Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Hospital-acquired infection wikipedia , lookup
Schistosomiasis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neonatal infection wikipedia , lookup
West Nile fever wikipedia , lookup
Marburg virus disease wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Henipavirus wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
Potato virus Y wikipedia , lookup
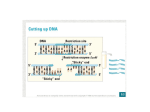
Hepatitis B Properties: HBV is a member of hepadnavirus family. It is 42 nm enveloped virion (also known as "Dane particles") contain a partially circular doublestranded DNA genome. The envelope contains a protein called surface antigen (HBsAg). Within the core is a DNA-dependent DNA polymerase. Also there are two other antigens: core antigen (HBcAg) and e antigen (HBeAg). Electron microscopy of HBsAg-positive serum reveals three morphologic forms (figure 1). The most numerous are spherical particles measuring 22 nm in diameter and small particles are made up exclusively of HBsAg––as are tubular or filamentous forms, which have the same diameter but may be over 200 nm long. Figure (1): Hepatitis B virus. 1 Replication: After the HBV has attached to the cell surface receptor, the viral membrane fuses with the cell membrane releasing the core into the cytoplasm. The core proteins dissociate from the partially double stranded DNA. DNA polymerase now completes the DNA so that it is completely double stranded. The double stranded DNA enters the nucleus and the viral DNA associates with host nuclear histones, then it is transcribed by cellular RNA polymerase II into mRNAs. In contrast to the situation with retroviruses, however, the DNA form of HBV is usually not integrated into cellular DNA. The mRNA codes for the polymerase and core HBcAg and HBeAg proteins. Inside the core, the RNA is transcribed to minus strand DNA by the same DNA polymerase (reverse transcriptase) that completed the double stranded DNA. The virus now buds through the endoplasmic reticulum and/or Golgi Body membranes (or perhaps a novel pre-Golgi compartment) of the host cell from which it acquires HBsAg. At this stage or later, the minus stand of DNA is partly transcribed into a plus strand. When the viral DNA polymerase is used to transcribe RNA to DNA, it is acting as a reverse transcriptase similar to that found in retroviruses; in fact, HBV DNA polymerase and retroviral reverse transcriptase are very similar, and may have evolved from a common ancestor. Epidemiology and transmission: World-wide in distribution, there are 450 million persistent carriers of hepatitis B, 50 million of which are in Africa. Carriage rates vary markedly in different areas. There are three mains mode of transmission are: via blood (blood transfusions, serum products, sharing of needles, 2 razors, acupuncture and organ donation); sexual intercourse and horizontal transmission (in children, families, 'close personal contact) or vertical transmission (perinatal transmission from a carrier mother to her baby). Pathogenesis Infection is parenterally transmitted. The virus replicates in the liver and virus particles, as well as excess viral surface protein, are shed in large amounts into the blood. Viraemia is prolonged and the blood of infected individuals is highly infectious. Following acute infection, approximately 5% of infected individuals fail to eliminate the virus completely and become persistently infected. The virus persists in the hepatocytes and on-going liver damage occurs because of the host immune response against the infected liver cells. Chronic infection may take one of two forms: Chronic persistent Hepatitis - the virus persists, but there is minimal liver damage Chronic Active Hepatitis - There is aggressive destruction of liver tissue and rapid progression to cirrhosis or liver failure. Patients who become persistently infected are at risk of developing hepatocellular carcinoma (HCC). Clinical Features: Insidious onset of symptoms tends to cause a more severe disease than Hepatitis A. Many HBV infections are asymptomatic infections. The incubation period is 10-12 weeks. The clinical appearance of acute 3 hepatitis B tends to be sever, and life threatening hepatitis can occur (figure 2). Symptoms anti-HBe HBeAg Total anti-HBc Titre 0 4 anti-HBs IgM anti-HBc HBsAg 8 12 16 20 24 28 32 36 52 100 Weeks after Exposure Figure (2): acute hepatitis B with recovery (typical serological course). Diagnosis: Serological tests are used for the diagnosis of acute and chronic hepatitis B infection. HBsAg - used as a general marker of infection. HBsAb - used to document recovery and/or immunity to HBV infection, is not found in chronic carriers. Anti-HBc IgM - marker of acute infection. Anti-HBcIgG - past or chronic infection. HBeAg - indicates active replication of virus and therefore infectiveness. 4 Anti-Hbe - virus no longer replicating. It indicates low infectivity in a carrier. Treatment and prevention: Alpha interferon is clinically useful for the treatment of chronic active hepatitis. Lamivudine - a nucleoside analogue reverse transcriptase inhibitor, reduce hepatic inflammation and lower the levels of HBV in chronic carriers. Prevention by; highly effective recombinant vaccines are now available, or hepatitis B immunoglobulin - HBIG may be used to protect persons who are exposed to hepatitis B. 5