Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
1016
Left Ventricular Pressure-Volume and
Frank-Starling Relations in
Endurance Athletes
Implications for Orthostatic Tolerance and
Exercise Performance
Benjamin D. Levine, MD; Lynda D. Lane, MS, RN; Jay C. Buckey, MD;
Daniel B. Friedman, MD; and C. Gunnar Blomqvist, MD, PhD
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Background. Endurance athletes have a high incidence of orthostatic intolerance. We
hypothesized that this is related to an abnormally large decrease in left ventricular enddiastolic volume (LVEDV) and stroke volume (SV) for any given decrease in filling pressure.
Methods and Results. We measured pulmonary capillary wedge (PCW) pressure (Swan-Ganz
catheter), LVEDV (two-dimensional echocardiography), and cardiac output (C2H2 rebreathing)
during lower body negative pressure (LBNP, -15 and -30 mm Hg) and rapid saline infusion
(15 and 30 ml/kg) in seven athletes and six controls (Vo2max, 68±7 and 41±4 ml/kg/min).
Orthostatic tolerance was determined by progressive LBNP to presyncope. Athletes had steeper
slopes of their SV/PCW pressure curves than nonathletes (5.5+2.7 versus 2.7+1.5 mI/mm Hg,
p<0.05). The slope of the steep, linear portion of this curve correlated significantly with the
duration of LBNP tolerance (r=0.58, p=0.04). The athletes also had reduced chamber stiffness
(increased chamber compliance) expressed as the slope (k) of the dP/dV versus P relation
(chamber stiffness, k=0.008±0.004 versus 0.031±0.004, p<0.005; chamber compliance,
l/k=449.8+283.8 versus 35.3+±4.3). This resulted in larger absolute and relative changes in
end-diastolic volume over an equivalent range of filling pressures.
Conclusions. Endurance athletes have greater ventricular diastolic chamber compliance and
distensibility than nonathletes and thus operate on the steep portion of their Starling curve.
This may be a mechanical, nonautonomic cause of orthostatic intolerance. (Circulation
1991;84:1016-1023)
E ndurance training results in central and peripheral adaptations that markedly improve an
individual's ability to perform physical work.
Athletes are thus commonly assumed to be able to
tolerate many kinds of physiological stressors better
than nonathletes. Gravitational stress, or orthostasis,
however, may be one condition during which being an
endurance athlete may be a disadvantage.1,2
Tolerance to orthostatic stress requires the successful integration of multiple elements of cardiovascular control. Orthostatic hypotension results when
there is an abnormally large postural decrease in
From the University of Texas Southwestern Medical Center,
Dallas, Tex.
Supported by the National Aeronautics and Space Administration and the National Heart, Lung, and Blood Institute.
Address for correspondence: Benjamin D. Levine, MD, Division
of Cardiology, University of Texas Southwestern Medical Center,
5323 Harry Hines Blvd., Dallas, TX 75235-9034.
Received October 1, 1990; revision accepted April 9, 1991.
central blood volume, cardiac filling pressures, and
stroke volume (SV), or inadequate neurohumoral
reflex responses to orthostasis, primarily tachycardia
and vasoconstriction.3 Orthostatic intolerance has
been reported to be particularly prevalent in endurance-trained athletes",2 and has been attributed primarily to abnormalities in baroreflex regulation of
heart rate4 and peripheral resistance.56 However, a
potentially important but previously unrecognized
mechanism for orthostatic intolerance in athletes
might also be related to structural or mechanical
adaptations in the cardiovascular system.
We have recently demonstrated that individuals
with a large resting SV have a disproportionately
large decrease in SV during lower body negative
pressure (LBNP) and that these characteristics may
be important features of orthostatic intolerance in
endurance athletes.7 Furthermore, studies of the
effect of volume loading on SV and cardiac output
Levine et al Frank-Starling Relations in Athletes
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
indicate that individuals with the largest SV at rest
have the greatest increase in SV after loading.8 These
observations suggest that endurance training, which
delivers an acute volume load to the heart during
exercise, may alter the compliance characteristics of
the left ventricle. Such an adaptation may be very
beneficial during exercise, allowing for increased
diastolic reserve and therefore increased SV and
cardiac output in response to increased filling pressures. This adaptive response, however, may be detrimental during decreases as opposed to increases in
central blood volume and cardiac filling. We postulated that athletes have a steeper ventricular function
and flatter diastolic pressure-volume curve than sedentary subjects over the physiological range of filling
pressures. During orthostasis, this characteristic results in an abnormally large decrease in ventricular
volume when filling pressure is reduced. To test this
hypothesis, we examined left ventricular pressurevolume relations and Starling curves relating left
ventricular end-diastolic pressure (LVEDP) to SV in
endurance-trained athletes compared with sedentary
controls and compared differences in these relations
to differences in orthostatic tolerance.
