Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Jatene procedure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
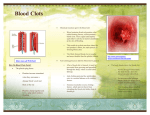
Anticoagulation and Associated Disorders Mikaela Elwell, Pharm.D. Jordan Light, Pharm.D. PGY1 Pharmacy Residents Disclosure We do not have (nor does any immediate family member have) a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with an organization whose philosophy could potentially bias our presentation. Objectives • Describe how clot formation occurs and list the risk factors for developing a clot • Identify and discuss the unique attributes of the most commonly used anticoagulant • Explain the utility of reversal agents and identify which anticoagulant they reverse • Recall important medication safety points for the common anticoagulants “Blood thinners” and Antiplatelets ANTICOAGULANTS Blood Clot Formation Injury to tissue / blood vessel Platelets adhere to damaged tissue/vessels Coagulation Cascade Platelet Plug = Clot Formed Image from: http://www.nlm.nih.gov/medlineplus/ency/imagepages/19462.htm When Bad Clots Arise Clot in an Artery Clot in a vein Venous Thromboembolism (VTE) – Deep vein thrombosis (DVT) – Pulmonary Embolism (PE) Atherosclerosis Stroke Heart Attack Right Image from: http://nymethodist.adam.com/content.aspx?productId=10&pid=10&gid=000003 Left Image from: http://www.nhlbi.nih.gov/health/health-topics/topics/atherosclerosis Risky Business Smoking Obesity Hypertension Hyperlipidemia Diabetes Pregnancy Oral contraception Trauma Immobility – airplane or car trips > 60 years old Family History Certain cancers or surgeries Venous Thromboembolism • Caused by blood clot forming in the venous circulation – Deep vein thrombosis (DVT): blood clot that blocks the veins to the lower extremities – Pulmonary embolism (PE): blood clot that breaks off and travels to the lungs, blocking the pulmonary arteries Heart Attack • Also called a ‘myocardial infarction’ • Occurs when blood flow in the arteries going to the heart become blocked Stroke • Occurs when a blood clot blocks the arteries going to the brain Atrial Fibrillation • Most common type of abnormal heart rhythm – Periods of rapid and irregular beating • Caused by an electrical problem in the heart • Irregular heartbeats can result in blood pooling in the heart blood clot stroke Prevention is Key Risk of Stroke Prevent blocking the flow of blood to the brain Risk of Heart Attack Prevent blocking the flow of blood to the heart After heart valve replacement Atrial fibrillation Reduced mobility Prior history of a VTE American Society of Hematology. Blood Clots. 07/1/2015 Available at: http://www.hematology.org/Patients/Clots/ Blood Clot Formation Injury to tissue / blood vessel Platelets adhere to damaged tissue/vessels Coagulation Cascade Platelet Plug = Clot Formed Image from: http://www.nlm.nih.gov/medlineplus/ency/imagepages/19462.htm Anticoagulants in the Clotting Cascade Warfarin Rivaroxaban Apixiban Dabigatran Argatroban Unfractionated heparin Low-molecular weight heparin CLOT Image from: http://www.nature.com/nrd/journal/v8/n5/fig_tab/nrd2851_F1.html Unfractionated Heparin (UFH) • Discovered: 1922 – Isolated from pig livers – Greek “Hepar” meaning liver • Used in humans: 1940’s PROS Reversal Agent: Protamine Monitoring available Cons Unpredictable patient response • Mixed chain lengths • 1/3 of UFH molecules active Monitoring required • aPTT (activated partial thromboplastin time) • 1.5-2.5x patient’s baseline • Mechanism of action (MOA): – Potentiates antithrombin • Route: IV, SQ 1. 2. Wardrop D, et.al. BJH. 2008.141:757-763 Dipiro JT, et. al. Pharmacotherapy: A pathophysiological Approach. McGraw Hill Inc. 2011 Heparin Products Caution: Several strengths available – always double check Left and Middle Image from: http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=cbc26e3c-aee9-4c0d-bdb1-bf350308fbce Right Image from: http://www.ismp.org/NAN/files/NAN-20130610.pdf Low-Molecular Weight Heparin (LMWH) • Discovered: 1980’s – Chemical/enzymatically changing UFH PROS • Predictable patient response • No frequent lab monitoring • Longer acting – dosed 1 -2 times daily • Given at home Cons • Subcutaneous injection • Renal dose adjustment • Enoxaparin (Lovenox) • Mechanism of action (MOA): – Potentiates antithrombin • Route: SQ Dipiro JT, et. al. Pharmacotherapy: A pathophysiological Approach. McGraw Hill Inc. 2011 Heparin Induced Thrombocytopenia (HIT) • Uncommon – UFH: • 5 days: 1-3% • 14 days: 6% – LMWH: <1% Exposure to Heparin Production of Antibodies AntibodyHeparin complex activates platelets • Life-threatening • Treatment: – Discontinue ALL sources of heparin – Start alternative anticoagulant: • Argatroban – IV infusion Dipiro JT, et. al. Pharmacotherapy: A pathophysiological Approach. McGraw Hill Inc. 2011 Increased clot formation Warfarin PROS • Discovered: 1941 – Wisconsin Alumni Research Foundation (WARF) • Reversal Agent: Vitamin K • Oral tablet • Monitoring for bleed/clot risk • International Normalized Ratio (INR) • Standardized worldwide • 1948: used as a rodenticide • MOA: Warfarin Dysfunctional Vitamin K reductase Coagulation Factors II, VII, IX, X, Protein C & S Dietary Vitamin K Functional 1. 