Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Specialty drugs in the United States wikipedia , lookup
Compounding wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Orphan drug wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmacognosy wikipedia , lookup
Psychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
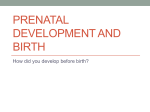
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Review of Terms ■Pharmacokinetics: … definition of each? —Absorption —Distribution —Metabolism —Excretion ■ Pharmacokinetic processes ■ Determine the concentration of a drug at its site(s) of action. ■ The concentration of drug at its sites of action determines the intensity and duration of the response. — MPinson_wi_16 1 Review of Terms ■ Molecule characteristics that allow molecules to cross membranes more readily ■ Small, uncharged, lipid-soluble, non-protein bound ■ These characteristics influence how readily a drug crosses membranes and can be transferred into specific compartments ■ such as crossing into the placenta, entering the fetus ■ or crossing the blood-brain barrier (BBB) and entering the CNS ■ Or crossing into breastmilk and being ingested by baby MPinson_wi_16 2 Drug Therapy during Pregnancy and Breast-Feeding Drug Therapy during Pregnancy and Breast-Feeding Clinical Goal: Provide effective treatment for mother while avoiding harm to fetus and/or nursing infant Clinical Challenge: How to provide safe and effective treatment when there is limited data on drug use during pregnancy and breast-feeding? Clinical Rule; Avoid unnecessary drugs during pg/BF, but all drug therapy cannot and should not be avoided Limited research data on drugs during pregnancy and breast-feeding • Women of reproductive age, infants and children were historically excluded from drug research trials in order to protect them from harm. • This resulted in decades of data-gathering on other populations (men) that then had to be “translated” or “extrapolated” to women/children with unique physiologic considerations. • In the 1990’s, FDA issued a series of guidelines mandating participation of women (and minorities) in new drug trials.FDA can now mandate that drug companies conduct research trials that include children. 5 • Patient registries- AHU p 78 Medication use during pregnancy is common • Meds may be used to treat/manage – Pregnancy-related conditions or complications – Chronic disorders – New diagnoses that arise: eg infections (UTI, STI); cancer; exacerbations/flares of certain conditions – Much too commonly, drugs of abuse continue to be used during pg, although many drug-using women choose not to breastfeed. • Certain chronic conditions may be (are) far more dangerous to the fetus than the drug(s) used to control the chronic condition • Conditions that threaten the mother’s health may well impact the fetus/baby as well • Uncontrolled asthma doubles the incidence of stillbirth among women with asthma who did not take medications to control 6 asthma Certain conditions or factors that might pose significant risks to the woman and/or fetus. • • • • • • • • Asthma Advanced maternal age lifestyle choices Anemia/ blood disorder Mother’s personal medical history Diabetes Mother’s family history Epilepsy Hypertension infection pre-existing obesity underlying mental health conditions http://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregcomplications.htm 7 http://contemporaryobgyn.modernmedicine.com/contemporary-obgyn/news/sickle-celldisease-pregnancy?page=full Basic approach to drug therapy during Pregnancy and Breast-Feeding ● Decide: should mother’s health condition be managed with medications or not? Risk vs benefit ● Rule: Avoid drug therapy when reasonably appropriate: is it safe for mom to go without meds? ● Use non-pharmacological measures to promote health when applicable/ appropriate: nutrition/ fiber/ water, physical activity, sleep, emotional support, physical assistance, etc ● If drug therapy is indicated, then choose the drug/ regimen with the least risk of causing harm ● Some conditions may require temporary use of a “lowest risk” med during pg/BF, then mother can resume use of a different 8 med after pg/BF if desired Physiologic changes during pregnancy impact pharmacokinetics. Dose adjustments of maternal medications may be necessary. • Blood volume: By the third trimester, blood volume doubles, thereby reducing the plasma concentration of drug. • RBF: By the third trimester, renal blood flow doubles, thereby more rapidly eliminating renal-excreted drugs. • Liver: For some drugs, hepatic metabolism increases (enzyme induction), thereby decreasing amount of drug. • Bowel: Tone & motility decrease, thereby prolonging transit time. Increased time in the bowel allows greater drug absorption and enterohepatic cycling to occur. 