Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropharmacology wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Development of analogs of thalidomide wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Psychopharmacology wikipedia , lookup
Discovery and development of cephalosporins wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Theralizumab wikipedia , lookup
Discovery and development of proton pump inhibitors wikipedia , lookup
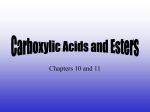
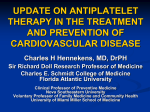
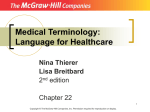
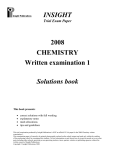
PLATELETS AND VASCULAR OCCLUSION Pharmacology of platelet inhibition in humans: implications of the salicylate-aspirin interaction GIOVANNI DE GAETANO, M.D., PH.D., CHIARA CERLETTI, PH.D., ELISABETrA DEJANA, PH.D., ROBERTO LATINI, M.D. AND Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 ABSTRACT The current dispute over the effects of "low" vs "high"doses of aspirin should take into consideration the pharmacokinetics of this drug. In fact, different pharmaceutical formulations of aspirin may deliver little or no aspirin to the systemic blood. This was the case, for instance, in healthy volunteers taking 320 mg of compressed aspirin or 800 mg of enteric-coated aspirin. In all instances thromboxane B2 generation in serum was fully inhibited. Platelet cyclooxygenase might therefore be effectively acetylated by exposure to aspirin in the portal circulation, whereas vascular cyclooxygenase could be spared. Thus aspirin formulations ensuring complete first-pass deacetylation should be sought rather than "low" or "high" doses of unspecified aspirin formulations. Regardless of the type and dose of aspirin administered, salicylate is formed and accumulates in the circulation. It may antagonize the effects of aspirin on cyclooxygenase, at least in acute conditions. As an example, after administration of 1 g of salicylate to healthy volunteers, when plasma levels of the drug were about 75 ,ug/ml, the effect of 40 mg iv aspirin (given 40 min later) on platelet cyclooxygenase and aggregation was significantly diminished. In contrast, in patients undergoing saphenectomy, the same dose of salicylate (1 g) gave plasma drug levels of about 25 ,ug/ml; salicylate was unable to prevent the inhibitory effect on platelets of 40 mg iv aspirin (given 1 hr later) but did act on vascular prostacyclin. Thus the combination of salicylate with aspirin at an appropriate dose and blood level ratio may result in almost complete dissociation of the drug's effect on platelets and vessels in man. Because the studies outlined in this review address only the short-term outcome of the salicylate-aspirin interaction, the possibility should be tested that inactivation of cyclooxygenase would occur after long-term administration of salicylate-aspirin. A pharmacokinetic approach to the "aspirin dilemma" should also consider the possibility that salicylate and/or its metabolites (e.g., gentisic acid) may interfere with lipoxygenase activity, synthesis of the prothrombin complex coagulation factors, and fibrinolysis. Circulation 72, No. 6, 1185-1193, 1985. Aspirin, salicylate, and inhibition of platelet aggregation and cyclooxygenase activity. Aspirin inhibits platelet aggregation and the concomitant release reaction.I4 This exciting discovery, made more than 15 years ago, was characterized by three main facts: (1) aspirin was active in man at oral doses as low as 150 mg (about 2 mg/kg), (2) its effects were long lasting (at least 24 to 48 hr), and (3) salicylate, the main metabolite of aspirin, was virtually inactive. The last two observations suggested that the effect of aspirin on platelets was the result of irreversible acetylation. Consequently, the salicylate moiety of aspirin was considered irrelevant for the drug's action on platelets. From the Laboratory of Cardiovascular Clinical Pharmacology, Istituto di Ricerche Farmacologiche Mario Negri, Milano, Italy. Supported by the Italian National Research Council, Progetto Finalizzato "Medicina Preventiva," Sottoprogetto "Malattie Degenerative," Contract No. 84.02277.56. Address for correspondence: Giovanni de Gaetano, M.D., Ph.D. ,Laboratory of Cardiovascular Clinical Pharmacology, Istituto di Ricerche Farmacologiche Mario Negri, via Eritrea, 62-20157 Milano, Italy. Vol. 72, No. 6, December 1985 In the early seventies, aspirin and other nonsteroidal anti-inflammatory drugs (NSAID) were shown to inhibit prostaglandin formation in human platelets.5 Again salicylate was inactive. Acetylation of platelet proteins by aspirin was subsequently reported.6 Because one of these proteins was a subunit of fatty acid cyclooxygenase, the role of this enzyme in the aspirin action was considered to be crucial. Although the nonspecific acetylation of other platelet proteins is currently of unknown biological significance, the inhibition of cyclooxygenase by aspirin does not appear to explain fully the antithrombotic effects of this drug.]10 Aspirin is quickly deacetylated in vivo to salicylate. It has been suggested that in sites readily accessible to aspirin, such as circulating platelet cyclooxygenase, it might be expected to act in its own right as the acetylsalicylate ion and hence to be more potent than salicylate.7 It would also be expected that the salicylate ion, into which aspirin is converted, would contribute to the overall activity of aspirin, for instance in actions that 1185 DE GAETANO et al. need persistent presence of an anti-inflammatory drug or that are located at poorly accessible sites; this might apply for example in rheumatic joints.7 Additionally, salicylate may antagonize some effects of aspirin, such as its gastrointestinal