Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Prenatal development wikipedia , lookup
Cell membrane wikipedia , lookup
Endomembrane system wikipedia , lookup
Umbilical cord wikipedia , lookup
Drosophila embryogenesis wikipedia , lookup
Gastrointestinal tract wikipedia , lookup
Human embryogenesis wikipedia , lookup
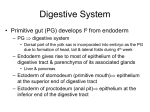
Chapter 24 Development of digestive and respiratory system * digestive and respiratory system derived from primitive gut /foregut /midgut /hindgut ---epi. of digestive and respiratory system derived from endoderm ---CT and MT of digestive and respiratory system derived from splanchnic or visceral mesoderm 1. Development of digestive system 1) derivatives of pharyngeal pouch ---pharyngeal pouch: /outpocketings of endodermal lining of the primary pharynx (extends from the buccopharyngeal membrane to the tracheobronchial diverticulum) /5 pairs ---derivatives of pharyngeal pouch: ① First pharyngeal pouch: ---distal portion: widen into a sac-like structuremiddle ear cavity, the branchial membrane form tympanic membrane or eardrum ---proximal part: remain narrow to form the pharyngotympanic or Eustachian tube ② Second pharyngeal pouch: ---distal portion: obliterated ---remaining part proliferate and primordium of the palatine tonsil form ③ Third pharyngeal pouch: ---dorsal portion: differentiates into inferior parathyroid gland ---ventral part: cells differentiates and form two cell cords, fuse with each other behind the thorax to give rise to the promordium of the thymus ④ Fourth pharyngeal pouch: ---dorsal portion: forms superior parathyroid gland ---ventral portion: degenerates ⑤ Fifth pharyngeal pouch: ---gives rise to the ultimobranchial body, immigrate into thyroid and differentiate into parafollicular cells *development of thyroid gland ---thyroid primordium: by the 4th week, endodermal proliferation of the floor of primitive pharynx, then descends in front of the primitive pharynx as a bilobed diverticulum ---thyroglossal duct: a narrow canal connecting primitive pharynx with thyroid primordium, by the 6th week, becomes solid and disappears. ---foramen caecum: ---thyroglossal cyst and fistula: a cystic remnant of the thyroglossal duct, may be found at any point along the migratory path followed by the thyroid gland; sometimes a thyroglossal cyst is connected to the outside by a fistulous canal, called thyroglossal fistula 2) development of esophagus and stomach ① development of esophagus ---derived from primitive gut extending from the laryngotracheal diverticulum to stomach ---with the descent of the heart and lungs, it lengthens rapidly ---muscular coat, formed by surrounding mesenchyme /striated in upper two-thirds /smooth in lower one-third ② development of stomach ---by 4th week, appears as a fusiform dilation of foregut ---greater and lesser curvatures: by the 5th week, posterior part of stomach grow faster than the anterior portion ---by 7-8th week, around the longitudinal axis, the stomach carries out a 90°clockwise rotation, its left side to face anterior ---rotation around the transverse axis, the caudal(pyloric) end of the stomach moves upward and to the right; the cephalic( cardiac)end moves downward and to the left ③ development of intestine a. midgut derivatives: ---duodenum formation: /formed by terminal part of foregut and the cephalic part of the midgut /“C”-shaped ventrally, rotates to the right ---midgut loop: by 5th week, midgut grow rapidly to form a “U”-shaped loop, its apex connects with yolk sac by way of the narrow vitelline duct /cephalic limb /caudal limb ---physiological umbilical herniation: during the 6th week, midgut loop grow rapidly, enter the umbilical coelum---extraembryonic coelom( in umbilical cord) ---by 6-8th week, midgut loop rotates 90° around an axis formed by the superior mesenteric artery in a counterclockwise direction, move cephalic limb to right, caudal limb left ---caecal swelling: a conical dilation of the caudal limb, form caecum and appendix ---by 10th week, midgut loop return to the abdominal cavity, simultaneously rotates 180° in a counterclockwise direction, move cephalic limb to left, caudal limb right ---cephalic limb: develop into jejunum and most part of ileum ---caudal limb: terminal part of ileum, caecum, appendix, 2/3 transverse colon b. hindgut derivatives ---give rise to 1/3 transverse colon, descending colon, sigmoid ---cloaca: dilation of terminal part of hindgut, connect with allantois, closed by cloacal membrane ---urorectal septum: by 6-7th week, mesenchyma between hindgut and allantois proliferates and form a transverse