Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Typhoid fever wikipedia , lookup
Poliomyelitis eradication wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Hepatitis C wikipedia , lookup
Trichinosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Orthohantavirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hepatitis B wikipedia , lookup
West Nile fever wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Ebola virus disease wikipedia , lookup
Leptospirosis wikipedia , lookup
Mycobacterium tuberculosis wikipedia , lookup
Henipavirus wikipedia , lookup
History of tuberculosis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Tuberculosis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
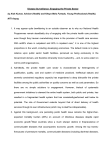
Eurosurveillance Weekly, funded by Directorate General V of the European Commission, is also available on the world wide web at <http://www.eurosurv.org>. If you have any questions, please contact Stuart Handysides <[email protected]>, +44 (0)20-8200 6868 extension 4496. Neither the European Commission nor any person acting on its behalf is liable for any use made of the information published here. Eurosurveillance Weekly: Thursday 16 March 2000. Volume 4, Issue 11 Contents: 1. Lassa fever imported to England 2. Measles outbreak in the Republic of Ireland: update 3. Case definitions for infectious diseases 4. Rates of tuberculosis continue to rise in eastern Europe 5. Monkeys with herpes B infection culled at safari park Lassa fever imported to England Lassa fever has been confirmed in a British aid worker based in Daru, in eastern Sierra Leone, who developed a fever and was brought back to England by a Swiss air ambulance. The man, aged 50, became ill with a fever around 21 February and travelled to Freetown for medical care on 1 March. On arrival in London on 6 March he was admitted to a hospital infectious disease unit with malaise, diarrhoea, and fever, but no pharyngitis or haemorrhage. When bleeding developed he was transferred to another hospital, where he could be managed in high security facilities. Lassa fever is endemic in some rural parts of Sierra Leone, where many subclinical cases occur, but 15% of cases admitted to hospital are fatal. Twelve cases of Lassa fever have been imported into Europe and North America since 1970. This is the fifth case imported to the United Kingdom (UK). In none of the cases has onward transmission been reported. Only people who have had close personal contact with a patient with Lassa fever, or with that patient's body fluids, are at risk of contracting the disease. UK guidelines recommend that the body temperature of such contacts should be monitored daily for 21 days from the last possible date of exposure to infection but that no restriction should be placed on work or movement within the UK1. Contacts who wish to go abroad during a period of surveillance need to be individually assessed for their likely risk and advised accordingly. About 90 people in the UK have been assessed to determine whether or not their level of contact qualifies them for temperature surveillance. Ribavirin prophylaxis has been offered to a few people with documented significant exposure to blood or body fluids. The crew of the Swiss air ambulance are being followed up by Swiss authorities and contacts in Sierra Leone are being managed by the World Health Organization. Reference: 1. Advisory Committee on Dangerous Pathogens. Management and control of viral haemorrhagic fevers. London: Stationery Office, 1996. Reported by Jane Jones ([email protected]), Public Health Laboratory Service Communicable Disease Surveillance Centre, London, England. Measles outbreak in the Republic of Ireland: update One hundred and sixty-one clinically suspected cases of measles were notified between 1 January and 13 March 2000 in Ireland’s Eastern Regional Health Authority (ERHA), compared with 108 cases (average of 9 cases a month) throughout 1999 (1). ERHA includes Dublin city and county and counties Wicklow and Kildare, population 1.3 million (1996 census). The increase in measles notifications has been concentrated in the North Dublin area (population 452 000), and notifications peaked in mid February (figure). Figure: Notifications of measles: Eastern Regional Health Board, 2000 The following interventions have been put in place. Children are now being offered measles, mumps, and rubella (MMR) vaccine at 12 rather than 15 months. Letters have been issued to parents of children for whom there is no record of MMR vaccination to inform them of the outbreak and to advise them to contact their