(5):365-371. 2. Mangiafico S et al. Eur Heart J. 2013;34:886-893. 3. Nathisuwan S, Talbert RL. Pharmacotherapy. 2002;22:27-42. 4. Hasenfuss G, Mann DL. Pathophysiology of heart failure. In: Mann DL et al, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 10th ed. Philadelphia, PA: Elsevier; 2015. 5. Mann DL. Management of Patients with Heart Failure with Reduced Ejection Fraction. In: Mann DL et al, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 10th ed. Philadelphia, PA: Elsevier; 2015 11 Sacubitril/Valsartan Effects of Sacubitril/valsartan in HFrEF Endogenous Compensatory Compensatory Endogenous 2-4 Peptides2-4 Peptides NPR-A, NPR-B, B2, calcitonin receptor-like receptor SNS1,4 Epinephrine Norepinephrine NPs, Bradykinin, Bradykinin, ADM NPs, ADM Vasodilation Vasodilation Blood pressure Blood pressure Sympathetic tone Sympathetic tone Natriuresis/diuresis Natriuresis/diuresis Vasopressin Aldosterone Vasopressin Fibrosis Aldosterone Hypertrophy Fibrosis Hypertrophy + HF SYMPTOMS & PROGRESSION Vasoconstriction RAAS activity Heart rate Contractility 1,2 RAAS 1,2,4 RAAS Enhance the beneficial effects of endogenous compensatory peptides Neprilysin Inhibitor Sacubitril/ valsartan5 α1, β1, β2 receptors Suppress deleterious effects of RAAS ARB Ang II Ang II AT1R AT1R Vasoconstriction Vasoconstriction Blood pressure Blood pressure Sympathetic tone Vasopressin Sympathetic tone Aldosterone Vasopressin Hypertrophy Aldosterone Fibrosis Hypertrophy Fibrosis 1. Kemp CD, Conte JV. Cardiovasc Pathol. 2012;21(5):365-371. 2. Mangiafico S et al. Eur Heart J. 2013;34:886-893. 3. Nathisuwan S, Talbert RL. Pharmacotherapy. 2002;22:27-42. 4. Hasenfuss G, Mann DL. Pathophysiology of heart failure. In: Mann DL et al, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 10th ed. Philadelphia, PA: Elsevier; 2015. 5. Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 12 Sacubitril/Valsartan Components and Indication Sacubitril/valsartan is a combination of a neprilysin inhibitor and an Ang II receptor blocker Neprilysin Inhibitor ARB Sacubitril/valsartan is indicated to reduce the risk of cardiovascular (CV) death and hospitalization for HF in patients with chronic HF (CHF; NYHA class II–IV) with reduced ejection fraction (HFrEF) Sacubitril/valsartan is usually administered in conjunction with other HF therapies, in place of an ACEi or other ARB NYHA, New York Heart Association. Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 13 Sacubitril/Valsartan Effect on BNP and NT-proBNP ⬆ proBNP secretion ⬆ Myocardial wall tension in HF Vasoactive peptidea with cardioprotective effects Sacubitril/ valsartan NT-proBNP BNP Neprilysin Inactive (inert) marker of HF Neprilysin inhibition has no effect on NT-proBNP Sacubitril/Valsartan Increases BNP Levels Inactive fragments BNPs, brain natriuretic peptides; NT-proBNP, N-terminal of the prohormone brain natriuretic peptide. aVasoactive peptides include the NPs (atrial NPs, BNPs, C-type NPs), adrenomedullin, and bradykinin. Modified from Vardeny O et al. Clin Pharmacol Ther. 2013;94:445-448. 14 Sacubitril/Valsartan Patient Selection Patients with • Chronic HFrEF • NYHA Class II – IV PI Indication Statement Sacubitril/valsartan is indicated to reduce the risk of CV death and hospitalization for HF in patients with chronic HFrEF (NYHA class II–IV) Sacubitril/valsartan is usually administered in conjunction with other HF therapies, in place of an ACEI or other ARB Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 15 Sacubitril/Valsartan Contraindications for Use Sacubitril/valsartan is contraindicated: In patients with hypersensitivity to any component In patients with a history of angioedema related to previous ACEI or ARB therapy With concomitant use of ACEIs. It cannot be administered within 36 hours of switching from or to an ACEI With concomitant use of aliskiren in patients with diabetes Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 16 PARADIGM-HF Trial Key Findings PARADIGM-HF Study Design Phase 3 Trial to Examine the Efficacy of Sacubitril/Valsartan vs Enalapril in Patients With HFrEF1,2 N=8442 patients with chronic HF (NYHA class II–IV with LVEF ≤40%) and elevated BNP Single-blind run-in period Double-Blind Randomized Treatment Period Randomization Sac/val 97/103 mg BID Enalaprila 10 mg BID Sac/valb 49/51 mg BID Sac/valb 97/103 mg BID Enalapril 10 mg BID Testing tolerability to target doses of enalapril and sac/val 2 weeks 1–2 weeks 2–4 weeks On top of standard HF therapy, excluding ACEIs and ARBs3 Median duration of follow-up: 27 months A 36 hour washout was required after single blind enalapril run-in and also at end of entresto single blind run-in prior to being randomized Primary outcome: To demonstrate superiority of sacubitril/valsartan over enalapril in reducing composite of death from CV causes or a first hospitalization for HF BID, twice daily; BNP, brain natriuretic peptide; NYHA, New York Heart Association. aEnalapril 5 mg BID for 1–2 weeks followed by enalapril 10 mg BID was an optional starting run-in dose for patients treated with ARBs or with a low dose of ACEI. bDosing in clinical trials was based on the total amount of both components of sac/val; 24/26 mg, 49/51 mg, and 97/103 mg were referred to as 50 mg, 100 mg, and 200 mg, respectively. Sac/val was formerly known as LCZ696 in clinical trials. 1. Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 2. McMurray JJ et al. Eur J Heart Fail. 2013;15(9):1062-1073. 3. McMurray JJ et al. N Engl J Med. 2014;371(11):993-1004. 18 PARADIGM-HF Baseline Characteristics Characteristic* Age, years Female, n (%) Ischemic cardiomyopathy, n (%) LVEF (%) NYHA functional class, n (%) II III SBP, mm Hg Heart rate, BPM NT-proBNP, median, pg/mL (IQR) BNP, median, pg/mL (IQR) History of DM, n (%) Treatments at randomization, n (%) Diuretics Digitalis Beta-blockers MRAs ICD CRT Sac/Val (N=4187) 63.8 ± 11.5 879 (21.0) 2506 (59.9) 29.6 ± 6.1 Enalapril (N=4212) 63.8 ± 11.3 953 (22.6) 2530 (60.1) 29.4 ± 6.3 2998 (71.6) 969 (23.1) 122 ± 15 72 ± 12 1631 (885–3154) 255 (155–474) 1451 (34.7) 2921 (69.3) 1049 (24.9) 121 ± 15 73 ± 12 1594 (886–3305) 251 (153–465) 1456 (34.6) 3363 (80.3) 1223 (29.2) 3899 (93.1) 2271 (54.2) 623 (14.9) 292 (7.0) 3375 (80.1) 1316 (31.2) 3912 (92.9) 2400 (57.0) 620 (14.7) 282 (6.7) BPM, beats per minute; CRT, cardiac resynchronization therapy; ICD, implantable cardioverter-defibrillator; IQR, interquartile range; SBP, systolic blood pressure. *Mean ± standard deviation, unless stated. McMurray JJ et al. N Engl J Med. 2014;371:993-1004. 19 PARADIGM-HF Primary Endpoint: Time to First Occurrence of CV Death or HF Hospitalization The difference in favor of sacubitril/valsartan was seen early in the trial and at each interim analysis Cumulative Probability of the Combined Endpoint of CV Death or HF Hospitalization 1.0 Enalapril 0.6 Sac/val HR: 0.80 (95% CI: 0.73–0.87) P<0.001 20% Relative Risk Reduction 0.4 1117 events 914 events 0.2 0 0 180 360 540 720 900 1080 1260 896 853 249 236 Days Since Randomization No. at risk Sac/val Enalapril 4187 4212 3922 3883 3663 3579 3018 2922 2257 2123 1544 1488 CI, confidence interval; HR, hazard ratio. McMurray JJ et al. N Engl J Med. 2014;371:993-1004. 