ulcerogenicity."1 Our aim in this article is to review the available evidence on (1) the occurrence and the possible clinical relevance of the interaction between salicylate (or other NSAID) and aspirin on platelet and vascular cyclooxygenase and (2) the existence of additional mechanism(s) related to salicylate and possibly involved in the antithrombotic effects of aspirin. Salicylate may antagonize the effects of aspirin on cyclooxygenase Salicylate-aspirin or other NSAID-aspirin interactions on animalplatelet cyclooxygenase. Studies in vitro have demDownloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 onstrated that salicylate, which is not inhibitory by itself, protects cyclooxygenase from aspirin inhibition in rat'2 and rabbit'3 platelets (figure 1). A similar pharmacologic interaction was apparent in vivo. 14 1' In the rat, administration of salicylate resulted in dose-related prevention of aspirin's effect on platelet cyclooxygenase activity. This interaction appeared to be competitive and closely dose related for both drugs.'5 Other NSAID structurally related or unrelated to salicylate, such as diflunisal and sulphinpyrazone, respectively, are able in the rat in vivo to counter the effect of aspirin on platelets.'5 This effect was apparent for diflunisal or sulphinpyrazone at doses that did not inhibit platelet cyclooxygenase. The prevention by indomethacin of the effect of aspirin on platelets was apparent 24 hr after administration of aspirin. Actually the effect of indomethacin on platelet cyclooxygenase is short lasting, whereas that of aspirin lasts at least 24 hr. When the two drugs were given concurrently, the lasting effect of aspirin was no longer detectable and inhibition of cyclooxygenase lasted as if indomethacin alone had been administered. On the other hand, salicylate and diflunisal competitively blunted the inhibitory effect of indomethacin on platelet cyclooxygenase. All these results could be explained by postulating a common site of interaction for the different NSAID on cyclooxygenase.'5 16 The observation that salicylate, a virtually inactive compound or ineffective doses of diflunisal and sulphinpyrazone counteract the effect of aspirin suggests that competition does not occur at the catalytic site but rather at a supplementary binding site. Interaction with this putative supplementary site is necessary but not sufficient for the efficacy of these drugs as cyclooxygenase inhibitors.'5' 16 Thus salicylate interacts with the binding site of cyclooxygenase but does not modify its enzymatic activity. However, neither aspirin nor indomethacin can exert their inhibitory activity on the enzyme when the binding site is occupied by salicylate. Further experimental evidence of a supplementary binding site on cyclooxygenase was provided by the failure of salicylate to prevent enzyme inhibition by 5,8,11,14-eicosatetraynoic acid (ETYA), a competitive antagonist of arachidonic acid. Moreover, salicylate did not affect either ETYA or nor-dihydroguaiaretic acid inhibition of platelet lipoxygenase. On the basis of these and other data presented in detail elsewhere, 17 a functional model of pharmacologic inhibition of cyclooxygenase by aspirin and other NSAID can be proposed (figure 2). This model would explain the selectivity of NSAID for the cyclooxygen- z 0 (/) (I i LI) z OX A AA AA a.- -J (D CONTROL SALICYLATE ASA SAL I C YLATE +ASA FIGURE 1. Prevention by salicylate of aspirin inhibition of arachidonic acid-induced platelet aggregation. Rat platelet aggregation was induced by threshold concentrations of arachidonic acid (AA 0.5 mM). Aspirin (100 jM) preincubation (1 min) with PRP completely prevented aggregation, whereas sodium salicylate (1 mM) 1 min before was ineffective. The combination of both compounds resulted in an almost normal aggregation. ASA = aspirin; PRP = platelet-rich plasma. 1186 CIRCULATION PLATELETS AND VASCULAR OCCLUSION ARACHIDONIC ACID SALICYLATE BINDING SITE CATALYTIC SITES CYCLO-OXYGENASE L IPOXYGENASE FIGURE 2. Functional model of cyclooxygenase and lipoxygenase inhibition. Salicylate, aspirin, and the other NSAIDs bind to a binding site related to but distinct from the catalytic site of cyclooxygenase. This binding is necessary but not sufficient for enzyme inhibition. 5,8,11,14-Eicosatetraynoic acid (ETYA) competes with arachidonic acid for the catalytic sites of both cyclooxygenase and lipoxygenase. Thus salicylate does not interfere with the effect of ETYA. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 ase pathway of arachidonic acid metabolism in relation to lipoxygenase. I6J 17 The intensity of interaction with the supplementary site and the ensuing modifications of the catalytic site would determine these compounds' potency as cyclooxygenase inhibitors. This model might also account for the finding that salicylate, aspirin, and indomethacin equipotently inhibit the lipoxygenase pathway.'8 Recently, additional evidence for two distinct enzymatic sites on rabbit platelet cyclooxygenase has been presented.19 Salicylate-aspirin interaction on animal vascular cyclooxy- genase. The interaction between salicylate and aspirin is not restricted to platelet cyclooxygenase.'2 In fact, salicylate administered to rats may prevent the inhibitory activity of aspirin on vascular cyclooxygenase.20 This effect was even more evident than that on platelets. Indeed the doses of salicylate needed to completely counteract the effect of the same dose of aspirin on vascular cyclooxygenase were lower than those on platelets. As a direct consequence of this observation, the administration of salicylate and aspirin at appropriate dose ratios could achieve complete inhibition of platelet cyclooxygenase without