Methods
Subjects
Subjects were 13 healthy male volunteers in whom
clear images could be obtained by screening twodimensional echocardiography. Subjects were nonobese nonsmokers less than 40 years of age and were
recruited and selected into two groups based on current
level of endurance training and maximal aerobic power
(Vo2max). Endurance athletes ran at least 50 miles per
week or bicycled at least 250 miles per week for at least
3 years (Vo2max, >60 ml/kg/min; n=7); sedentary
controls performed no regular exercise (Vo2max, <45
ml/kg/min; n=6).
The study was approved by the University of Texas
institutional research review committee, and informed
consent was obtained from all subjects before the study.
Aerobic Power
Vo2max was determined using a continuous incremental protocol on a treadmill. After a 5-minute
warm-up period, subjects began running at an individualized speed (6-12 mph) and 0% grade. The
grade was subsequently increased by 2% every
minute until an increase in work load produced no
further increase in Vo2. Gas concentrations and
ventilation were determined on a breath-by-breath
basis using a mass spectrometer (Perkin-Elmer) and
turbine flow meter (SensorMedics), respectively, and
interfaced with a dedicated AT&T computer for
calculation of Vo2.
Plasma volume was measured at a separate session
after 30 minutes of supine rest using Evans blue
indicator dilution.9 A blood sample was also drawn
through a peripheral vein and analyzed in triplicate
for hematocrit (HCT) by the microcapillary centri-
1017
fuge technique (Damon). Plasma volume was divided
by (1 -HCT) to give a measure of blood volume,
applying customary corrections for peripheral sampling (0.92) and red cell trapping of plasma (0.98).
Ventricular Filling Pressure and Cardiac Output
The mean pulmonary capillary wedge (PCW) pressure was used as a measure of LVEDP. A 6F
balloon-tipped, flow-directed pulmonary arterial
catheter (Swan-Ganz, American Edwards Laboratories) was placed percutaneously from a right brachial
vein and advanced under fluoroscopic guidance into
the PCW position. Correct position of the catheter
was confirmed fluoroscopically and by the presence
of characteristic pressure waveforms. The catheter
was connected to a physiological pressure transducer
(Gould-Statham) with the zero reference point set at
5 cm below the sternal angle. The signal was passed
through an amplifier (Hewlett-Packard 8805B) to an
inkjet recorder (Mingograph) calibrated to display 1
mm Hg/2 mm paper. Mean PCW pressure was determined visually at end expiration.
To minimize perturbation of the system being
evaluated by frequent injections of saline, cardiac
output was measured with a standard inert gas
rebreathing technique using acetylene as the soluble
gas and helium as the insoluble gas. Adequate mixing
of rebreathing gas in the lung was confirmed by a
constant level of helium in all cases. This technique
has been described previously from our laboratory10
and has been validated against both green dye10 and
thermodilution1l methods in normal subjects and in
patients with significant cardiopulmonary disease.
Heart rate was measured and averaged over 20
seconds during the rebreathing, and SV was then
calculated.
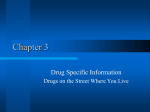
Ventricular filling was manipulated using a sequence of LBNP and rapid saline infusion as shown
in Figure 1. LBNP was accomplished by placing the
subjects in a cylindrical metal tank sealed at the level
of the iliac crest. Suction was provided by a vacuum
pump and controlled with a regulator calibrated
against a mercury manometer. Measurements of
PCW pressure and SV were made after at least 30
minutes in the supine position at rest and after 5
minutes each at -15 mm Hg and -30 mm Hg LBNP.
After the LBNP and at least a 15-minute rest period,
resting measurements were repeated to ensure return to baseline condition. Ventricular filling was
then increased using a rapid infusion of warm isotonic saline (37°C, 10 min/l). The saline was infused
through the proximal port of the Swan-Ganz catheter
and through an 18-gauge peripheral i.v. placed in the
opposite antecubital vein. Measurements of PCW
pressure and SV were again made after 15 ml/kg and
30 ml/kg saline were infused.