20 PARADIGM-HF Summary of Key Findings Sac/Val N=4187 n (%) Enalapril N=4212 n (%) HR (95% CI) P Value 914 (21.8) 1117 (26.5) 0.80 (0.73–0.87) <0.0001 CV death as first event 377 (9.0) 459 (10.9) HF hospitalization as first event 537 (12.8) 658 (15.6) CV deathb 558 (13.3) 693 (16.5) 0.80 (0.71–0.89) HF hospitalizations 537 (12.8) 658 (15.6) 0.79 (0.71–0.89) 711 (17.0) 835 (19.8) 0.84 (0.76–0.93) Endpoint Primary composite endpoint of CV death or HF hospitalization Number of patients with eventsa All-cause mortality 0.0009 aAnalyses of the components of the primary composite endpoint were not prospectively planned to be adjusted for multiplicity. subjects who had HF hospitalization prior to death. Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. bIncludes 21 21 PARADIGM Adverse Effects Sac/Val Enalapril N=4203 n (%) N=4229 n (%) Hypotension 18 12 Hyperkalemia 12 14 Cough 9 13 Dizziness 6 5 Renal failure/acute renal failure 5 5 Adverse Reactions Occurring ≥5% In the PARADIGM-HF trial, the incidence of angioedema was 0.1% in both the enalapril and sacubitril/valsartan run-in periods. In the double-blind period, the incidence of angioedema was higher in patients treated with sacubitril/valsartan than enalapril (0.5% and 0.2%, respectively). The incidence of angioedema in Black patients was 2.4% with sacubitril/valsartan and 0.5% with enalapril Orthostasis was reported in 2.1% of patients treated with sacubitril/valsartan compared to 1.1% of patients treated with enalapril during the double-blind period of PARADIGM-HF. Falls were reported in 1.9% of patients treated with sacubitril/valsartan compared to 1.3% of patients treated with enalapril Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 22 2016 ACC/AHA/HFSA Focused Update Pharmacological Treatment for Stage C HFrEF: Recommendations Recommendations for Renin-Angiotensin System Inhibition With ACE Inhibitor or ARB or ARNI COR LOE Recommendations ACE: A ARB: A I ARNI: B-R The clinical strategy of inhibition of the renin-angiotensin system with ACE inhibitors (Level of Evidence: A), OR ARBs (Level of Evidence: A), OR ARNI (Level of Evidence: B-R) in conjunction with evidence-based beta blockers, and aldosterone antagonists in selected patients, is recommended for patients with chronic HFrEF to reduce morbidity and mortality. “In ARNI, an ARB is combined with an inhibitor of neprilysin, an enzyme that degrades natriuretic peptides, bradykinin, adrenomedullin, and other vasoactive peptides. In an RCT that compared the first approved ARNI, valsartan/sacubitril, with enalapril in symptomatic patients with HFrEF tolerating an adequate dose of either ACE inhibitor or ARB, the ARNI reduced the composite endpoint of cardiovascular death or HF hospitalization significantly, by 20%. The benefit was seen to a similar extent for both death and HF hospitalization and was consistent across subgroups. The use of ARNI is associated with the risk of hypotension and renal insufficiency and may lead to angioedema, as well.” ARNI, angiotensin receptor-neprilysin inhibitor Yancy CW, et.al. , 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure, Journal of the American College of Cardiology (2016), doi: 10.1016/ j.jacc.2016.05.011. 2016 ACC/AHA/HFSA Focused Update Pharmacological Treatment for Stage C HFrEF: Recommendations Recommendations for Renin-Angiotensin System Inhibition With ACE Inhibitor or ARB or ARNI (cont’d) COR LOE I ARNI: B-R Recommendations In patients with chronic symptomatic HFrEF NYHA class II or III who tolerate an ACE inhibitor or ARB, replacement by an ARNI is recommended to further reduce morbidity and mortality. “In patients with mild-to-moderate HF (characterized by either [1] mildly elevated natriuretic peptide levels, BNP [B-type natriuretic peptide] >150 pg/mL or NT-proBNP [N-terminal pro-B-type natriuretic peptide] ≥600 pg/mL; or [2] BNP ≥100 pg/mL or NT-proBNP ≥400 pg/mL with a prior hospitalization in the preceding 12 months) who were able to tolerate both a target dose of enalapril (10 mg twice daily) and then subsequently an ARNI (valsartan/sacubitril, 200* mg twice daily, with the ARB component equivalent to valsartan 160 mg), hospitalizations and mortality were significantly decreased with the valsartan/sacubitril compound compared with enalapril.” *Dosing in clinical trials was based on the total amount of both components of sacubitril/valsartan, i.e., 24/26 mg, 49/51 mg, and 97/103 mg were referred to as 50 mg, 100 mg, and 200 mg, respectively. ARNI, angiotensin receptor-neprilysin inhibitor Yancy CW, et.al. , 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure, Journal of the American College of Cardiology (2016), doi: 10.1016/ j.jacc.2016.05.011. Sacubitril/Valsartan Available Dosages Sacubitril/valsartan is available as film-coated tablets for oral administration. It is available in the following dosages: 24 mg of sacubitril and 26 mg of valsartan 49 mg of sacubitril and 51 mg of valsartan 97 mg of sacubitril and 103 mg of valsartan These doses should be utilized when prescribing sacubitril/valsartan.* 24/26 mg 49/51 mg 97/103 mg *In clinical studies sacubitril/valsartan doses were refered to as 50mg, 100mg and 200mg (24/26mg, 49/51mg and 97/103mg), respectively Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 25 Sacubitril/Valsartan Dosing Guidelines1,2 ARB ACEI Choose the initial dose of sacubitril/valsartan* based on current treatment and titrate to the target dose Dosing in clinical trials was based on the total amount of both components of sacubitril/valsartan; 24/26 mg, 49/51 mg, and 97/103 mg were referred to as 50 mg, 100 mg, and 200 mg, respectively Clinicians should use the available doses when prescribing (24/26mg, 49/51mg and 97/103mg) to help avoid errors in dispensing >10 mg of enalapril or therapeutically equivalent doses of another ACEI: • Lisinopril >10 • Ramipril >5 mg ≤10 mg of enalapril or therapeutically equivalent doses of another ACEI: • Lisinopril ≤10 mg • Ramipril ≤5 mg Start sac/val at the recommended dose of 49/51 Stop mg BID ACEI 36 hours before Double the dose after starting Start sac/val at the 2 to 4 weeks to sac/val recommended dose of 49/51 mg BID, as >160 mg of valsartan or therapeutically equivalent doses of another ARB: • Losartan >50 mg • Olmesartan >10 mg ≤160 mg of valsartan or therapeutically equivalent doses of another ARB: • Losartan ≤50 mg • Olmesartan ≤10 mg Not currently taking ACEIs or ARBs 24/26 mg BID tolerated by the patient Start sac/val at the recommended dose of 49/51 mg BID Start sac/val at the recommended dose of 24/26 mg BID Double the dose after 2 to 4 weeks to 49/51 mg BID, as tolerated by the patient Start sac/val at the recommended dose of 24/26 mg BID Double the dose after 2 to 4 weeks to 49/51 mg BID, as tolerated by the patient Double the dose of sac/val after 2 to 4 weeks, as tolerated by the patient, to reach the target maintenance dose of 97/103 mg BID BID, twice daily; sac/val, sacubitril/valsartan. *Sacubitril/valsartan may be taken with or without food. Sacubitril/valsartan is not scored, and should not be broken in half or crushed. 1. Entresto (sacubitril/valsartan) [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; August 2015. 2. Senni M et al. Presented at ESC-HF Congress; May 23, 2015; Seville, Spain. 