affecting the vascular enzyme. Whether the different efficacy of salicylate in preventing aspirin effect derives from a different sensitivity to or access of the drug at various cellular levels remains to be established. Salicylate-aspirin interaction at other cellular levels in animals. In the guinea pig, salicylate, inactive by itself, prevents the protective effect of aspirin in arachidonic acid-induced bronchoconstriction in vivo.21 Because this arachidonate effect was not mediated by platelet aggregation but most likely by endoperoxide and thromboxane A2 (TxA2) production by the lung, the Vol. 72, No. 6, December 1985 salicylate-aspirin interaction could occur in the lungs. It has been reported that salicylate diminishes the gastric lesions induced by aspirin and other NSAID in rats." This effect seems to be secondary to a depression of prostaglandin synthesis in the stomach, and the counteracting effect of salicylate was correlated to its ability to protect gastric cyclooxygenase from NSAID inhibition.1"1 22 Salicylate-aspirin interaction on human platelet cyclooxy- genase. All the above data have been obtained in vitro or in vivo in animal studies. Interference by salicylate with aspirin inhibition of human platelet cyclooxygenase activity has also been observed.2-25 The question remains as to whether a similar interaction occurs between salicylate and other NSAID on cyclooxygenase in vivo in man and as to its clinical relevance. In a recent study in human volunteers we observed that orally administered indomethacin (50 mg) prevented the long-lasting effect of a subsequent dose of aspirin (500 mg) on platelet cyclooxygenase activity and on platelet aggregation.25 Similarly, ingestion of ibuprofen prevented the aspirin effect.26 More recently we investigated whether salicylate and aspirin interact on platelets in man at doses and plasma levels of clinical relevance.27 Six volunteers, given oral doses of sodium salicylate (250 or 1000 mg) presented peak plasma salicylate levels averaging 20 and 75 ,ug/ml, respectively. Neither platelet aggregation nor serum immunoreactive thromboxane B2 (TxB2) formation was modified by either salicylate treatment. Forty minutes later, all volunteers received 40 mg iv aspirin, the lowest single dose that suppressed arachidonate-induced platelet aggregation and TxB2 generation. Aspirin plasma levels were not affected by previous salicylate ingestion. Inhibition by aspirin of both platelet 1187 DE GAETANO et al. aggregation and TxB2 generation was significantly prevented by the larger salicylate dose, giving plasma salicylate levels similar to those after an oral dose of 800 mg of enteric-coated aspirin. Pretreatment with 250 mg of salicylate, giving plasma salicylate levels similar to those obtained with an oral dose of 320 mg of compressed aspirin, resulted in proportionally diminished prevention of aspirin's effect on platelet aggregation but did not significantly modify its effect on serum TxB2 generation. Salicylate-aspirin interaction in man as a possible pharma- TABLE 1 Effect of aspirin and salicylate on immunoreactive serum TxB2 and vascular 6-keto-PGF,a generation in 21 patients undergoing saphenectomy cologic solution to the "aspirin dilemma." When it was Ap < .01 compared with the other two groups (Duncan's test). 6Keto-PGF,a was measured by specific radioimmunoassay in the supernatant of epigastric segments of saphenous vein incubated for 5 min with arachidonic acid (50 ttM), as described.3' Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 shown that aspirin, while inhibiting TxA2 in platelets, equally inhibited antiaggregatory prostacyclin (PGI2) in vascular cells, the "aspirin dilemma" emerged.28 29 Simultaneous inhibition of PGl2 and TxB2 synthesis was considered a possible reason for the disappointing results of clinical trials on the drug's antithrombotic effect.8 In an effort to solve the "aspirin dilemma," studies were devised to determine the aspirin dose that would inhibit TxA2 production but would not interfere with PGI2 synthesis in vascular cells. Platelet cyclooxygenase was believed to be more sensitive than vascular cyclooxygenase to aspirin inhibition. If it had been, the "aspirin dilemma" could have been solved easily by using low doses of the drug. Unfortunately, studies with endothelial cells in culture, laboratory animals, and man have not completely dissociated the inhibitory effect of aspirin on platelets from that on vascular cells (for review see refs. 8 and 30). We have already mentioned that in the rat, salicylate was more effective in counteracting the inhibitory activity of aspirin on vascular cyclooxygenase than that on platelet cyclooxygenase.20 We have recently completed a study3' in patients undergoing saphenectomy, aimed at verifying a similar differential salicylate-aspirin interaction in man. Twenty-one female patients, admitted to the Milan- University Institute of Vascular Surgery for removal of varicose veins, entered this study. Seven took no medications, and six were given 40 mg iv aspirin 1 hr before operation. The remaining eight patients took 1000 mg sodium salicylate orally 1 hr before aspirin. During surgery, segments of epigastric vein in close proximity to the saphenous vein were removed for measurements of prostacyclin production. At the same time, venous blood was collected for measurements of serum TxB2 synthesis. As reported in table 1, TxB2 generation was completely inhibited in all patients given aspirin alone, whereas prostacyclin generation was reduced by more than 50%. In the salicylate-aspirin group, TxB2 gen1188 Vascular Treatment Control Aspirin (40 mg iv) Salicylate (1 g po) + aspirin nd = 6-keto-PGF,, n Serum TxB2 (pmol/ml) 7 6 8 44.8+4 nd 