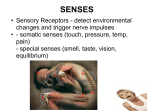
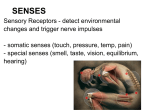
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Telecommunications relay service wikipedia , lookup
Auditory processing disorder wikipedia , lookup
Olivocochlear system wikipedia , lookup
Sound localization wikipedia , lookup
Lip reading wikipedia , lookup
Hearing loss wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Auditory system wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
James Zeigler Au.D. Thank You Protocol for screening and evaluating hearing loss in infants and young children Conductive and sensorineural hearing losses Amount of hearing loss Audiogram overview Hearing Tests - abr and sound booth tests Hearing Aids JCIH 2007 www.jcih.org Early Hearing Detection and Intervention (EHDI): What is it? Hearing loss is the most common disorder screened in the newborn period and one of the most cost effective to treat EHDI is an integrated system that brings multiple disciplines together for the single purpose of detecting and treating hearing loss as early in life as possible There must be a seamless integration of universal newborn screening, prompt diagnosis, effective intervention and tracking. EHDI Program Goals • Screen all newborns by 1 month of age • Diagnose hearing loss by 3 months of age • Link the child to intervention by 6 months of age to maximize developmental, educational and communication outcomes • Provide support and education for families about the importance of detection and treatment of newborn hearing loss Remember!! 1 - 3 - 6 Why the rush?? Anu Sharma Ph.D. Cortical Auditory Potentials Boys Town National Research Hospital Study of Earlier vs. Later 129 deaf and hard-of-hearing children assessed 2x each year 6 Identified <6 mos (n = 25) Identified >6 mos (n = 104) Language Age (yrs) 5 4 3 2 1 0 0.8 1.2 1.8 2.2 2.8 Age (yrs) 3.2 3.8 Moeller, M.P. (1997). Personal communication , [email protected] 4.2 4.8 Anatomy and Physiology Anatomy and Physiology of Hearing Divided into 4 parts Outer Ear Middle Ear Inner Ear Central Auditory Nervous System Structures of the Outer Ear Pinna Gathers sound waves Aids in localization Structures of the Outer Ear External Auditory Canal or Ear Canal Approx. 1 inch long “S” shaped Amplifies sound by 3 to 6 dB Isolates the eardrum from physical damage Cerumen glands moisten/soften skin Presence of some cerumen is normal Structures of the Outer Ear Tympanic Membrane or Ear Drum Thin membrane Forms boundary between outer and middle ear Vibrates in response to sound waves Changes acoustical energy into mechanical energy Structures of the Middle Ear Ossicles Ossicular chain = malleus, incus & stapes Focus/amplify vibration of TM to smaller area Enables vibration of cochlear fluids Malleus = Hammer Attaches to TM Incus = Anvil Connector Stapes = Stirrup Smallest bone in the body Footplate inserts in oval window of the cochlea Structures of the Middle Ear Eustachian Tube Connects middle ear cavity to nasopharynx “Equalizes” air pressure in middle ear Normally closed, opens under certain conditions May allow a pathway for infection Children “grow out of” most middle ear problems as this tube lengthens and becomes more vertical PKS and high arch palate? Structures of the Inner Ear Cochlea Snail shaped cavity within mastoid bone 2 ½ turns 3 fluid-filled chambers Contains Organ of Corti Converts mechanical energy to neuroelectrical energy Structures of the Inner Ear Organ Of Corti End organ of hearing 3 rows of Outer Hair Cells 1 row of Inner Hair Cells Tectorial and Basilar Membranes Cochlear fluids (From Augustana College, “Virtual Tour of the Ear”) Structures of the Inner Ear Hair Cells Frequency specific Low pitches = apex of cochlea High pitches = base of cochlea Fluid movement causes deflection of nerve endings Nerve impulses (electrical energy) are generated and sent to the brain Structures of the Central Auditory System VIIIth Cranial Nerve or Auditory Nerve Bundle of nerve fibers (2530K) Travels from cochlea through internal auditory meatus to skull cavity and brain stem Carry signals from cochlea to primary auditory cortex, with continuous processing along the way Structures of the Central Auditory System Auditory Cortex Wernicke’s Area within Temporal Lobe of the brain Sounds interpreted based on experience/association Anatomy of Hearing Loss Site of Conductive Loss Site of Sensorineural Loss Types of Hearing Loss Conductive = Outer and/or Middle Ear Sensorineural = Inner Ear Mixed = Outer and/or Middle Ear and Inner Ear Auditory Neuropathy Spectrum Disorder (AKA Auditory Neuropathy / Dys-synchrony) = Central Auditory System Unilateral Bilateral Deciphering the Audiogram Horizontal axis: Frequency information (pitch) Deciphering the Audiogram Vertical axis: Sound energy (loudness) Frequency Low Pitch to High Pitch Loudness Soft to Loud Normal Hearing Mild Loss Moderate Loss Moderate Severe Loss Severe Loss Profound Loss Audiogram of Familiar Sounds Plotting Results on an Audiogram White area is inaudible Tan area is audible From: Glen R. Meier, M.S., CCC-A, FAAA http://www.audiologyawareness.com/hea rinfo_audiogramread.asp Conductive Hearing Loss (CHL) Caused by damage, disease, or malformation of the outer or middle ear Sound is prevented from reaching