general practitioner to arrange immunisation. Local health centres are generating lists of children for whom there are no records of MMR vaccination. Public health nurses will follow up these children, to encourage vaccination. Letters have been sent to managers of preschool facilities to ask that they encourage parents to have their children immunised and to contact the local senior area medical officer if there is a case of measles in their facility. When a case of measles occurs in a school in an affected area, the parents/guardians of children in that school will be sent a letter from the senior area medical officer, advising them that their child/children should have MMR vaccine now, whether as a primary or booster dose. Parents/guardians will be given the option of attending their family doctor or special health board clinics. Reference: 1. Cronin M, O’Connell T. Measles outbreak in the Republic of Ireland. Eurosurveillance Weekly 2000; 4: 000210. (http://www.eurosurv.org/2000/000210.html) Reported by Mary Cronin ([email protected]) and Tom O’ Connell ([email protected]), Eastern Health Board, Dublin, Republic of Ireland. Case definitions for infectious diseases Case definitions for the 40 diseases considered by the European Commission for inclusion in surveillance networks that cover the European Union (EU) have been developed by the ‘Charter Group’, which consists of the national heads of surveillance of all EU countries (and similar representatives of Iceland, Norway, and Switzerland) as part of a project called ‘Preparing standards for surveillance of infectious diseases on the European Union level’. The purpose was to develop a set of definitions to be used for reference within the EU, for development of national surveillance systems, and for outbreak investigations in the EU.The definitions are based on similar work by the World Health Organization and the Centers for Disease Control and Prevention, but also take into account definitions used in various EU countries. Definitions are given for ‘possible’, ‘probable’, and ‘confirmed’ cases. The idea is that each country can choose to base its surveillance on any of these levels for each disease, as long as the definition used is clearly communicated to the other members of the surveillance network. The case definitions are currently available on the website of the Swedish Institute for Infectious Disease Control at <http://www.smittskyddsinstitutet.se/archive.asp?theSection=4>. They have not been officially approved by the commission or the Network Committee, and anyone interested should look them up and send any comments to [email protected]. Reported by Anders Tegnell ([email protected]) and Johan Giesecke, Swedish Institute for Infectious Disease Control, Stockholm, Sweden. Rates of tuberculosis continue to rise in eastern Europe Rates of tuberculosis are continuing to rise in eastern Europe, according to the latest report from EuroTB (1). Surveillance of tuberculosis in Europe reports on just under 354 000 notifications made by 51 countries for 1997, the third year of the EuroTB surveillance programme. Compared with 1996, the figures show a 2% decrease in the number of cases of tuberculosis in European Union countries, but a 7% increase in former Soviet Union countries, with a 4% increase for the region as a whole. Notification rates ranged from 2.9/100 000 in Malta to 154.1/100 000 in Georgia. In countries notifying < 20 cases /100 000, the rates were highest in those aged over 65, and rates were highest in those between 35 and 54 elsewhere. Rates were higher in men for all age groups above the age of 14 years. Twenty-two countries reported a notification rate of fewer than 20 per 100 000 cases, all but three of which - Albania, Czech Republic and Israel - were in western Europe. Fifteen countries reported a rate of >50/100 000, which, with the exception of Portugal, were in eastern Europe. These figures reflect a trend observed since 1990 (3). The report also notes that increases in the incidence of HIV and AIDS reported for Moldova, the Russian Federation and the Ukraine (2) could have a significant impact on the rate of tuberculosis in these countries in the near future. Patients from overseas accounted for 10% or more of cases in 16 countries, mostly in western Europe, with seven countries notifying more than half of all TB cases from among this group. Drug resistance was also more common in overseas patients in Scandinavia, the Netherlands, Slovenia, and Switzerland. Most of the reported multidrug resistance was in Estonia and Romania where three-quarters of the cases