4.3+1 2.73±0.2 1.18 ± 0.2A 2.11 ±0.2 (pmollmg) not detectable (<0.075 pmol/ml). eration remained undetectable in three patients and reached about 10% of control values in the other five. In contrast, six patients generated prostacyclin levels within the control range and only two appeared to be partially inhibited. Mean salicylate blood levels at the moment of aspirin administration were 25.9 + 5 jug/ml. This observation confirms in man the results obtained in the rat. In this animal as well as in the present study in man, vascular cells showed lower sensitivity to aspirin than platelets. Salicylate resulted in both instances in an amplification of the difference in response to aspirin of platelets and vascular cells. The mechanism of this property of salicylate (e.g., different access of the drug at various cellular levels) remains to be defined. This observation, however, may constitute an original approach on which to base the clinical use of aspirin in a supposedly beneficial antithrombotic direction. When analyzed with respect to the study in healthy male volunteers, this study in female patients undergoing saphenectomy merits some comments. As summarized in table 2, the same salicylate-aspirin dose ratio (1000 mg oral vs 40 mg iv) resulted in significant prevention of the aspirin effect on platelet TxB2 generation in the group of volunteers but not in patients. The most likely explanation is that at the moment of aspirin administration, the plasma levels of salicylate, measured 1 hr after ingestion (abut 25 ,g/ml), were markedly lower than those measured 40 min after ingestion in volunteers (about 75 gg/ml). In fact, salicylate levels in patients were similar to those found in volunteers 40 min after 250 mg of salicylate. In the latter condition, as well as in patients, no significant prevention of aspirin's effect on TxB2 synthesis could be detected. Possibly, gastrointestinal absorption of salicylate was reduced in patients by anesthesia. CIRCULATION PLATELETS AND VASCULAR OCCLUSION TABLE 2 Salicylate-aspirin interaction at platelet and vascular level and plasma salicylate levels in healthy volunteers and in patients undergoing saphenectomy Subjects Volunteers Volunteers Saphenectomy patients Salicylate levels SAL/ASA interaction TxB2 PGI2 Salicylate (mg, oral) Interval (min) 250 1000 40 40 22.3 ± 1.7 76.3 ± 5.1 No Yes 1000 60 25.9 ± 5.0 No (,uglml) Yes SAL = salicylate; ASA = aspirin. Plasma salicylate levels were measured immediately before aspirin (40 mg iv). For other details see table 1. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Independently of the reasons why the same dose of salicylate gave rise to different plasma levels of the drug in the two groups of subjects, it appears that the plasma levels of salicylate rather than the amount of the drug administered are relevant for an optimal interaction with aspirin. In summary, we have discussed the hypothesis that platelet and/or vascular cyclooxygenase might be spared acetylation by aspirin if the plasma levels of salicylate are carefully balanced with the plasma levels of aspirin. This hypothesis has been tested experimentally both in vitro and ex vivo in short-term animal and human studies. Protection of cyclooxygenase with salicylate acutely prevented irreversible inactivation by aspirin; experimental evidence that salicylate protects cyclooxygenase from inactivation by aspirin after long-term administration of both compounds is still lacking. Cyclooxygenase protection by salicylate might slow the rate of its inactivation by aspirin but not prevent it completely; thus the cyclooxygenase population might be finally inactivated during long-term salicylate-aspirin therapy, despite a careful balance between salicylate and aspirin levels. On the basis of these considerations we addressed our attention to another possible approach to solve the "aspirin dilemma." pirin after either 320 mg of compressed aspirin or 800 mg of enteric-coated aspirin were not statistically different (2.9 ± 0.06 and 3.3 ± 0.3 gg/ml, respectively). Serum TxB2 generation was almost completely inhibited 1 hr after either aspirin formulation. Of even greater interest was the observation that similar full TxB2 inhibition was obtained in five volunteers in whose peripheral circulation aspirin levels were not measurable (figure 3). Three subjects had received a compressed aspirin and two an enteric-coated aspirin. No significant differences in salicylate area under the plasma concentration vs time curve could be found between subjects with detectable or undetectable aspirin plasma levels after either formulation (table 3). On account of the potential for erratic absorption pattern of aspirin, detectable plasma levels of the unchanged drug may depend on fortuitous blood collection times.32 In our study, however, this was unlikely because as many as eight blood samples were collected within the first hour after compressed aspirin and six 100- 320 mg COMPRESSED ASA DETECTABLE oJ ASA N. D. 0 z os50 0 0 -_-L 10min 0m 10 lh 30m 800 mg 24h 4h ENTERIC-COATED ASA DETECTABLE AS A N.D0. _J z o so0 Aspirin formulations that deliver only salicylate to the systemic circulation: a pharmacokinetic approach to the "aspirin dilemma." The importance of salicylate plasma levels mentioned in the preceding section suggests that a better knowledge of the pharmacokinetics of aspirin might help solve the "aspirin dilemma." Little attention has been paid to aspirin pharmacokinetics with regard to the different pharmaceutical formulations used in thrombosis prevention trials. This approach seemed of particular interest in view of observations in healthy volunteers27 that the peak plasma levels of asVol. 