ridge, divided the cloaca into urogenital sinus and anorectal canal ---urogenital sinus: ventral portion of cloaca, develops into bladder and urethra ---anorectal canal: dorsal portion of cloaca, develops into rectum and upper segment of anal tube 3) development of liver and pancreas ①development of liver and gall bladder ---hepatic diverticulum: by beginning of 4th week, endodermal proliferation of end of the foregut ---hepatic diverticulum extends into the septum transversum and divides into a large cephalic and a small caudal part ---cephalic part cells proliferate to give rise to hepatic cord and bile duct ---cystic diverticulum(caudal part): develop into gall bladder and cystic duct ---the paired vitelline veins and umbilical vein form hepatic sinusoids ---at about 6th week, blood stem cell immigrate into liver from yolk sac, hemopoiesis begin ② development of pancreas ---dorsal pancreatic bud and ventral pancreatic bud: by the end of 4th week, arise from the endoderm of caudal part of the foregut ---dorsal pancreas, ventral pancreas: pancreatic buds cells proliferate to give rise to acinus and ducts ---the ventral pancreas rotates to right-dorsal direction and fuse with dorsal pancreas ---the ventral pancreas forms the inferior part of the head of the pancreas; dorsal pancreas forms other part of pancreas ---main pancreatic duct, together with the common bile duct, enters the duodenum at the site of the major papilla 4) congenital malformations of the digestive tract ① atresia or stenosis of digestive tract: caused by failure of recanalization or improper recanalization, mostly in esophagus and duodenum ② congenital umbilical hernia: caused by incomplete closure of the central part of the abdominal wall, the viscera return to the abdomen but herniated again during the fetal period ③ umbilical fistula and Meckel’ diverticulum: ---umbilical fistula: results from persistence of a patent vitelline duct, meconium or mucus may be found at the umbilicus ---vitelline sinus: results when a small portion of duct remains and opens onto the skin ---vitelline cyst: results when intermediate patent leaves ---vitelline ligament: vitelline duct persist as a fibrous cord, will cause intestinal obstruction ---Mcekel’s diverticulum: caused by persistence of a shore length of the vitelline duct, that remains attached to ileum ④ congenital aganglionic megacolon: results from the absence of ganglion cell of the parasympathetic ganglia, which cause failure of the distal segment to move the intestinal contents onward ⑤imperforate anus, rectal atresia and rectal fistula: ---imperforate anus: results from failure rupture of anal membrane ---rectal atresia: due to a failure of the anal pit to develop or deviation of the urorectal septum in dorsal direction ---rectal fistula: associate with an imperforate anus, between the rectum and the vagina or urinary bladder or urethra ⑥ abnormal rotation of the intestinal loop: nonrotation or reversed rotation of the midgut ⑦ atresia of the gall bladder and bile ducts: results from failure of vacuolization of the epithelial cords or reopen ⑧ annular pancreas: ventral pancreatic bud give rise to two branches, which rotate the duodenum in an opposite direction, the duodenum is completely surrounded by pancreatic tissue 2. development of respiratory system 1) development of larynx, trachea and lung ---laryngotracheal groove: by the begin of 4th week, shallow groove from the ventral wall of the foregut caudal to the hypobranchial eminence ---laryngotracheal diverticulum: laryngotracheal groove deparated from foregut by the esophagotracheal septum ---lung bud: by the end of 4th week, laryngotracheal diverticulum forms two lateral outpocketings. By the 5th week, the right lung bud divides into three branches-main bronchi, and the left into two main bronchi. By the end of 2nd month, lobar bronchi divided into segmental bronchi. By the end of 6th month, approximately 17 generations of subdivisions formed and give rise to terminal bronchi, respiratory bronchi and alveoli. By 7th month, type II alveolar cell appears. ---splanchnic mesoderm develops into the CT, cartilage, SM and visceral pleura 2) congenital malformations ① tracheal stenosis or atresia : caused by failure of reopen or unequal division of the foregut ② tracheoesophageal fistula; imcomplete development or deviation of tracheoesophageal septum, with esophageal atresia ③ hyaline membrane disease( respiratory distress syndrome): incomplete development of type II alveolar cells, a membrane-like substance is formed from the injured pulmonary cells ④ pulmonary agenesis and pulmonary hypoplasia: