Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
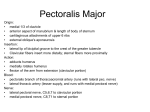
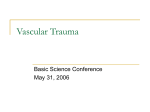
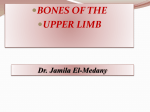
UPPER EXTREMITY Lecture #1 Bones and superficial structures of the upper limb Associate Professor Dr. Alexey Podcheko Spring 2015 Intended Learning Outcomes BONES OF UPPER LIMB • • • • • • Clavicle Scapula Humerus Bones of Forearm Bones of Hand Surface Anatomy of Upper Limb Bones FASCIA, EFFERENT VESSELS, CUTANEOUS INNERVATION, AND MYOTOMES OF UPPER LIMB • • • Fascia of Upper Limb Venous Drainage of Upper Limb Cutaneous Innervations of Upper Limb UPPER LIMB SEGMENTS 1. 2. 3. 4. Shoulder Arm Forearm Hand Shoulder • Proximal segment of the limb that overlaps parts of the trunk and lower lateral neck • Includes the pectoral, scapular, and lateral supraclavicular regions and is built on half of the pectoral girdle •The pectoral girdle is a bony ring, incomplete posteriorly, formed by the scapulae and clavicles and completed anteriorly by the manubrium of the sternum Arm (Latin - brachium) • First segment of the free upper limb (more mobile part of the upper limb independent of the trunk) and the longest one • Extends between and connects the shoulder and the elbow and is centered around the humerus Forearm (Latin - antebrachium): • Is the second longest segment of the limb • Extends between and connects the elbow and the wrist and contains the ulna and radius Hand (Latin - manus) • part of the upper limb distal to the forearm that is formed around the carpus, metacarpus, and phalanges. • It is composed of the wrist, palm, dorsum of hand, and fingers (including an opposable thumb) and is richly supplied with sensory endings for touch, pain, and temperature. Bones of the Upper Limb 1. Clavicle 2. Humerus 3. Radius 4. Ulna 5. Carpal bones (8) 6. Metacarpal bones (5) 7. Phalanges •Sternal end articulates with the manubrium of the sternum at the sternoclavicular (SC) joint. •Acromial end articulates with the acromion of the scapula at the acromioclavicular (AC) joint •Serves as a cranelike strut, keeps scapula and free limb away from the trunk so that the limb has maximum freedom of motion. •Commonly fractured Clavicle CLINICAL CORRELATES: Fracture of the Clavicle -The weakest part of the clavicle is the junction of its middle and lateral thirds -In children fractures often caused by: a) fall b) by the obstetrician in breech presentation when the infant presses against the maternal pubic symphysis during its passage through the birth canal CLINICAL CORRELATES: Fracture of the Clavicle • Middle third fracture results in upward displacement of the proximal fragment (sternocleidomastoid muscle) and downward displacement of the distal fragment by the deltoid muscle and gravity • May cause injury to the brachial plexus: -paresthesia (sensation of tingling, burning, and numbness) in the area of the skin supplied by medial brachial and antebrachial cutaneous nerves • May cause fatal hemorrhage from the subclavian vein • May cause thrombosis of the subclavian vein (cause of pulmonary embolism) CLINICAL CORRELATES: Fracture of the Clavicle A fracture may also result from a fall directly on the shoulder. A fracture of the clavicle is often incomplete in younger children, which is called ‘greenstick fracture’, in which one side of a bone is broken and the other is bent. CLINICAL CORRELATES: Clinical Signs of Fracture of Clavicle •Person support the sagging limb with the other limb •Lateral fragment of the clavicle may be pulled toward the chest •Clavicle looks shortened (Overriding of the bone fragments) CLINICAL CORRELATES: Treatment of Fracture of Clavicle Ice pack, sling support for 6 weeks. Sling Figure of eight bandage Surgical treatment: plates and screws are used CLINICAL CORRELATES: Congenital disorders • • • Clavicle is the first bone to begin ossification during fetal development, but it is the one of the last to complete ossifi cation, at approximately 21 years of age Is the only long bone to be ossified intramembranously Cleidocranial dysplasia, a disorder characterized by patent fontanelles, delayed closure of cranial sutures, Wormian bones*, delayed eruption of secondary teeth, primitive clavicles, and short height Scapula - aka shoulder blade • Overlying the 2nd-7th ribs • Structures you should know: 1. 2. 3. 4. 5. 6. 7. 8. 9. Spine of the scapula Supraspinous fossa Infraspinous fossa Subscapular fossa Acromion Coracoid process Glenoid cavity (glenohumeral joint ) Medial border of the scapula Scapular notch (transmits the suprascapular nerve) Scapula: more details 1. Spine of the Scapula • forms upper supraspinous and lower infraspinous fossae , and also provides an origin for the deltoid and an insertion for the trapezius 2. Acromion • Is the lateral end of the spine and articulates with the clavicle • Provides an origin for the deltoid and an insertion for the trapezius 3. Coracoid Process: Provides the origin of the • coracobrachialis and biceps brachii • insertion of the pectoralis minor • attachment site for the coracoclavicular, coracohumeral, and coracoacromial ligaments and the costocoracoid membrane Clinical Correlates:Calcification of the superior transverse scapular ligament • Suprascapular notch is bridged by the superior transverse scapular ligament and transmits the suprascapular nerve • Calcification of the superior transverse scapular ligament may trap or compress the suprascapular nerve as it passes through the scapular notch affecting functions of the supraspinatus and infraspinatus muscles (rotator cuff muscles) – affecting the abduction and external rotation of arm Scapula (Other structures) Humerus (arm bone): Important Structures • Forms glenohumeral joint and articulates with radius and ulna • Structures: 1. Head 2. Greater tubercle (lateral margin of the humerus) 3. Lesser tubercle ( anterior margin of humerus) 4. The intertubercular (bicipital) groove separates the tubercles and provides protected passage for the slender tendon of the long head of the biceps muscle 5. Surgical neck (narrow part distal to the head and tubercles) 6. Anatomical neck (groove circumscribing the head and separating it from the greater and lesser tubercles) 7. Deltoid tuberosity (for attachment of the deltoid muscle) 8. Oblique radial groove (groove for radial nerve and deep artery of arm) 9. Medial epicondyle and the lateral epicondyle, providing for muscle attachment. 10. Trochlea; 11. Capitulum; and olecranon fossa 12. Coronoid and radial fossa Humerus (arm bone): more details 1. Head: Articulates with the scapula at the glenohumeral joint 2. Anatomic Neck: Is an indentation distal to the head and provides an attachment for the fibrous joint capsule 3. Greater Tubercle: Lies just lateral and distal to the anatomic neck and provides attachments for the supraspinatus, infraspinatus, and teres minor muscles 4. Surgical Neck: narrow area distal to the tubercles that is a common site of fracture and is in contact with the axillary nerve and the posterior humeral circumflex artery Clinical Correlations: Humerus fractures • Fracture of the greater tubercle: occurs by direct trauma or by violent contractions of the supraspinatus muscle. The bone fragment has the attachments of the supraspinatus, infraspinatus, and teres minor muscles, whose tendons form parts of the rotator cuff. • Fracture of the surgical neck may injure the axillary nerve and the posterior humeral circumflex artery as they pass through the quadrangular space. Humerus (arm bone): more details • Lesser Tubercle: Lies on the anterior medial side of the humerus, just distal to the anatomic neck, and provides an insertion for the subscapularis muscle • Intertubercular (Bicipital) Groove :Lies between the greater and lesser tubercles, lodges the tendon of the long head of the biceps brachii muscle, and is bridged by the transverse humeral ligament, provides insertions for the pectoralis major on its lateral lip, the teres major on its medial lip, and the latissimus dorsi on its floor . • Deltoid Tuberosity: Is a rough triangular elevation on the lateral aspect of the midshaft that marks the insertion of the deltoid muscle • Spiral Groove: Contains the radial nerve, separating the origin of the lateral head of the triceps above and the origin of the medial head below Clinical Correlations: Humerus fractures • Fracture of the shaft may injure the radial nerve and deep brachial artery in the spiral groove. • Supracondylar fracture (common in children) is a fracture of the distal end of the humerus: occurs when the child falls on the outstretched hand with the elbow partially flexed and may injure the median nerve. • Fracture of the medial epicondyle may damage the ulnar nerve. This