72, No. 6, December 1985 10min FIGURE 3. Serum 320 mg of h TxB2 2 4h measured at different times after compressed (upper panel) or ingestion of 800 mg of enteric-coated (lower panel) aspirin in subjects with detectable or undetectable aspirin levels. Figures are percent values of predrug serum TxB2 in each subject and SEM. Three subjects had detectable and three undetectable aspirin plasma levels after 320 mg aspirin, while four had detectable and two undetectable aspirin plasma levels after 800 mg enteric-coated aspirin. In this last group the mean and the two single values are reported, respectively. ASA = aspirin; ND = not detectable. 1189 DE GAETANO et al. TABLE 3 Pharmacokinetics of aspirin after ingestion of two diferent drug formulations in six healthy volunteers AUC (0o, Aspirin (nmol/ml/hr) preparation (oral dose) n Aspirin Salicylate Compressed (320 mg) 3 3 4 2 17.3±1.4 undetectable 31.9 ± 3.3 undetectable 544 ±-42 830 ± 40 2680 +153 2190-2851 Enteric-coated (800 mg) AUC = area under the plasma concentrations between 0 and m. Detection limit of aspirin = 0.5 nmol/ml. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 during the first 3 hr after enteric-coated aspirin. The time of peak aspirin concentration in subjects in whom it was detectable was 33 min for compressed and 83 min for enteric-coated aspirin.27 Experiments in vitro showed that incubation of human whole blood from three different donors with 0.5 ,.tM aspirin (corresponding to the detection limit of the high-performance liquid chromatographic assay method used) for 1 hr at 370 C did not result in any significant reduction of serum TxB2 generation. As shown in figure 4, concentrations of aspirin at least 50 times this detection limit were required to prevent TxB2 generation by more than 90%. It has long been known that aspirin undergoes extensive first-pass deacetylation within the enterohepatic circulation.33 Whether this first-pass effect is dosedependent is not yet known. Thus inhibition of serum TxB2 generation in the absence of measurable aspirin in systemic peripheral blood might result from acetylation of platelet cyclooxygenase by exposure of circulating cells to the drug in the portal circulation. Cyclooxygenase in the peripheral vasculature could thus come into contact only with inactive salicylate, with the possible exception of the mesenteric and portal 100* *0 5 0 vessels exposed to aspirin before the first-pass occurs. Thus aspirin formulations ensuring extensive firstpass deacetylation rather than merely "low" or "high" doses of unspecified aspirin formulations should be sought as a pharmacologic goal for solving the "aspirin dilemma." The current dispute on the difference in sensitivity to "low" doses of aspirin between platelet and vascular cyclooxygenase may well arise from the wide variability of aspirin pharmacokinetics. Indeed, as in our experiments, the same dose or formulation may or may not deliver measurable amounts of aspirin to the systemic circulation; the inhibitory effect on platelet cyclooxygenase would be achieved in any case, but vascular PGI2 synthesis would only be spared in the absence of detectable peripheral aspirin levels. Similar conclusions have recently been reached by other investigators.", 35 Salicylate may contribute to the overall activity of aspirin in the prevention of vascular occlusion. Although inhibition of prostanoid synthesis has become an attractive, unifying explanation of the anti-inflammatory activity of aspirin-like drugs, this mechanism does not explain all aspects of the anti-inflammatory action of salicylates, especially in conditions in which aspirin and salicylate are of approximately equal potency.7 It has therefore been suggested that the anti-inflammatory activity of aspirin-like drugs probably does not arise from a single mechanism but may be mediated through an additional or alternative mechanism, which becomes operative only at doses in excess of those required to suppress cyclooxygenase. The possibility has also been discussed that aspirin has additional components to its mechanism of action not possessed by other NSAIDs, such as flufenamic acid or indomethacin. The major lines of research into alternative mechanisms that might explain the therapeutic action of sa- licylate have been reviewed extensively.7 Because several pathways may be involved in the initiation and growth of thrombi, one would expect aspirin to be inhibitory only in conditions in which prostanoid biosynthesis (cyclic endoperoxides and TxA2) plays a major role in thrombus formation. Effects of aspirin and salicylate on blood coagulation and z 0 -x v .X r 0.5 1 - 2.5 5 10 25 50 100 [AiM] Aspi rin FIGURE 4. Effect of different aspirin concentrations on TxB2 generation in human serum in vitro. Blood was collected without anticoagulant from the antecubital vein of healthy subjects and incubated in glass tube at 370 C for 1 hr in the presence of aspirin. TxB2 generation was measured in serum. The values (mean from four experiments) are percent inhibition of control values. 