2. 3. Wardrop D, et.al. BJH. 2008.141:757-763 Dipiro JT, et. al. Pharmacotherapy: A pathophysiological Approach. McGraw Hill Inc. 2011 Image from: http://www.surgery.usc.edu/hepatobiliary/liversurgery.html Warfarin Cons • Frequent monitoring: INR • Consistently eat Vitamin K rich foods o Leafy greens o Kale o Chickpeas o Spinach o Broccoli o Tea – green & black o Onions o MANY drug interactions Tablets: • • • • • • • • • 1mg – pink 2mg – lavender 2.5mg – green 3mg – brown 4mg – blue 5mg – peach 6mg – teal 7.5mg – yellow 10mg – white Caution: Dispensing Errors – dosing changes may be frequent (based on INR levels) Strength Pneumonic: Please Let Greg Brown Bring Peaches to Your Wedding New Oral Anticoagulants (NOAC) • Direct Thrombin Inhibitor – Dabigatran (Pradaxa) (2010) • Daily PROS Oral tablets Fewer interactions No lab monitoring Rapid Onset of Action Cons Miss a dose – risk of clot No current approved reversal agent for anti-Xa inhibitors • Anti-Xa Inhibitors – Rivaroxaban (Xarelto) (2011) • Daily – Apixaban (Eliquis) (2012) • Twice daily Caution: Black Box Warning Premature discontinuation increases the risk of clotting events ◦ Patients should never run out / miss refills 1. 2. DailyMed. Dabigatran, Rivaroxaban, Apixaban Package Inserts. 2015 Idaruxizumab. Press Release Archive. Available at: http://us.boehringeringelheim.com/news_events/press_releases/press_release_archive/2015/4-232015-fda-grants-priority-review-boehringer-ingelheims-biologics-license-application-idarucizumab.html Clot Busters • Work by dissolving a clot that already exists • Used in emergency settings (e.g. new onset stroke, heart attack, or pulmonary embolism) • “Thrombolytic” or “fibrinolytic” • Alteplase (Activase)* • Tenecteplase (TNKase) • Reteplase (Retavase) – IV infusions • Must be prepared quickly ANTIPLATELET AGENTS Antiplatelets Aspirin – acetylsalicylic acid – Willow bark – salicyclic acid – Egyption’s recorded use 1534 BC – Tablet form: 1904 MOA: – Inhibits Cyclooxygenase-1 • Prevents thromboxane A2 formation – Prevents platelet aggregation – Irreversible for life of the platelet Primary & Secondary Prevention: – men age 45-79 to reduce risk of myocardial infarction (MI) – women age 55-79 to reduce risk of ischemic stroke – previous stroke or MI Caution: ◦ Non-steroidal anti-inflammatory (NSAID): ◦ risk of gastrointestinal bleed 1. 2. Sneader W. The discovery of aspirin: a reappraisal. BMJ. 2000 Dec 23; 321(7276): 1591–1594. Using Aspirin for the Primary Prevention of Cardiovascular Disease. AHRQ.June 2009. Antiplatelets Clopidogrel • Clopidogrel (Plavix) • MOA: – Inhibits P2Y12 ADP • Alters platelet membrane • Prevents platelet aggregation • Secondary Prevention: – Previous stroke or MI 1. 2. PROS Less GI bleeding than aspirin Cons Prodrug - Liver must transform to active drug • Efficacy decreased if liver enzyme is inhibited/reduced Dipiro JT, et. al. Pharmacotherapy: A pathophysiological Approach. McGraw Hill Inc. 2011 Image from: http://archinte.jamanetwork.com/article.aspx?articleid=215618 High Alert Medications • ALL anticoagulants and antiplatelets – Serious risk of bleed 1. 2. ISMP Medication Safety Alert. Jan. 11, 2000. Available at: https://www.ismp.org/newsletters/acutecare/articles/20070111.asp Image from: http://libguides.usc.edu.au/risk High Alert Medications • ALL anticoagulants and antiplatelets – Serious risk of bleed • Risks: Duplicate or concurrent therapy Accidental stoppage Look-alike vials or syringes Look-alike names Dosing errors Drug and Food Interactions 1. 2. ISMP Medication Safety Alert. Jan. 11, 2000. Available at: https://www.ismp.org/newsletters/acutecare/articles/20070111.asp Image from: http://libguides.usc.edu.au/risk REVERSAL AGENTS Protamine • • • • Reverses: heparin Binds to heparin to form a complex, and neutralizes its effects Storage: refrigerator Dose determined by amount of heparin given – 1 mg protamine for every 100 units of heparin Vitamin K • “Phytonadione” • Reverses: warfarin • Competes with warfarin in binding to receptor on vitamin K-dependent clotting factors • Given either PO or IV depending on: – How high is the INR? – Is the patient bleeding? Praxbind • • • • “Idarucizumab” Reverses: dabigatran FDA approved October 2015 Monoclonal antibody that binds with high affinity to dabigatran and neutralizes it within minutes • Given as two separate 2.5 g infusions • Storage: refrigerator • Do NOT tube! Bad Blood: Common Hematologic Diseases and Their Management Mikaela Elwell, Pharm.D. Jordan Light, Pharm.D. PGY1 Pharmacy Residents