nerve may be compressed in a groove behind the medial epicondyle “funny bone,” causing numbness. • USMLE SCENARIO: • A 24-year-old mountain climber presents to the emergency room with right shoulder pain following a fall. He was climbing a cliff at a nearby national park when he lost his grip and fell approximately 5 meters onto the boulders below. He says that he "landed on his right arm and heard the bone snap”. Physical examination reveals total inability to extend the right wrist X-ray reveals a fracture of the right humeral shaft. Which of the following arteries is most likely to be injured in this patient? • A. Anterior circumflex humeral artery • B. Brachial artery • C. Common interosseous artery • D. Deep brachial artery • E. Radial collateral artery Bones of the Forearm • this unit is formed by two parallel bones, one of which (the radius) can pivot about the other (the ulna), supination and pronation are possible. This makes it possible to rotate the hand when the elbow is flexed. Radius • Situated lateral to the ulna • Structures you need to identify: • 1. Head (articulates with the capitulum of the humerus and the radial notch of the ulna and is surrounded by the annular ligament) • 2. Distal End (Articulates with the proximal row of carpal bones -scaphoid, lunate, and triquetral bones ) • 3. Radial Tuberosity (prominence just distal to the neck and provides an attachment site for the biceps brachii tendon) • 4. Styloid Process (distal end of the radius and is approximately 1 cm distal to that of the ulna and provides insertion of the brachioradialis muscle - can be palpated in the proximal part of the anatomic snuffbox between the extensor pollicis longus and brevis tendons Radius CLINICAL CORRELATES: RADIUS FRACTURES • Colles’s fracture of the wrist is a distal radius fracture in which the distal fragment is displaced (tilted) posteriorly, producing a characteristic bump described as dinner (silver) fork deformity because the forearm and wrist resemble the shape of a dinner fork. • If the distal fragment is displaced anteriorly, it is called a reverse Colles’s fracture (Smith’s fracture). • Ulna Medial and longer of the two forearm bones • Structures you need to identify: 1. Olecranon ( curved projection on the back of the elbow that provides an attachment site for the triceps tendon) 2. Coronoid Process (below the trochlear notch, attachment site for the m.brachialis) 3. Trochlear Notch (receives the trochlea of the humerus) 4. Ulnar Tuberosity (prominence distal to the coronoid process that provides an attachment site for the m. brachialis) 5. Radial Notch (accommodates the head of the radius at the proximal radioulnar joint) 6. Head (articulates with the articular disk of the distal radioulnar joint and has a styloid process) Bones of the Hand • The wrist, or carpus, is composed of eight carpal bones (carpals) arranged in proximal and distal rows of four (lateral to medial): scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate (mnemonic: Sandra Likes To Pat Tom’s Two Cold Hands)- (Trapezium precedes trapezoid alphabetically!) •Sandra Likes To Pat Tom’s Two Cold Hands)- (Trapezium precedes trapezoid alphabetically!) – •scaphoid, lunate, triquetrum, pisiform, •trapezium, trapezoid, capitate, and hamate USMLE SCENARIO • A 34-year-old female presents to the emergency room after failing in the bathroom. She complains of wrist pain and numbness in her right palm. Based on her symptoms, you suspect that she has dislocated the lunate bone in the wrist. Identify the lunate bone on the X-ray below A.A B.B C.C D.D E.E CLINICAL CORRELATES: Fractures of carpal bones • The scaphoid is the most frequently fractured carpal bone • Fracture of the scaphoid occurs after a fall on the outstretched hand, shows a deep tenderness in anatomical snuffbox, and damages the radial artery and cause avascular necrosis of the bone and degenerative joint disease of the wrist • Fracture of the hamate may injure the ulnar nerve and artery because they are near the hook of the hamate CLINICAL CORRELATES: Guyon’s canal syndrome • Guyon’s canal (ulnar tunnel) is formed by the pisiform, hook of the hamate, and pisohamate ligament, deep to the palmaris brevis and palmar carpal ligament and transmits the ulnar nerve and artery. • Guyon’s canal syndrome is an entrapment of the ulnar nerve in the Guyon’s canal • Symptoms: pain, numbness, and tingling in the ring and little fingers, followed by loss of sensation and motor weakness. • Dx: surgical decompression of the nerve. USMLE SCENARIO • A 19-year-old female presents to your office complaining of right hand clumsiness. Physical examination reveals decreased sensation over the fifth finger and a flattened hypothenar eminence. The affected nerve is commonly injured at which at the following locations? • A. Carpal tunnel • B. Hook of the hamate • C. Surgical neck of the humerus • D Head of the radius • E. Coracobrachial muscle Metacarpals & Phalanges • Miniature long bones consisting of bases (proximal ends), shafts (bodies), and heads (distal ends). • Metacarpal Heads form the knuckles of the fist. • Phalanges - occur in fingers (three each) and thumb (two) CLINICAL CORRELATES: Fractures of carpal bones • Bennett’s fracture is a fracture of the base of the metacarpal of the thumb. • Boxer’s fracture is a fracture of the necks of the second and third metacarpals, seen in professional boxers, and typically of the fifth metacarpal in unskilled boxers Surface Anatomy of the Upper Limb Bones Identify on your friend or yourself: •Clavicle •Jugular notch •Acromion •Acromial angle •The crest of the scapular spine •The medial border of the scapula •The inferior angle of the scapula •The head of the humerus ( push fingers into the armpit). The greater tubercle of the humerus •The shaft of the humerus The medial and lateral epicondyles •Styloid process of radius and ulna The coracoid process of the scapula can be felt by palpating deeply at the lateral side of the clavipectoral triangle Superficial structures of the upper limb 1. 2. 3. 4. Fascia of the Upper Limb CUTANEOUS NERVES SUPERFICIAL VEINS LYMPHATIC VESSELS Fascia of the Upper Limb • Deep fascia of the upper limb surrounds and contains the structures of the upper limb as an expansion-limiting membrane deep to the skin and subcutaneous tissue. • Deep fascia forms fascial compartments containing individual muscles or muscle groups of similar function and innervation • The compartments also contain or direct the spread of infection or hemorrhage Axillary fascia forms the floor of the axilla and is continuous with the pectoral fascia SUPERFICIAL VEINS OF THE UPPER LIMB (4) • Cephalic Vein (arises from dorsal venous network along the lateral surface of the biceps, lies in the deltopectoral triangle, ends in the axillary vein) • Basilic Vein (arises from the dorsal venous arch of the hand and lies along the ulnar border of the forearm and passes anterior to the medial epicondyle, joins the brachial veins to form the axillary vein) SUPERFICIAL VEINS OF THE UPPER LIMB (4) • Median Cubital Vein (connects the cephalic vein to the basilic vein over the cubital fossa, lies close to brachial artery which is vulnerable to being punctured during IV puncturess) • Median Vein of Forearm (arises in the palmar venous network, ascends on the front of the forearm, and terminates in the median cubital or the basilic vein) Superficial Veins Venous Palmar arch CUTANEOUS NERVES OF THE UPPER LIMB 1. Supraclavicular Nerve - cervical plexus (C3-4) and innervates the skin over the upper pectoral, deltoid, and outer trapezius areas 2. Medial Brachial Cutaneous Nerve: from the medial cord of the brachial plexus (C8-T1) and innervates the medial side of the arm 3. Medial Antebrachial Cutaneous Nerve: medial cord of the brachial plexus and innervates the medial side of the forearm (C8-T1) 4. Lateral Brachial Cutaneous Nerve: from the axillary nerve(C5-6) and innervates the lateral side of the arm 5. Lateral Antebrachial Cutaneous Nerve: from the musculocutaneous nerve and innervates the lateral side of the forearm (C5-C6) 6. Posterior Brachial and Antebrachial Cutaneous Nerves: from the radial nerve and innervate the posterior sides of the arm and forearm (C5-8) 7. Intercostobrachial Nerve: Lateral cutaneous branch of the second intercostal nerve emerging from the second intercostal space and may communicate with the medial brachial cutaneous nerve (T12) CUTANEOUS NERVES OF THE UPPER LIMB Referred pain to the shoulder most probably indicates involvement of the phrenic nerve (or diaphragm). The supraclavicular nerve (C3–C4), which supplies sensory fi bers over the shoulder, has the same origin as the phrenic nerve (C3–C5), which supplies the diaphragm!