1190 fibrinolysis. A recent study9 in rabbits with in-dwelling aortic catheters strongly suggests that aspirin at doses that inhibit only platelet cyclooxygenase activity is not a satisfactory inhibitor of arterial thrombosis when there is a significant fibrin component. At very high doses aspirin inhibited thrombosis, but this effect was not mediated through inhibition of platelet function. In fact salicylate was more effective than aspirin. The tendency for high doses of aspirin or salicylate to inCIRCULATION PLATELETS AND VASCULAR OCCLUSION Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 hibit thrombus formation appears related to a prolongation of the one-stage prothrombin time and to activation of whole blood fibrinolytic activity; which of these pathways is most important in reducing thrombus formation remains to be established. This experimental finding is in keeping with some observations in man. There are reports that doses of 2 to 3 g of aspirin per day in man prolong prothrombin time36 37 and increase whole blood fibrinolytic activity.3 -0 Moroz39 reported that aspirin and sodium salicylate (1.8 g) were equipotent in stimulating fibrinolytic activity through the protease action of leukocytes. The beneficial effect of high doses of aspirin in preventing venous thrombosis and pulmonary embolism after total knee replacement41 may be due not just to the effect of aspirin on platelets but also to its effect (and/or of the salicylate) on blood coagulation and fibrinolysis. However, in a recent study on healthy human volunteers, aspirin (650 mg given orally both 18 and 2 hr before blood collection) inhibited the rise in vascular plasminogen activity after venous occlusion.42 Similarly a decrease in fibrinolysis induced by both cellular and plasmatic factors after ingestion of 1 g of aspirin per day for 4 days had been reported.43 Recently Roncaglioni et al.4 have shown in rats that salicylate, like warfarin, with which it may have some common chemical features (figure 5), reduced the plasma concentration of the prothrombin complex clotting factors in vivo. It also caused an accumulation of microsomal substrates for vitamin K-dependent carboxylase in the liver and lung. These effects of salicylate were dose-dependent (between 4 x 50 and 4 x 200 mg/kg) and were counteracted by simultaneous administration of vitamin K (20 mg/kg). The mechanism of salicylate-induced hypoprothrombinemia in the rat and in the rabbit has been extensively investigated by several groups.45-48 Because the effect of sa- OH 0 0 licylate was additive to that of warfarin,44 relatively low doses of aspirin or salicylate should interfere with oral anticoagulant therapy. Aspirin-induced fluctuation in clotting factor levels of as little as 5% to 10% of normal might have serious consequences in patients undergoing anticoagulant treatment, although it might not even be measurable in healthy volunteers. These considerations should be borne in mind when analyzing the results of clinical trials combining aspirin and oral anticoagulants. On the one hand it is not surprising that this drug combination has been reported to be more effective than oral anticoagulants alone in preventing thrombotic complications in patients with aortic ball valves.49 On the other hand it could explain the high frequency of bleeding complications encountered in other trials.50 Two recent reports in rabbits5" and in rats52 have suggested that high doses of aspirin may prolong bleeding time independently of an effect on platelet cyclooxygenase and also of formation of salicylate. Effects of aspirin and salicylate on leukocytes. The observation that aspirin and salicylate equipotently inhibit the generation of chemotactic 12-HETE from 12HPETE in the lipoxygenase pathway of the arachidonic acid metabolism,18 although controversial, has been considered as diminishing the importance of the cyclooxygenase pathway in the anti-inflammatory activity of salicylate.7 A key event in any inflammatory reaction is the migration of leukocytes from the blood into the inflammatory lesion. Leukocytes metabolize arachidonic acid by lipoxygenase53 and the products of this enzyme are potent chemotactic agents54 that induce leukocyte aggregation.55 56 It has recently been proposed57 that migrating leukocytes contribute to the tissue injury accompanying myocardial ischemia, possibly by release of proinflammatory mediators and free radicals 0 DY ~~~~~F Rh FIGURE 5. Chemical structures of salicylate and warfarin. OH SALICYLIC ACID Vol. 72, No. 6, December 1985 OH CH2COCH3 WARFARIN 1191 DE GAETANO et al. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 (oxygen metabolites). Drugs that reduce the migration and/or activation of leukocytes might be useful in reducing infarct size. Aspirin and salicylate inhibit the production of superoxide anion by activated leukocytes7 but do not reduce leukocyte invasion into an inflammatory exudate.58 Thus, although an interaction with superoxide anion could be considered as a possible additional mechanism of the anti-inflammatory action of salicylates, the biological consequences of this pharmacologic effect are not obvious. A recent observation in our laboratory (A. Lorico and S. Villa, unpublished) may also be of interest in this context: gentisic acid,59 a hydroxylated metabolite of salicylate, not only prevented superoxide anion production by human leukocytes stimulated with either arachidonic acid or phorbol myristate acetate, but also prevented leukocyte aggregation. The concentrations of gentisic acid active in vitro (0.4 to 1.2 mM) are probably not reached in the human circulation after current therapeutic doses of aspirin.60 However, this finding merits further investigation. Conclusions. Aspirin inhibits cyclooxygenase. This effect distinguishes it from salicylate, its major metabolite, with regard to inhibition of the platelet function induced by certain stimuli. Although inactive on cyclooxygenase, salicylate may interfere with the effect of aspirin on this enzyme both in platelets and (even more effectively) in the vasculature. Knowledge of the pharmacokinetics of aspirin and salicylate is essential for optimal use of aspirin as a selective inhibitor of platelet but not of vascular cyclooxygenase activity. The mechanism involving cyclooxygenase does not, however, appear to fully explain the antithrombotic action of aspirin. Therefore, it is best to assume that in preventing thrombosis aspirin acts by at least two mechanisms, one of which is the inhibition of platelet cyclooxygenase. The best candidate mechanisms, most likely to be linked to the salicylate moiety of aspirin, are the inhibition of vitamin K-dependent clotting factor synthesis, cell-mediated activation of blood fibrinolysis, and interference with the platelet and/or leukocyte lipoxygenase pathway of arachidonic acid metabolism. 