the inner ear Sound perceived as muffled or weak Conductive Hearing Loss Sensorineural Hearing Loss (SNHL) Caused by damage, disease, or malformation of the inner ear Sensory loss associated with inner ear damage Neural loss if hearing nerve cannot send the impulse to the brain Sound perceived as distorted AND weak Sensorineural Hearing Loss Hearing loss and Prosthesis Simulator HeLPS Demo #1 Severity of sensorineural hearing loss http://www.sens.com/helps/helps_d01.htm Demo # 3 Mild Conductive and Mild Sensorineural hearing loss comparison http://www.sens.com/helps/helps_d03.htm - Hearing Test Categories Objective tests or physiologic tests Do not require child's participation Subjective tests Require the child to participate in evaluation Types of Subjective Auditory Tests Sound Booth Tests Visual Reinforcement Audiometry (VRA) Play Audiometry Conventional Audiometry Hearing for Speech All subjective tests evaluate HEARING: requires consistent responses from the child Types of Objective Auditory Tests Tympanometry - middle ear Otoacoustic Emissions (OAEs) - inner ear Auditory Brainstem Response (ABR) -auditory pathways in brainstem DO NOT evaluate Hearing Tympanometry Special earplug placed in the ear canal produces a puff of air The technique measures the response of the eardrum to the change in air pressure Tympanometry evaluates only the middle ear and does not provide information about hearing Used to determine if (temporary) middle ear abnormality contributes to hearing loss Otoacoustic Emissions (OAEs) Special earphones placed into the ear that deliver clicking sound within the ear canal Cochlea responds by producing a sound Probe detects this cochlear emission, which is recorded on computer OAEs detect presence or absence of hearing loss, but cannot assess degree of hearing impairment Method for newborn hearing screening Auditory Brainstem Response (ABR) Special earphones deliver sound to ear Electrodes on the scalp measure brain activity in response to sound Resulting waves provide information on the integrity of the neural pathway ABRs can estimate degree of hearing loss at different frequencies Used for infants and children who cannot consistently respond to subjective testing JCIH - Changes in 2007 Audiologic Evaluation Should be performed by audiologists experienced in pediatric hearing assessment Initial audiologic test battery to confirm hearing loss must include: physiologic measures – objective tests when developmentally appropriate, behavioral methods Completed in both ears regardless of the results of screening tests JCIH 2007 Audiologic Evaluation – Birth to 6 months (Developmental Age) Child and family history Frequency-specific AC (air conduction) ABR; Bone conduction, frequency specific ABR, when indicated Click-evoked ABR if infant has risk indicators for neural HL, any infant demonstrating no response on FS-ABR requires clickevoked ABR OAE (DPOAE or TEOAE) Tympanometry using 1000-Hz probe tone Observation of auditory behavior As cross-check; not for assessment or amplification fitting JCIH 2007 Audiologic Evaluation – 6 months to 36 months Child and family history Parent report of auditory and visual behaviors and communication milestones Behavioral audiometry (VRA, CPA), including: Pure-tone audiometry across the frequency range for each ear Speech detection and speech recognition measures OAE testing Tympanometry & Acoustic Reflex Thresholds ABR testing if responses to behavioral audiometry are not reliable, OR if ABR testing has not been performed previously JCIH 2007 Amplification Infants diagnosed with permanent hearing loss should be fit with amplification within one month of confirmation of hearing loss Treatment and intervention for hearing loss Medical intervention surgical treatment treatment for chronic middle ear disorder Hearing aids Cochlear implants FM systems Treatment and intervention for hearing loss Early intervention for overall development Communication modalities Emotional Social Cognitive Who Early interventionists Speech-language therapists – specialized in hearing impairment Educators for the hearing impaired Monitoring and managing hearing loss Hearing can change – can get worse Plan for future needs - amplification flexibility Monitor hearing aid/cochlear implant function – trouble shoot Provide educational input and consultation (classroom modifications, FMs, educational strategies) How to work collaboratively with audiologists Out reach efforts can be individual or group Mutual information sharing Keep asking questions Take Home Message Infants can and should be assessed as soon as possible to maximize development of maturing auditory skills; sets the stage for language development Family choices for intervention often includes hearing aids/cochlear implants AND early intervention (communication strategies) Questions about hearing? Ask your Audiologist Resources You tube video on hearing: Brandon Pletsch http://www.youtube.com/watch?v=PeTriGTENoc&NR=1 Hearing screening information for parents: www.babyhearing.org American Speech,Language and Hearing Association www.asha.org American Academy of Audiology www.audiology.org Pennsylvania Early Hearing Detection and Intervention www.paearlyhearing.org • Contact information: [email protected] Thank You!