26 Corlanor ® (Ivabradine) -Has been used in Europe since 2005. -Was initially approved for treatment of Chronic, stable angina, in patients intolerant to beta blockers or for those on beta blockers with resting heart rate greater than 70. -Was approved in Europe for use in Chronic systolic heart failure in 2012. Was approved for use in United States in April 2015 Corlanor® (ivabradine) Indication • Corlanor® is indicated to reduce the risk of hospitalization for worsening heart failure in patients who meet all of the following conditions • Stable, symptomatic chronic heart failure with left ventricular ejection fraction ≤ 35% – In sinus rhythm with resting heart rate ≥ 70 bpm – On maximally tolerated doses of beta-blockers or have a contraindication to beta-blocker use bpm, beats per minute. Corlanor® (ivabradine) Prescribing Information, Amgen. Corlanor ® (Ivabradine, cont’d) • Approved based on SHIFT study which studied the rationale that a higher resting heart rate is associated with a worse prognosis in patients with chronic heart failure • This finding was first seen in retrospective analysis of the CHARM study, which found that higher resting heart rates were associated with higher likelihood of admission for heart failure • Has unique mechanism of action which lowers heart rate without lowering blood pressure Corlanor® (ivabradine) Blocks the HCN Channel in the Sinus Node which Reduces Heart Rate Adapted from: Postea O, et al. Nature Reviews. 2011;10:903-914. Adapted from: DiFrancesco D, et al. Drugs. 2004;64:1757-1765. Corlanor® (ivabradine) Prescribing Information, Amgen. SHIFT Study Corlanor® (ivabradine) Pivotal Study – SHIFT Systolic Heart failure treatment with the If inhibitor ivabradine Trial SHIFT Study SHIFT Study Design Randomized, double-blind, parallel-group study to assess the effect of ivabradine in addition to guidelines-based treatment in 6,558 patients with HF, conducted from October 2006 through March 2010. • Subjects ≥ 18 years • NYHA Class II, III, or IV and in stable condition for ≥ 4 weeks • LVEF ≤ 35% • Optimal stable Standard of Care (SOC) therapy, including maximally tolerated doses of betablockers Randomization • In sinus rhythm and had a resting HR ≥ 70 bpm • Hospitalization for worsening HF within ≤ 12 months 14 day run-in HF, heart failure; HR, heart rate; LVEF, left ventricular ejection fraction. Swedberg K, et al. Lancet. 2010;376:875-885. Ivabradine 5 mg twice daily for 2 weeks (n = 3,268) Ivabradine 7.5/5.0/2.5 mg twice daily according to HR and tolerability* Placebo twice daily (n = 3,290) Median follow-up duration: 22.9 months (interquartile range = 18 to 28 months) SHIFT Study Primary and Secondary Endpoints •Primary Endpoint • Composite of the first occurrence of either CV death or hospital admission for worsening HF CV, cardiovascular. Swedberg K, et al. Lancet. 2010;376:875-885. Corlanor® (ivabradine) Prescribing Information, Amgen. •Secondary Endpoints • CV death (component of the primary composite endpoint) • Hospitalization for worsening HF (component of the primary composite endpoint) SHIFT Study Ivabradine Titration Starting dose 5 mg twice daily Titration Period: D14 & D28 Follow-up Period: Every 4 months < 50 bpm or patient experiencing signs or symptoms related to bradycardia 50 to 60 bpm > 60 bpm 2.5 mg twice daily 5 mg twice daily 7.5 mg twice daily Treatment was discontinued if heart rate remained below 50 bpm or symptoms of bradycardia persisted after dose reduction. D, day. Swedberg K, et al. Lancet. 2010;376:875-885. Corlanor® (ivabradine) Prescribing Information, Amgen. Primary Composite Endpoint Time to First Event of Hospitalization for Worsening HF or CV Death Composite Endpoint (%) Patients With Primary 40 Placebo + SOC (937 events) Hazard Ratio 0.82 95% CI (0.75–0.90) ARR = 4.2% P < 0.0001 30 18% Relative Risk Reduction Ivabradine + SOC (793 events) 20 10 The treatment effect reflected only a reduction in the risk of hospitalization for worsening HF; there was no favorable effect on the mortality component of the primary endpoint. 