Ventricular Volumes
Left ventricular volumes were determined using
two-dimensional echocardiography. Images were obtained from standard windows using a phased-array
1018
Circulation Vol 84, No 3 September 1991
PROTOCOL FOR CHANJGING
CENTRAL BLOOD VOlLUME
USING LOWER BODY NEGATIVE PRE.SSURE AND SALINE
30 mI/kg SALINE
*
15 mi/kg SALINE
*
REPEAT BASELIN [E
-15 mmHG LBNP
-30 mmHg LONP
0
30
I
35
40
TIME (m1n)
55
65
75
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
FIGURE 1. Chart demonstrating the protocol used to alter
central blood volume during the experiment. After at least a
30-minute baseline period, measurements of cardiac output
were repeated until stable (two consecutive values within 500
ml) followed with LBNP of -15 mm Hg and -30 mm Hg.
After 5 minutes at each level, two-dimensional echocardiography, pulmonaty capillary wedge pressure measurement, and
cardiac output were performed. After release of LBNP, there
was a 15-minute recovery period where baseline measurements
were repeated. This was then followed by rapid infusion of
warm saline at a rate of approximately 10 minll. The same
tests were repeated after 15 and 30 mllkg were infused. All
measurements were obtained under hemodynamic steady-state
conditions. *Measurement ofpulmonary capillary wedge pressure, cardiac output, and left ventricular volumes via twodimensional echocardiography. LBNP, lower body negative
pressure.
transducer with a frequency of 2.5 or 3.5 MHz
(Hewlett-Packard 77020A Ultrasound Imaging System). Data were collected on videotape and played
back on a videotape recorder (Panasonic AG-6200).
The images were digitized on an image processing
and quantitation system (MICROSONICS CAD886,
Version 2.5). A continuous-loop presentation was
used to capture the best cardiac cycles for analysis.
Two or three beats were averaged during steady-state
hemodynamic conditions, with the subject pausing
during the respiratory cycle at end expiration.
Measurements were made of the left ventricular
area from the parasternal short-axis window at the
level of the mitral valve and papillary muscles, and
major and minor axes lengths were obtained from the
short-axis and apical long-axis views. Volumes were
then calculated in biplane format using the MICROSONICS software by modeling the left ventricle as
a prolate ellipsoid (length-area method) using standard formulas as recommended by the American
Society of Echocardiography.12 All echocardiographic studies were analyzed by a skilled technician
unaware of fitness group or the purpose of the study.
In our hands, echocardiographically derived measurements of left ventricular end-diastolic volume
(LVEDV) have an interobserver variability of 10%.
Furthermore, validation studies within our laboratory comparing echocardiographic volumes with biplane angiography at cardiac catherization in 30
subjects demonstrated an r value of 0.90 with a
standard error of the mean of 26 ml.
Orthostatic Tolerance
Tolerance to LBNP, which decreases central blood
volume in a graded fashion, was used as a measure of
orthostatic tolerance.13 At a separate session, at least
48 hours after but within a week of the Starling curve
determination, the subjects were placed in the LBNP
tank, and the suction was increased in a stepwise
fashion according to the following protocol: -15
mm Hgx 15 minutes, -30 mm Hgx5 minutes, -40
mm Hg x 15 minutes, and -55 mm Hg (the maximum
suction generated by our device) x30 minutes. This
protocol has been used in previous studies of cardiovascular regulation following head-down tilt14 and
allows data collection at both high and low levels of
LBNP as well as a test of maximal tolerance. LBNP
was discontinued if the subject developed signs or
symptoms of presyncope (sudden onset of nausea,
sweating, lightheadedness, bradycardia, or hypotension) or a sustained decrease in systolic blood pressure below 90 mm Hg. An index of tolerance,
LBNPxtime, was calculated by summing the product
of pressure and duration at each level of LBNP.