9 Placental drug transfer • Essentially, all drugs can cross the placenta, but the degree to which specific drugs enter the placenta varies • Factors that determine drug passage into the placenta are the same factors that determine drug passage across all other membranes • Drugs that cross membranes easily will enter the placenta most readily = Lipid-soluble • Drugs that do not cross membranes easily enter the placenta least readily = Ionized, highly polar, proteinbound, or super LARGE molecules do not cross as readily • For practical purposes, assume that any drug taken 10 during pregnancy will reach the fetus Drug-related Adverse Effects during pregnancy 1- Pregnant women are subject to the same adverse effects as non-pregnant women 2- The physiologic state of being pregnant may itself impose additional issues for mother – Ex: Body-habitus, nutrient issues, etc – Ex: heparin can cause osteoporosis. In pregnant women, heparin may lead to vertebral compression fractures 3- Potential adverse effects to: ● Reproductive structures (uterus, cervix, placenta) ● Fetus (organogenesis, functional development) 11 Potential impact of drugs on fetal growth and development • Teratogen = a medicine or other chemical capable of producing a permanent structural or functional birth defect, growth impairment, or fetal death • Teratogenesis = the process by which congenital malformations are produced in an embryo or fetus − greatest concern for many 12 Causes of birth anomalies • About 25% - genetic factors • Less than 1%- drugs • Significant but unknown %- environmental chemicals • Vast majority of birth defects have unidentified causes 13 Effects of teratogens at various stages of fetal development ** Not all exposures to teratogens result in congenital anomalies. The specific chemical/ drug to which the fetus is exposed is of prime importance. However, the amount of chemical/ dose, frequency, duration, and fetal stage of development, (and other variables) are additional contributing factors that cumulatively determine degree of impact. Some teratogens quickly cause damage, whereas others require prolonged exposure. Stage of Fetal Development Effects of Teratogen Exposure Preimplantation conception – week 2 “All or nothing” Embryonic period week 3 – week 8 Gross malformations, anatomic abnormalities Fetal period 14 Effects are usually functional Teratogenesis and Stage of Development Preimplantation Embryonic Period Fetal Period Figure 9-1 Effects of teratogens at various stages of development of the fetus. (From Moore KL: The 15 Developing Human: Clinically Oriented Embryology, 5th ed. Philadelphia: WB Saunders Company, 1993. With permission.) FDA pregnancy risk categories The FDA established five categories (A, B, C, D, and X) to indicate a drug's probable risk to the fetus (1979). A - Controlled studies in women fail to demonstrate a risk to the fetus in the first trimester, and the possibility of fetal harm appears remote. B - Animal studies do not indicate a risk to the fetus and there are no controlled human studies, or animal studies do show an adverse effect on the fetus but well-controlled studies in pregnant women have failed to demonstrate a risk to the fetus. C - Studies have’ shown that the drug exerts animal teratogenic or embryocidal effects, but there are no controlled studies in women, or no studies are available in either animals or women. D - Positive evidence of human fetal risk exists, but benefits in certain situations (e.g., life-threatening situations or serious diseases for which safer drugs cannot be used or are ineffective) may make use of the drug acceptable despite its risks. X - Studies in animals or humans have demonstrated fetal abnormalities or there is evidence of fetal risk based on human experience, or both, and the risk 16 dearly outweighs any possible benefit. * This organizational schema is likely to be replaced by one that provides more detailed information. Drugs that Should Be Avoided during pregnancy because of proven or strongly suspected teratogenicity. Drugs to avoid- aspirin, ibuprofen on frequent basis Drugs of choice – acetaminophen, but not too excessively Table 9-1 (p 84) 17 Drug Therapy During Breast-Feeding 18 Drug Therapy During Breast-Feeding • Nearly all drugs can enter breast milk, but the extent of drug entry into breast milk varies greatly – Drugs that readily cross membranes will readily enter breast milk • “Fortunately, there are relatively few instances in which drugs secreted into breast milk have been found to cause injury to patients”… • …For the few drugs that are absolutely contraindicated