0 0 6 12 18 Time (months) Primary Composite Endpoint: Time to CV Death or First Hospitalization for Worsening HF. ARR, absolute risk reduction; CI, confidence interval; SOC, standard of care. Corlanor® (ivabradine) Prescribing Information, Amgen. Swedberg K, et al. Lancet. 2010;376:875-885 24 30 36 Secondary Endpoint CV Death at Any Time Patients With CV Death (%) 40 Hazard Ratio 0.91 95% CI (0.80–1.03) ARR = 1.1% In the overall treatment population, Corlanor® had no statistically significant benefit on cardiovascular death 30 Placebo + SOC (491 events) 20 9% Relative Risk Reduction Ivabradine + SOC (449 events) 10 0 0 6 12 18 Time (months) CI, confidence interval; CV, cardiovascular; SOC, standard of care. Swedberg K, et al. Lancet. 2010;376:875-885. 24 30 Secondary Endpoint Hospitalization for Worsening HF at Any Time For Worsening HF (%) Patients With First Hospitalization 40 Hazard Ratio 0.74 95% CI (0.66–0.83) ARR = 4.7% 30 Placebo + SOC (672 events) 26% Relative Risk Reduction 20 Ivabradine + SOC (514 events) 10 0 0 6 12 18 Time (months) Swedberg K, et al. Lancet. 2010;376:875-885. 24 30 Adverse Events Adverse Drug Reactions with Rates ≥ 1.0% Higher on Ivabradine than Placebo Ivabradine N = 3,260 Placebo N = 3,278 Bradycardia 10% 2.2% Hypertension (Blood pressure increased) 8.9% 7.8% Atrial Fibrillation 8.3% 6.6% Phosphenes (Visual brightness) 2.8% 0.5% Adverse Events Corlanor® (ivabradine) Prescribing Information, Amgen. Ivabradine, summary SHIFT study showed beneficial effect on HF hospitalization, but not mortality Benefits were greater in those intolerant/on low doses of beta blockers along with those with higher resting heart rates 2016 Updated ACC/AHA/HFSA guidelines: Class IIa recommendation Ivabradine can be beneficial to reduce HF hospitalization for patients with: symptomatic (NYHA class II-III) stable chronic HFrEF (LVEF ≤35%) who are receiving GDMT, including a beta blocker at maximum tolerated dose who are in sinus rhythm with a heart rate of 70 bpm or greater at rest CardioMEMS™ HF System Pulmonary Artery Pressure Sensor Patient Electronics System CardioMEMS™ HF System Website Time Course of Decompensation Physiologic Markers of Acute Decompensation Graph adapted from Adamson PB, et al. Curr Heart Fail Reports, 2009. CardioMEMS™ HF System The pulmonary artery pressure sensor is implanted via a right heart catheterization procedure via femoral vein approach. Target location for pulmonary artery pressure sensor CardioMEMS™ HF System The pulmonary artery pressure sensor is implanted via a right heart catheterization procedure via femoral vein approach. Target location for pulmonary artery pressure sensor CHAMPION Clinical Trial: The Effect of Pulmonary Artery PressureGuided Therapy on HF Hospitalizations vs. Standard of Care Patients with moderate NYHA class III HF for at least 3 months, irrespective of LVEF and a HF hospitalization within the past 12 months were included in the study. 550 Pts with CardioMEMS™ HF System Implants All Pts Take Daily readings Treatment 270 Pts Management Based on PA Pressure +Traditional Info 26 (9.6%) Exited < 6 Months 15 (5.6%) Death 11 (4.0%) Other Abraham WT, et al. Lancet, 2011. Control 280 Pts Management Based on Traditional Info Primary Endpoint: Rate of HF Hospitalization Secondary Endpoints: Change in PA Pressure at 6 months No. of patients admitted to hospital for HF Days alive outside of hospital QOL 26 (9.6%) Exited < 6 Months 20 (7.1%) Death 6 (2.2%) Other CHAMPION Clinical Trial Patients managed with PA pressure data had significantly fewer HF