3. O'Brien JR: Effects of salicylates on human platelets. Lancet 1: 779, 1968 4. Zucker MB, Peterson J: Inhibition of adenosine diphosphate-induced secondary aggregation and other platelet functions by acetylsalicylic acid ingestion. Proc Soc Exp Biol Med 127: 547, 1968 5. Smith JB, Willis AL: Aspirin selectively inhibits prostaglandin production in human platelets. Nature New Biol 231: 235, 1971 6. Roth GJ, Stanford N, Majerus PW: Acetylation of prostaglandin synthase by aspirin. Proc Natl Acad Sci USA 72: 3073, 1975 7. Atkinson DC, Collier HOJ: Salicylates: molecular mechanism of therapeutic action. Adv Pharmacol Chemother 17: 233, 1980 8. de Gaetano G, Cerletti C, Berteld V: Pharmacology of antiplatelet drugs and clinical trials on thrombosis prevention: a difficult link. Lancet 2: 974, 1982 9. Cattaneo M, Chahil A, Somers D, Kinlough-Rathbone RL, Packham MA, Mustard JF: Effect of aspirin and sodium salicylate on thrombosis, fibrinolysis, prothrombin time, and platelet survival in rabbits with indwelling aortic catheters. Blood 61: 353, 1983 10. Marcus AJ: Aspirin as an antithrombotic medication. N Engl J Med 309: 1515, 1983 11. Ezer E, Palosi E, Hajos Gy, Szpomy L: Antagonism of the gastrointestinal ulcerogenic effect of some non-steroidal anti-inflammatory agents by sodium salicylate. J Pharm Pharnmacol 28: 655, 1976 12. Merino J, Livio M, Rajtar G, de Gaetano G: Salicylate reverses in vitro aspirin inhibition of rat platelet and vascular prostaglandin generation. Biochem Pharmacol 29: 1093, 1980 13. Vargaftig BB: The inhibition of cyclo-oxygenase of rabbit platelets by aspirin is prevented by salicylic acid and by phenanthrolines. Eur J Pharmacol 50: 231, 1978 14. Vargaftig BB: Salicylic acid fails to inhibit generation of thromboxane A2 activity in platelets after in vivo administration to the rat. J Pharm Pharmacol 30: 101, 1978 15. Cerletti C, Livio M, de Gaetano G: Non-steroidal anti-inflammatory drugs react with two sites on platelet cyclo-oxygenase: evidence from in vivo drug interaction studies in rats. Biochim Biophys Acta 714: 122, 1982 16. Humes JL, Winter CA, Sadowski SJ, Kuehl FA Jr: Multiple sites on prostaglandin cyclooxygenase are determinants in the action of nonsteroidal antiinflammatory agents. Proc Natl Acad Sci USA 78: 2053, 1981 17. Cerletti C, Livio M, Doni MG, de Gaetano G: Salicylate fails to prevent the inhibitory effect of 5,8,11,14-eicosatetraynoic acid on human platelet cyclo-oxygenase and lipoxygenase activities. Biochim Biophys Acta 759: 125, 1983 18. Siegel MI, McConnell RT, Porter NA, Cuatrecasas P: Arachidonate metabolism via lipoxygenase and 12L-hydroperoxy-5,8,10,14icosatetraenoic acid peroxidase sensitive to anti-inflammatory drugs. Proc Natl Acad Sci USA 77: 308, 1980 19. Rotilio D, Joseph D, Hatmi M, Vargaftig BB: Structural requirements for preventing the aspirin- and the arachidonate-induced inactivation of platelet cyclo-oxygense: additional evidence for distinct enzymatic sites. Eur J Pharmacol 97: 197, 1984 20. Dejana E, Cerletti C, De Castellamau C, Livio M, Galletti F, Latini R, de Gaetano G: Salicylate-aspirin interaction in the rat: evidence that salicylate accumulating during aspirin administration may protect vascular prostacyclin from aspirin-induced inhibition. J Clin Invest 68: 1108, 1981 21. Lefort J, Vargaftig BB: Role of platelets in aspirin-sensitive bron22. Judith Baggott, Antonella Bottazzi, Vincenzo de Ceglie, and Felice de Ceglie helped prepare the manuscript. 23. References 24. 1. Evans G, Packham MA, Nishizawa EE, Mustard JF, Murphy EA: The effect of acetylsalicylic acid on platelet function. J Exp Med 128: 877, 1968 2. Weiss HJ, Aledort LM, Kochwa S: The effect of salicylates on the hemostatic properties of platelets in man. J Clin Invest 47: 2169, 1968 1192 25. 26. choconstriction in the guinea-pig: interaction with salicylic acid. Br J Pharmacol 63: 35, 1978 Robert A: Antisecretory, antiulcer, cytoprotective and diarrheogenic properties of prostaglandins. Adv Prostaglandins Thromboxane Res 2: 507, 1976 Ali M, McDonald JWD: Interference by sulfinpyrazone and salicylate of aspirin inhibition of platelet cyclooxygenase activity. Prostaglandins Med 3: 327, 1979 Peterson DA, Gerrard JM, Rao GHR, White JG: Salicylic acid inhibition of the irreversible effect of acetylsalicylic acid on prostaglandin synthetase may be due to competition for the enzyme cationic binding site. Prostaglandins Med 6: 161, 1981 Livio M, Del Maschio A, Cerletti C, de Gaetano G: Indomethacin prevents the long-lasting inhibitory effect of aspirin on human platelet cyclooxygenase activity. Prostaglandins 23: 787, 1982 Rao GHR, Johnson GG, Reddy R, White JG: Ibuprofen protects CIRCULATION PLATELETS AND VASCULAR OCCLUSION 27. 28. 29. 30. 31. 32. 33. 34. Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 35. 36. 37. 38. 39. 40. 41. 42. 