Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
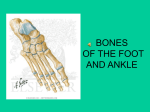
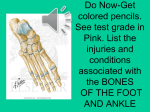
Radiology of LE (21) Bone Knee Description/Pictures -normal: AP x-ray -normal: lateral x-ray useful for assessing soft tissues as well as bones; the quadriceps & patellar tendons are visible; note the normal suprapatellar pouch between fat pads above the patella (asterisks) widening of these fate pads or increased density in this area can indicate a knee joint effusion -normal sunrise view (“skyline” view) not usu. indicated in the context of trauma; more helpful to assess knee pain d/t suspected patellofemoral compartment OA; normal patellofemoral compartment spacing -tibial plateau fx- AP view *fx fragment is displaced & depressed from its normal position (dotted line) -tibial plateau fx- lateral view *no visible fx line; depressed tibial plateau contour (arrow); lipohemarthrosis (fat & blood in the joint) -normal anatomical variants A fabella is a normal sesamoid bone of the lateral head of gastrocnemius tendon - not to be mistaken for a fracture or loose body -normal anatomical variants bipartite patella is a common normal variant; note the smooth edges of each part *Injury to the interface of the 2 components is possible which may be symptomatic -Knee MRI- coronal (1) lateral femoral condyle (2)medial femoral condyle (3) PCL (4) lateral meniscus (5) medial meniscus (6) tibia (7) fibula (8) ACL (9) LCL (10) MCL -MRI- sagittal (1) patella (2) femur (3) infrapatellar fat pad (4) ACL (5) PCL (6) tibia (7) patellar ligament (8) Quad femoris tendon (9) popliteus -MRI- axial 1=patella; 2=Lateral condyle of femur; 3=medial condyle of femur; 4=ACL; 5=PCL; 6=LCL; 7=MCL; 8=popliteal artery and vein; 9=popliteus; 10=biceps femoris Tibia & Fibula -Comminuted fx with medial displacement & posterior angulation -Tibial stress fx periosteal stress reaction are signs of stress injury (often not present on the initial XR); hx of chronic pain worsened by activity -toddler’s fx a spiral tibial fx seen in young children; associated with a twisting injury and may present with refusal to weight-bear; often little or no displacement & fx line is very subtle *some not visible on initial XR but cause a periosteal stress reaction which becomes visible on f/u Ankle -normal AP “mortise” the weight bearing portion is formed by the tibial plafond and the talar dome; joint extends on the “lateral gutter” and the “medial gutter” joint evenly spaced throughout -Trimalleolar fx- AP & lateral views (1) medial malleolus fx; (2)lateral malleolus fx proximal to the ankle & extending up the fibula [Weber C fx]; (3) posterior malleolus fx *joint is unstable & widened anteriorly (arrowheads) and the distal tibiofibular syndesmosis (asterisk) *talus is displaced posteriorly & laterally along w/the medial & lateral malleolus bone fragments -abnormal ankle which ligaments indicated by 1 & 2? (1) anterior tibiotalar & (2) tibiofibular -Maisonneuve fx typical mechanism of action for fracture? *disruption of the medial ankle joint w/small bone avulsion *OR disruption of the distal tibio-fibular syndesmosis *no fibular fx is visible at the ankle raising the suspicion of a proximal fibular fx *spiral fracture of the proximal fibula Foot -osteochondral fracture talus -Dorsal-plantar & oblique views *hindfoot calcaneus + talus *midfoot clavicular + cuboid + cuneiforms *Forefoot metatarsals + phalanges *MC- medial cuneiform *IC - intermediate cuneiform *LC- lateral cuneiform *note the sesamoid bones! (1)hind-midfoot junction CHOPART’S JOINTS (2)mid-forefoot junction tarsometatarsal joints (TMTJs) = LISFRANC’S JOINT -ligament anatomy -abnormal extremely strong Lisfranc’s ligament runs obliquely from the plantar surface of the base of the second metatarsal to the plantar surface of the medial cuneiform, and is a major restraint to midfoot disruption -anatomic variants 5th metatarsal base fx *L image - fx line passes transversely across the bone *R image – a normal unfused 5th metatarsal base apophysis is aligned more longitudinally along the bone *what would be a typical hx presentation for a fx like this? Avulsion- This type of fracture is the result of an injury in which the ankle rolls Jones fracture- occur in a small area of the fifth metatarsal that receives less blood and is therefore more prone to difficulties in healing; can be either a stress fracture (a tiny hairline break that occurs over time) or an acute (sudden) break; caused by overuse, repetitive stress, or trauma; They are less common and more difficult to treat than avulsion fractures Pain, swelling, and tenderness on the outside of the foot; Difficulty walking; Bruising may occur