hospitalizations as compared to the control group. Abraham WT, et al. Lancet, 2011. CHAMPION CLINICAL Trial: Both Primary Safety Endpoints and All Secondary Endpoints Were Met at 6 months Primary Safety Endpoints Device-related or system-related complications Pressure-sensor failures Control (n = 280) 3 (1%) 3 (1%) Total 8 (1%)* P-value < 0.0001 0 0 < 0.0001 -156 33 0.008 Number and proportion of patients hospitalized for HF (%) 55 (20%) 80 (29%) 0.03 Days alive and out of hospital for HF (mean ± SD) 174.4 ± 31.1 172.1 ± 37.8 0.02 Quality of life (Minnesota Living with Heart Failure Questionnaire, mean ± SD) 45 ± 26 51±25 0.02 Change from baseline in PA mean pressure (mean AUC [mm Hg x days]) Secondary Endpoints Treatment (n = 270) * Total of 8 DSRCs including 2 events in Consented not implanted patients (n = 25) Abraham WT, et al. Lancet, 2011. Cardiomems ™ approval • Approved by the FDA in May, 2014 for the indication of reduction of heart failure hospitalization • Indication for implantation is NYHA class III heart failure and hospitalization for CHF within last year LCS experience with Cardiomems ™ • 11 patients have been implanted thus far • One patient has been admitted to the hospital with HF Insurance Coverage • Novitas, which contracts with Medicare to determine local coverage, declined to reimburse Cardiomems ™ in February of 2016 • Select private insurers have continued to reimburse Cardiomems ™ • A national decision from CMS is expected by the end of the year Telehealth • What is Telehealth? – The use of digital /communication technology to provide healthcare – Examples of telehealth include phone calls, use of media such as tablets to transmit vital signs including weight, BP, HR, and O2 saturation – ECG’s can be transmitted with some telehealth programs – Other telehealth programs utilize video conferencing Telehealth • There have been dozens of studies which have examined different approaches using telehealth with HF patients • A meta analysis published in 2015 reviewing 41 randomized trials found minimal benefit in reduction of HF admissions (8% relative risk reduction, NNT to prevent HF admission was 52) (Ann Fam Med 2015:13:6 562-571) TELE-HF Trial: Telemonitoring of Weight and Symptoms Do Not Reduce Readmission or Death • Randomized study of 1653 patients • Primary endpoint: Readmission for any reason or death from any cause within 180 days after enrollment • Control group = Standard-of-care (no telemonitoring) • Treatment group = telemonitoring of symptoms and weight • Results: No difference in number of deaths, readmissions or days in hospital p = 0.39 60 % of Patients 50 Telemonitoring of Symptoms and Weight group 40 30 p = 0.86 20 10 0 Re-hospitalization Chaudhry SI, et al. N Engl J Med, 2010. Death Standard-of-care Group TIM-HF Trial: Telemonitoring of Weight and Blood Pressure Do Not Reduce Readmission or Mortality • Randomized study of 710 patients • Primary Endpoint: Total Mortality • Control Group: Standard-of-care (no telemonitoring) • Treatment Group: Telemonitoring of weight and BP information • Results: No difference in all-cause death or HF hospitalizations Telemonitoring n = 354 (%) Usual care n = 356 (%) HR (95% CI) p All-cause mortality 15.3 15.4 0.97 (0.67-1.41) 0.87 Cardiovascular-related mortality 11.3 12.9 0.86 (0.56-1.31) 0.49 54.2 50.3 1.12 (0.91-1.37) 0.29 End Point Koehler F et al, Circulation 2011 All-cause readmission Cardio-oncology • Emerging field in cardiology which pertains to the cardiovascular effects of chemotherapy and radiation treatments on cancer patients • Utilizes techniques such as strain imaging with echocardiography which can help identify patients that are at risk