43. platelet cyclooxygenase from irreversible inhibition by aspirin. Arteriosclerosis 3: 383, 1983 Cerletti C, Bonati M, Del Maschio A, Galletti F, Dejana E, Tognoni G, de Gaetano G: Plasma levels of salicylate and aspirin in healthy volunteers: relevance to drug interaction on platelet function. J Lab Clin Med 103: 869, 1984 Moncada S, Vane JR: Pharmacology and endogenous roles of prostaglandin endoperoxides, thromboxane A2, and prostacyclin. Pharmacol Rev 30: 293, 1979 Marcus AJ: Aspirin and thromboembolism: a possible dilemma. N Engl J Med 297: 1284, 1977 Majerus PW: Arachidonate metabolism in vascular disorders. J Clin Invest 72: 1521, 1983 Dejana E, Costantini V, de Amicis G, Cerletti C, Lorenzi G, de Gaetano G: Differential salicylate-aspirin interaction on vascular prostacyclin and platelet thromboxane synthesis in patients undergoing saphenectomy. Proc Soc Exp Biol Med (in press) Ali M, McDonald JWD, Thiessen JJ, Coates PE: Plasma acetylsalicylate and salicylate and platelet cyclo-oxygenase activity following plain and enteric-coated aspirin. Stroke 11: 9, 1980 Rowland M, Riegelman S, Harris PA, Sholkoff SD: Absorption kinetics of aspirin in man following oral administration of an aqueous solution. J Pharm Sci 61: 379, 1972 Siebert DJ, Bochner F, Imhoff DM, Watts S, Lloyd JV, Field J, Gabb BW: Aspirin kinetics and platelet aggregation in man. Clin Pharmacol Ther 33: 367, 1983 FitzGerald GA: Novel aspects of aspirin action. In Proceedings of the 4th International Washington Spring Symposium, Washington, May 1984, abst. 52 Quick AJ, Clesceri L: Influence of acetylsalicylic acid and salicylamide on the coagulation of blood. J Pharmacol Exp Ther 128: 95, 1960 Loew D, Vinazzer H: Dose-dependent influence of acetylsalicylic acid on platelet functions and plasmatic coagulation factors. Haemostasis 5: 239, 1976 Menon IS: Aspirin and blood fibrinolysis. Lancet 1: 364, 1970 Moroz LA: Increased blood fibrinolytic activity after aspirin ingestion. N Engl J Med 296: 525, 1977 Green D, Davies RO, Holmes GI, Johnson C, Kohl H, Reynolds N, Ts'ao C-h: Fibrinolytic activity after administration of diflunisal and aspirin: a double-blind, randomized, placebo-controlled clinical trial. Haemostasis 13: 394, 1983 McKenna R, Galante J, Bachmann F, Wallace DL, Kaushal SP, Meredith P: Prevention of venous thromboembolism after total knee replacement by high-dose aspirin or intermittent calf and thigh compression. Br Med J 280: 514, 1980 Levin RI, Harpel PC, Weil D, Chang T-S, Rifkin DB: Aspirin inhibits vascular plasminogen activator activity in vivo: studies utilizing a new assay to quantify plasminogen activator activity. J Clin Invest 74: 571, 1984 Ghezzo F, Trinchero P, Pegoraro L: Effects of aspirin treatment upon fibrinolytic activity of peripheral blood granulocytes. Acta Haematol (Basel) 65: 229, 1981 Vol. 72, No. 6, December 1985 44. Roncaglioni MC, Ulrich M, Muller AD, Soute BAM, de Boer-van den Berg MAG, Vermeer C: The vitamin K-antagonism of salicylate and warfarin. Thromb Res (in press) 45. Owens MR, Cimino CD: The inhibitory effects of sodium salicylate on synthesis of factor VII by the perfused rat liver. Thromb Res 18: 839, 1980 46. Park BK, Leck JB: On the mechanism of salicylate-induced hypothrombinaemia. J Pharm Pharmacol 33: 25, 1981 47. Hildebrand EF, Suttie JW: The effects of salicylate on enzymes of vitamin K metabolism. J Pharm Pharmacol 35: 421, 1983 48. Owen MR, Cimino CD: The interaction of salicylate and vitamin K in synthesis of factor II (prothrombin). Thromb Res 31: 135, 1983 49. Dale J, Myhre E, Storstein 0, Stormorken H, Efskind L: Prevention of arterial thromboembolism with acetylsalicylic acid: a controlled clinical study in patients with aortic ball valves. Am Heart J 94: 101, 1977 50. Chesebro JH, Fuster V, Elveback LR, McGoon DC, Pluth JR, Puga FJ, Wallace RB, Danielson GK, Orszulak TA, Piehler JM, Schaff HV: Trial of combined warfarin plus dipyridamole or aspirin therapy in prosthetic heart valve replacement: danger of aspirin compared with dipyridamole. Am J Cardiol 51: 1537, 1983 51. Buchanan MR, Richke JA, Hirsh J: Aspirin inhibits platelet function independent of the acetylation of cyclo-oxygenase. Thromb Res 25: 363, 1982 52. Buczko W, de Gaetano G: Effect of high doses of aspirin and salicylate on bleeding time in rats. Thromb Res 32: 631, 1983 53. Sun FF, McGuire JC: Metabolism of arachidonic acid by human neutrophils: characterization of the enzymatic reactions that lead to the synthesis of leukotriene B4. Biochim Biophys Acta 772: 56, 1984 54. Lewis RA, Auster F: The biologically active leukotrienes: biosynthesis, metabolism, receptors, functions, and pharmacology. J Clin Invest 73: 889, 1984 55. Ford-Hutchinson AW, Bray MA, Doig MV, Shipley ME, Smith MJH: Leukotriene B4, a potent chemokinetic and aggregating substance released from polymorphonuclear leukocytes. Nature 286: 264, 1980 56. Villa S, Colotta F, de Gaetano G, Semeraro N: Arachidonic acid and leukotriene B4 induce aggregation of human peripheral blood mononuclear leukocytes in vitro. Br J Haematol 58: 137, 1984 57. Mullane KM, Read N, Salmon JA, Moncada S: Role of leukocytes in acute myocardial infarction in anesthetized dogs: relationship to myocardial salvage by anti-inflammatory drugs. J Pharmacol Exp Ther 228: 510, 1984 58. Higgs GA, Eakins KE, Mugridge KG, Moncada S, Vane JR: The effects of non-steroidal anti-inflammatory drugs on leukocyte migration in carrageenan-induced inflammation. Eur J Pharmacol 66: 81, 1980 59. Angelico F: Sulla trasformazione dell'acido salicilico nell'organismo animal. Arch Farmacol Sper 31: 8, 1921 60. Bochner F, Graham GG, Chan E, lmhoff DM, Haavisto TM: Salicylate metabolite kinetics after several salicylates. Clin Pharmacol Ther 30: 263, 1981 1193 Pharmacology of platelet inhibition in humans: implications of the salicylate-aspirin interaction. G de Gaetano, C Cerletti, E Dejana and R Latini Downloaded from http://circ.ahajournals.org/ by guest on April 28, 2017 Circulation. 1985;72:1185-1193 doi: 10.1161/01.CIR.72.6.1185 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1985 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/72/6/1185 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/