Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
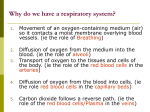
Gas Exchange in Humans In humans the gas exchange organ system is the respiratory or breathing system. The main features are shown in this diagram. The actual respiratory surface is on the alveoli inside the lungs. An average adult has about 600 million alveoli, giving a total surface area of about 100m², so the area is huge. The walls of the alveoli are composed of a single layer of flattened epithelial cells, as are the walls of the capillaries, so gases need to diffuse through just two thin cells. Water diffuses from the alveoli cells into the alveoli so that they are constantly moist. Oxygen dissolves in this water before diffusing through the cells into the blood, where it is taken up by haemoglobin in the red blood cells. The water also contains a soapy surfactant which reduces its surface tension and stops the alveoli collapsing. The alveoli also contain phagocyte cells to kill any bacteria that have not been trapped by the mucus. The steep concentration gradient across the respiratory surface is maintained in two ways: by blood flow on one side and by air flow on the other side. This means oxygen can always diffuse down its concentration gradient from the air to the blood, while at the same time carbon dioxide can diffuse down its concentration gradient from the blood to the air. The flow of air in and out of the alveoli is called ventilation and has two stages: inspiration (or inhalation) and expiration (or exhalation). Lungs are not muscular and cannot ventilate themselves, but instead the whole thorax moves and changes size, due to the action of two sets of muscles: the intercostal muscles and the diaphragm. Inspiratio n The diaphragm contracts and flattens downwards The external intercostal muscles contract, pulling the ribs up and out this increases the volume of the thorax this increases the lung and alveoli volume this decreases the pressure of air in the alveoli below atmospheric (Boyle's law) Normal expiration air flows in to equalise the pressure The diaphragm relaxes and curves upwards The external intercostal muscles relax, allowing the ribs to fall this decreases the volume of the thorax this decreases the lung and alveoli volume this increases the pressure of air in the alveoli above atmospheric (Boyle's law) Forced expiration air flows out to equalise the pressure The abdominal muscles contract, pushing the diaphragm upwards The internal intercostal muscles contract, pulling the ribs downward This gives a larger and faster expiration, used in exercise These movements are transmitted to the lungs via the pleural sac surrounding each lung. The outer membrane is attached to the thorax and the inner membrane is attached to the lungs. Between the membranes is the pleural fluid, which is incompressible, so if the thorax moves, the lungs move too. The alveoli are elastic and collapse if not held stretched by the thorax (as happens in stab wounds or deliberately to rest a lung). Controlling Breathing Rate But what controls the breathing rate? It is clearly an involuntary process (you don’t have to think about it), and like many involuntary processes (such as heart rate, coughing and sneezing) it is controlled by a region of the brain called the medulla. The medulla and its nerves are part of the autonomic nervous system (i.e. involuntary). The region of the medulla that controls breathing is called the respiratory centre. It receives inputs from various receptors around the body and sends output through two nerves to the muscles around the lungs. The respiratory centre depends on information relayed via chemoreceptors that pick up changes in: carbon dioxide concentration – levels in the blood go up when the rate of respiration increases and more carbon dioxide is produced as a waste product. Oxygen concentration – levels in the blood go down as it is used in respiration to produce extra ATP as an energy source for exercise. The chemoreceptors are stimulated by a rise in carbon dioxide levels and a fall in pH and oxygen in the blood. The respiratory centre received the information as a nerve impulse from the chemoreceptors and uses this to regulate breathing. Later in this module we will be look in more detail about the effects of exercise and how the breathing rate and heart rate is controlled via various changing conditions within the body. How does the respiratory centre control ventilation? [back to top] Unlike the heart, the muscles that cause breathing cannot contract on their own, but need nerve impulses from the brain for each breath. The respiratory centre transmits regular nerve impulses to the diaphragm and intercostal muscles to cause inhalation. Stretch receptors in the alveoli and bronchioles detect inhalation and send inhibitory signals to the respiratory centre to cause exhalation. This negative feedback system in continuous and prevents damage to the lungs. One difference between ventilation and heartbeat is that ventilation is also under voluntary control from the cortex, the voluntary part of the brain. This allows you to hold your breath or blow out candles, but it can be overruled by the autonomic system in the event of danger. For example if you hold your breath for a long time, the carbon dioxide concentration in the blood increases so much that the respiratory centre forces you to gasp and take a breath. Pearl divers hyperventilate before diving to lower the carbon dioxide concentration in their blood, so that it takes longer to build up. During sleep there is so little cellular respiration taking place that it is possible to stop breathing for a while, but the respiratory centre starts it up again as the carbon dioxide concentration increases. It is possible that one cause of cot deaths may be an underdeveloped respiratory centre in young babies, which allows breathing to slow down or stop for too long.