were patients who had never been treated for tuberculosis. The completeness of bacteriological data still varied, with little improvement over previous years (1). A median of 58% of cases were confirmed by culture, but only 21 countries reported this information; 23 reported on sputum smear results, with a median positive proportion of 48%. The report suggests that high quality bacteriological information could best be achieved if all laboratories were to join national notification schemes (4,5). References: 1. EuroTB (CESES/KNCV) and the national coordinators for tuberculosis surveillance in the WHO European Region. Surveillance of tuberculosis in Europe: report on tuberculosis cases notified in 1997. Saint Maurice, France: EuroTB, 1999. (http://www.ceses.org/eurotb) 2. Handysides S. Surveillance of tuberculosis in Europe: first data emerge from "EuroTB". Eurosurveillance Weekly 1997; 1 :971030. (http://www.outbreak.org.uk/1997/971030.html) 3. Raviglione MC, Rieder HL, Styblo K, Khomenko AG, Esteves K, Kochi A. Tuberculosis trends in Eastern Europe and the former USSR. Tubercle Lung Dis 1994; 400- 16. 4. Rieder H, Watson J, Raviglione M, Forssbohm M, Migliori GB, Schwoebel V, et al. Surveillance of tuberculosis in Europe. Recommendations of a Working Group of the World Health Organisation (WHO) and the Europe Region of the International Union Against Tuberculosis and Lung Disease (IUATLD) for uniform reporting on tuberculosis cases. Eur Respir J 1996; 9:1097- 104. (http://www.ncbi.nlm.nih.gov/htbin-post) 5. Schwoebel V, Rieder HL, Watson JM, Raviglione MC for the working group on uniform reporting on tuberculosis cases in Europe. Surveillance of tuberculosis in Europe. Eurosurveillance 1996; 1: 5- 8. (http://www.ceses.org/eurosurv) Reported by Caroline White ([email protected]), PHLS Communicable Disease Surveillance Centre, England. Monkeys with herpes B infection culled at safari park Eleven rhesus macaque monkeys at Woburn Safari Park were found recently to be positive for Herpes B virus, a simian Simplexvirus related to the human herpes simplex virus. Herpes B virus was reclassified as a biohazard level 4 agent by the Advisory Committee on Dangerous Pathogens in 1998 1. The Woburn colony was long-established and a view was taken that all members were likely to be infected. Under COSHH regulations animals infected with level 4 pathogens must be either handled under level 4 containment conditions or destroyed. Since the Woburn colony was of a substantial size and only one level 4 animal facility of limited size exists in the United Kingdom, a decision was made to cull the entire colony. Other zoos and safari parks that hold rhesus monkeys are arranging for testing to be carried out. Herpes B virus does not cause illness in macaques, but infection in humans is often fatal (4/9 cases have died since acyclovir became available) and survivors usually have neurological sequelae. Fewer than 40 human cases have been documented worldwide since the virus was identified in 1932; most were infected by monkey bites but indirect exposure to monkey body fluids can also cause infection. A laboratory worker in the United States died 42 days after being splashed in the eye by a body fluid from a rhesus monkey 2. The rarity of human B virus disease, given the frequency of monkey related exposure, suggests monkey to human transmission seldom occurs. Control strategies include selection of B virus free colonies for zoos and biomedical research, development of screening and safe handling policies, and the adoption of guidelines for the management of potential B virus exposure3-5. 1. Advisory Committee on Dangerous Pathogens. Supplement to: Categorisation of biological agents according to hazard and categories of containment (fourth edition, 1995). Sudbury: HSE Books, 1998. (http://www.open.gov.uk/hse/agents.htm) 2. Fatal Cercopithecine herpesvirus 1 (B virus) infection following a mucocutaneous exposure and interim recommendations for worker protection. MMWR Morb Mortal Wkly Rep 1998; 47: 1073-6, 83. (ftp://ftp.cdc.gov/pub/Publications/mmwr/wk/mm4749.pdf) 3. Holmes GP, Chapman LE, Stewart JA, Straus S, Hilliard JK, Davenport DS. Guidelines for the prevention and treatment of B virus infections in exposed persons. Clin Infect Dis 1995; 20: 421-39. 4. Guidelines for prevention of Herpesvirus simiae (B virus) infection in monkey handlers. MMWR Morb Mortal Wkly Rep 1987; 36: 680-2, 687-9. (http://www.cdc.gov/epo/mmwr/preview/mmwrhtml/00015936.htm) Reported by Stuart Handysides ([email protected]), PHLS Communicable Disease Surveillance Centre, London, England.