during lactation, equally effective and safer medications are usually available” (Adams, Holland & Urban, 2014, p 79.) • If drug concentrations are high enough, the baby will experience a physiologic/pharmacologic effect, raising the possibility of harm • Very little systematic research has been collected in the US 19 • Data coming from Europe Principles of Drug Therapy During Breastfeeding • Is the drug therapy necessary? • What is the safest option for the infant? • If there is the possibility of harm, monitor infant blood levels of the drug. • Minimize infant exposure. – American Academy of Pediatrics 20 Strategies to minimize infant exposure to drug • Postpone pharmacotherapy until the baby is weaned if possible; use nonpharm strategies when possible. • Although most maternal medications probably pose no harm to the breastfeeding infant, their effects have not been fully studied. • If drug needs to be used: – If possible, Mom should take the medication immediately AFTER feeding the baby… to reduce (if possible) the amount of drug in the breast milk – Avoid breast-feeding during peak effect – Avoid drugs with long half-life (or active metabolites) – Drugs that are highly protein-bound are preferred – Use caution if baby is severely ill; a neonate; or preterm. They may not have adequate drug metabolizing 21 enzymes Drugs Associated with Serious Adverse Effects During Breast-Feeding • Insert Table p 80, AHU • And lehne p 86 • Immune suppressants ( e.g., cyclosporine. methotrexate) • Amiodarone & antithyroid drugs • Benzodiazepines, anticonvulsants, antihistamine – watch for sedation • Caffeine – high infant exposure = irritability • All drugs of abuse, controlled substances 22 Resources for further Learning: Drugs • Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk, 10th edition by Gerald G. Briggs BPharm, FCCP, and Roger K. Freeman MD • www.hsl.uw.edu • Introduction to 9th edition was written by Sumner J. Yaffe, MD: excellent, profound eye-opener. 23 Resources for further Learning: Herbs • HERBS TO BE AVOIDED DURING LACTATION Two popular herbal remedies for nursing mothers fenugreek and comfrey - can pose a health risk to their infants. Women advised to avoid fenugreek, but comfrey is much more dangerous and is banned in Canada. • Nursing mothers should be steered away from most herbs, but there are some teas. Chicory, peppermint, orange spice and red bush tea are all fine. Rose hips is an especially good tea because it has a very high concentration of vitamin C. • www.micromedexsolutions.com 24 Drug Therapy in Pediatric Patients NURS 310 Winter 2016 MPinson_wi_16 25 Drug Therapy in Pediatric Patients • Infants/children have largely been excluded from drug research trials since the 1960’s. As a result, inadequate data currently exists for prescribers to ensure safe dosing for infants/children. Two thirds of drugs used in pediatrics have never been tested in pediatric patients • • Best Pharmaceuticals for Children Act (2002) Pediatric Research Equity Act of 2003 • After these laws were enacted, early studies indicated- • 20 % of drugs were ineffective for children (even though they were effective for adults) • 30 % of drugs caused unanticipated side effects, some of which were potentially lethal • 20 % of drugs required dosages different from those that had been extrapolated from dosages used in adults • These laws were permanently reauthorized as part of the FDA Safety and Innovation Act (FDASIA) of 2012 MPinson_wi_16 26 Pharmacokinetics: Comparison between Infants and Adults- Clearly, children are not little adults Figure 10-1: Drug doses adjusted to body weight were administered to infants and adults, via IV injection (left) or subcut (right). Duration/time above MEC, and peak drug levels, differed significantly between infants and adults. Therefore, adjusting dose MPinson_wi_16 amounts based on body size alone is inadequate to safely medicate neonates and infants. Drug Therapy in Pediatric Patients Pediatric patients respond differently to drugs than adults. Most of these differences are quantitative. — Neonates/infants are more sensitive to drugs than adults Heightened sensitivity is due mainly to organ system immaturity — Neonates/infants are at increased risk for adverse drug reactions — Young patients show greater individual variation MPinson_wi_16 28 Pharmacokinetics in Neonates and Infants: ABSORPTION ● Absorption – Oral administration • Gastric emptying time – Prolonged and irregular – Adult function at 6 to 8 months • Gastric acidity – Very low 24 hours after birth – Does not reach adult values until age 2 years – Low acidity: Absorption of acid-labile drugs is increased – Intramuscular administration • During the first few days of life: Slow, Erratic, Delayed absorption as a result of low blood flow • During early infancy, absorption of intramuscular drugs more rapid than in neonates and adults – Transdermal absorption • • • • Stratum corneum of infant’s skin is very thin Blood flow to skin greater in infants than in older patients More rapid and complete for infants than for older children and adults Infants at increased risk of toxicity from topical drugs 29 Pharmacokinetics in Neonates and Infants: DISTRIBUTION ● Distribution – Protein binding • Binding of drugs to albumin and other plasma proteins is limited in the infant • Amount of serum albumin is relatively low • Consequence? _______________ – Blood-brain barrier • Not fully developed at birth • Drugs and other chemicals have relatively easy access to the CNS • Infants especially sensitive to drugs that affect CNS function • Dosage should also be reduced for drugs used for actions outside the CNS if those drugs are capable of producing CNS toxicity as a side effect – Endogenous compounds compete with drugs for available binding sites • Limited drug/protein binding in infants • Reduced dosage needed • Adult protein binding capacity by 10 to 12 months of age 30 Pharmacokinetics in Neonates and Infants: METABOLISM • Hepatic metabolism – The drug-metabolizing capacity of newborns is low – Neonates are especially sensitive to drugs that are eliminated primarily by hepatic metabolism – The liver’s capacity to metabolize many drugs increases rapidly about 1 month after birth – The ability to metabolize drugs at the adult level is reached a few months later – Complete liver maturation occurs by 1 year of age 31 Pharmacokinetics in Neonates and Infants: EXCRETION • Renal excretion – Significantly reduced at birth – Low renal blood flow, low glomerular filtration, and low active tubular secretion – Drugs eliminated primarily by renal excretion must be given in reduced dosage and/or at longer dosing intervals – Adult levels of renal function achieved by 1 year 32 Drug Therapy in Pediatric Patients: Pharmacokinetics in Neonates and Infants: consequences • Neonates and infants are more sensitive to drugs (than adults) primarily due to organ system immaturity. • Elevated drug levels = more intense response • Delayed elimination = prolonged response • Immaturity of organs puts patient at risk for both of these responses • And increases the risk of adverse effects • Most pharmacokinetic parameters are similar to those of adults by the age of 1 year 33 Rationale & Examples of Adverse Drug Reactions • Neonates/infants are vulnerable to unique adverse effects related to organ immaturity – Fewer albumin proteins greater concentrations of free drug – Elevated free drug levels more intense response – Decreased hepatic metabolism prolonged response – Decreased renal elimination prolonged response – Blood-brain-barrier not well-formed CNS effects 34 Drug Therapy in Pediatric Patients Pharmacokinetics: Children Aged 1 Year and Older MPinson_wi_16 35 Drug Therapy in Pediatric Patients Pharmacokinetics in Children Age 1 Year and Older • By the age of 1 year, most pharmacokinetic parameters in children are similar to those of adults • In children age 1 year and older, drug sensitivity is more like that of adults • One important difference: rate of metabolism varies. Children between the ages of 1 and 12 years metabolize drugs faster than adults. – Beginning ~ age 1 year, metabolism is markedly faster than adults until the baby reaches age of 2 years, then a gradual decline… – Sharp decline at puberty – May need to increase dosage or decrease interval between doses accordingly 36 Rationale & Examples of Adverse Drug Reactions • Examples of age-related adverse drug reactions: • Growth suppression (caused by glucocorticoids) • Discoloration of developing teeth (tetracyclines) • Kernicterus (sulfonamides) 37 Drug Therapy in Pediatric Patients Dose approximation based on body surface area MPinson_wi_16 38 Drug Therapy in Pediatric Patients: Dosage Determination • Pediatric doses have been established for a few drugs, but not most drugs • Dosing is most commonly based on body surface area (BSA) – Initial pediatric dosing is, at best, an approximation • Nurses must be able to determine if a prescribed pediatric dose is within a safe range – Compare the patient’s prescribed dose to the recommended safe dose as found in a reputable drug reference • After an initial dose, pt must be monitored carefully for possible adverse effects • Subsequent doses must be adjusted on the basis of clinical response/ outcome and plasma drug concentrations • Dose adjustments are especially important in neonates and younger infants MPinson_wi_16 39 Drug Therapy in Pediatric Patients: Dosage Determination Approximate dosage for a child = Body surface area of the child × adult dose 1.73 m² MPinson_wi_16 40 Drug Therapy in Pediatric Patients: IV hydration rates IS YOUR PATIENT GETTING ADEQUATE HYDRATION? ????????????? MPinson_wi_16 41 Drug Therapy in Pediatric Patients: Promoting Adherence to a Medication Regimen • Effective two-way communication, and individualized patient education, are critical to promoting adherence to a drug therapy. • Provide patient education in several ways, and always in writing as well. Verbal, infomercial, class, etc. • Demonstration techniques should be included when/if appropriate • “Teach Back” MPinson_wi_16 42 Drug Therapy in Pediatric Patients: Promoting Adherence to a Medication Regimen Patient/ caregiver/ family need to know: • Name of medication, and its purpose • Dosage size and timing (r/t meals, other meds, time of day, symptom onset, and so forth) • Administration route and technique • Special considerations • Treatment duration • Drug storage- safety for children in household • Nature and time course of desired responses • Nature and time course of adverse effectsteach possible adverse effects, how to respond, when and how to follow-up with provider, and when to call 911 MPinson_wi_16 43 Drug Therapy in Geriatric Patients Age-related physiologic changes Individuals do not “age” uniformly at the same rate Rate of aging and effects on physiology vary “Biologic age” may not match “chronologic age” Rate of change dependent on “lifelong health” Genetic makeup Lifestyle Health status − presence or absence of disease, injury) Cardiovascular fitness Demographics r/t drug use in the aging population: Disproportionate drug use • Drug use among adults age 65 years or older is disproportionately high •Represent 13% of current US population •Consumers of 33% of prescription drugs •Consumers of 40% of OTC drugs • Ambulatory older adults use 2 to 4 prescription drugs regularly • Long-term care residents use an average of 7-8 medications (Tindall, Sedrak & Boltri, 2014) Demographics r/t drug use in the aging population: polypharmacy & associated risks Greater prevalence in older adults due to increased prevalence and/or severity of disease Drugs to manage disease(s) Drugs to manage symptoms (of disease or aging) Drugs to treat side effects of other drugs Multiple prescribers, excessive prescribing Multiple pharmacies Drug advertising (…pills to cure all…stay young..) Older adult patients experience more adverse drug reactions and drug-drug interactions than younger patients do Age-related physiologic changes pose unique considerations to geriatrics Age-related changes COMBINE with diseaserelated changes to impact pharmacokinetics and pharmacodynamics Most commonly, effects of drugs are increased in older adults Older adults are “more sensitive” to drugs than younger adults However, effects of some drugs may be decreased (eg beta blockers) Older adults show wider individual variation in responses 48 Age-related physiologic changes Age and/or disease- related physiologic changes • profoundly affect pharmacokinetics • whereas pharmacodynamic effects not understood • Which pharmacokinetic change is responsible for most ADRs in older adults? → Reduced renal excretion • Age-related Physiologic changes: gastrointestinal changes affect pharmacokinetics r/t absorption Age-related changes to GI tract Reduced GI blood flow Reduced motility Atrophy of mucosa and glands Reduces digestive secretions Decrease in number of absorptive cells; decreased absorptive surface area gastric acid production may be unchanged or reduced (ie increased pH) delayed gastric emptying Effect on pharmacokinetics The rate of absorption may slow with age, but overall percentage (amount) absorbed from an oral med does not change with age Age-related Physiologic changes: body composition changes affect pharmacokinetics r/t distribution Body composition/ other changes & volume of distribution Decreased percentage of lean body mass Increased percentage of body fat Storage depot for lipid-soluble drugs Increased half-life of fat-soluble drugs Decreased total body water Increases serum concentration of water soluble drugs; effects more intense Reduced concentration of plasma proteins (especially serum albumin) Reduced protein binding of drugs and increased levels of free drug In some people, albumin levels and “physiologic reserve” may be significantly reduced and depleted 51 Age-related Physiologic changes: hepatic changes affect pharmacokinetics r/t hepatic metabolism Age-related changes to liver —reduced hepatic blood flow —reduced liver mass —decreased activity of some hepatic enzymes occurs Hepatic metabolism declines with age Age – related changes combine with effects of concomitant disease or social impacts such as decreased nutritional status Half-lives of some drugs may increase, responses may b prolonged Responses to some oral drugs may be enhanced (eg drugs that undergo extensive first-pass effect) Age-related Physiologic changes: renal changes affect pharmacokinetics r/t renal excretion Age-related changes to kidney: Renal function undergoes progressive decline beginning in early adulthood: Reduction in number of functional nephrons, Decreased glomerular filtration rate, Decreased active tubular secretion; Diminished ability to adapt to changes in electrolyte, acid levels Reduction in renal blood flow, decreased renal excretion Drug accumulation as a result of reduced renal excretion is the most important cause of adverse drug reactions, drug-drug interactions, and may lead to toxicity in older adults 53 Age-related Physiologic changes: Assessment of Renal Function Renal function should be assessed for all pts taking drugs that are eliminated primarily by the kidneys In older adults: Use creatinine clearance to assess renal function (rather than serum creatinine), because lean muscle mass (source of creatinine) declines in parallel with kidney function Creatinine levels may be normal even though kidney function is greatly reduced 54 Age-related Physiologic changes: Assessment of Renal Function, cont’d • Cockcroft – Gault Equation is adequate for most adult patients with normal muscle mass and serum creatinine (Scr) < 4.5 mg/dL Creatinine = clearance (ml/min) _140 - age in yrs x weight in kg _ 72 x serum creatinine (% mg/100mL (for women, multiply result by .85) Age-related Physiologic changes: Assessment of Renal Function: example of Cockcroft– Gault Equation 80 year old male weighs 72 40 year old male kg weighs 72 kg Yearskg cr cl = (140 - 40) 72 72 (1.0) (140 - 80) 72 cr cl = 72 (1.0) Serum Creatinine cr cl = 100 ml/min cr cl = 60 ml/min * To estimate cr cl in women, multiply result by .85 Age-related physiologic changes impact pharmacodynamics Alterations in receptor properties may underlie altered sensitivity to some drugs. Examples: Some drugs have more intense effects in older adults Warfarin and certain central nervous system depressants → possibly due to increases in number of receptors, affinity or both Beta blockers are less effective in older adults, even in the same concentrations → possible reduction in number of beta receptors , affinity of beta receptors for beta-receptor blocking agents, or both 57 Adverse drug reactions and drug-drug interactions are HIGH in older adult population: Predisposing Factors that increase rate of ADR Drug accumulation secondary to reduced renal function is the most important cause of adverse drug reactions and drug-drug interactions in older adults Polypharmacy Greater severity of illness Multiple pathologies Greater use of drugs that have a low therapeutic index (for example, digoxin) Increased individual variations secondary to altered pharmacokinetics Inadequate supervision of long-term therapy Poor patient adherence 58 Drug Therapy in Geriatric Patients: Examples of ADE/ ADR May be undetected in older adults because they can mimic characteristics of problems, disease, or symptoms commonly present in the elderly Symptoms of ADR in older adults are often nonspecific Examples: −Oversedation −Cognitive changes such as confusion −Dizziness −Hallucinations −Accidents/ Falls −Bleeding −and other unwanted, uncomfortable, or dangerous effects How can the nurse decrease incidence of adverse drug reactions and drug-drug interactions based on altered pharmacoKINETICS? Identify the organs involved Monitor organ functioning Liver- PT/INR good indicators of hepatic function AST, ALT are markers for hepatic inflammation Ammonia albumin Kidneys – creatinine clearance Assess for symptoms that suggest a decline in organ function Assess for desired and adverse responses to the drug How can the nurse decrease the incidence of adverse drug reactions and drug-drug interactions based on altered pharmacodynamics? Differences in receptor number and binding = UNPREDICTABLE Assess for desired and adverse responses to the drug Use caution with drugs that can have serious adverse effects, especially with low therapeutic index drugs Use less toxic analgesics first (e.g., acetaminophen versus NSAID) Watch for delayed signs of drug-related toxicity Start with low doses of meds… titrate up as needed at appropriately spaced time intervals, carefully monitoring for effect Remember: it takes between 4 – 5 doses of meds administered at properly spaced/timed intervals (r/t half-lif to achieve plateau Start low . . . . Go slow!