Statistics
We performed linear regression on the individual
data to identify the slope of the relation between the
change in PCW pressure and the change in SV during
both LBNP and saline infusion. The slopes for the
subjects were then grouped and the means compared
separately for both a decrease and increase in left
ventricular filling using the unpaired t test. This strategy was determined a priori. We also compared the
relation between end-diastolic volume and SV between groups using a repeated-measures analysis of
covariance with a time-varying covariate (BMDP 5v,
BMDP Statistical Software Inc., Los Angeles). The
relation between the slope of the linear portion of the
PCW pressure/stroke volume curve during decreased
left ventricular filling and LBNPxtime was determined by linear regression with Pearson's correlation.
Pressure-volume curves were analyzed by modeling the relation according to the exponential equation P=aekv+b, where P is PCW pressure, V is
LVEDV, and a,b, and k are constants. 15 Curve fitting
was performed with the Marquardt-Levenberg algorithm using commercially available software (SIGMAPLOT 4.04, Jandel Scientific, Corte Madera, Calif.).
The constant k then represents the slope of the
relation describing the instantaneous change in pressure for a change in volume at any given pressure
(dP/dV versus P), and was used as an estimate of
chamber stiffness.15 We also calculated the inverse of
k to provide an index of chamber compliance. Curvefitting parameters were calculated for each individual
Levine et al Frank-Starling Relations in Athletes
TABLE 1. Subject Characteristics
Lower body negative
pressurextime (mm Hgxmin)
Age (yr)
Athletes
Nonathletes
1,345±668*
2,516+881
27+2
68.4±6.6*
178±1
69.3±2.5*
110±6*
77.4±2.8*
27±1
40.8±4.4
178±3
75.8±2.6
83±3.9
57.8±3.4
217±14*
164±12
Vo2max (ml/kg/min)
Height (cm)
Weight (kg)
Stroke volume (ml)
Blood volume (mllkg)
Left ventricular end-diastolic
volume (ml)
Values are mean±SD.
*p<0.05 vs. nonathletes.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
curve, and the means were compared between groups
using the unpaired t test.
Hemodynamic variables were compared using a
repeated-measures analysis of variance with Scheffe's
post hoc for multiple comparisons.
Results
Subject Characteristics
The subjects were closely matched for age, height,
and weight (Table 1). LBNP tolerance was significantly lower in the athletes compared with the
nonathletes: 1,345 mm Hg x min + 668 versus 2,516 +
881 mm Hgxmin (p<0.02). Six of seven athletes had
presyncopal reactions during maximal LBNP testing
compared with one of six nonathletes. The athletes
had larger Vo2max by design (68.4+6.6 versus
40.8±4.4 ml/kg/min) as well as larger LVEDV, SV,
and plasma/blood volumes.
Starling Curves (PCW Pressure Versus SV)
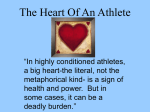
Representative pressure tracings from one subject
(Figure 2) demonstrate that with our techniques of
LBNP and saline infusion, we were able to vary PCW
pressure over a wide physiological range of almost 20
mm Hg. Hemodynamic conditions associated with
this change in cardiac filling are provided in Table 2.
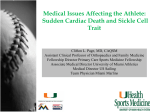
The relations between PCW pressure and SV for the
mean group data (Figure 3) demonstrate two important points. First, for any given filling pressure, the
ECG
(mmHg)
athletes had a greater stroke volume than the
nonathletes. Second, they also had a greater change
in stroke volume with any change in central blood
volume and cardiac filling pressure, as manifested by
the slope of the steep linear portion of these curves.
This slope, determined over a range of filling pressures from 1 to 13 mm Hg by linear regression (mean
r value of 0.92+0.03 for all subjects), was significantly
steeper in the athletes at 5.5 ±2.7 ml/mm Hg versus
2.7+ 1.5 ml/mm Hg in the nonathietes (p=0.03). The
functional consequence of this concept (Figure 4) is
that a decrease in PCW, for example, from 10 to 5
mm Hg as might occur going from supine to upright
posture, would be associated with a 27-ml decrease in
SV in the athletes (25% of baseline), nearly twice the
14-ml decrease in SV that would be observed with
the same stress in the nonathletes (17% of baseline).
The magnitude of this decrease in SV appeared to
play an important role in determining LBNP tolerance because the slope of the steep linear portion of
the PCW pressure versus SV curve correlated significantly with LBNPxtime (Figure 5; r=0.58, p=0.04).
The relation between LVEDV and SV was determined as linear for both groups (r=0.97 for athletes,
0.65 for nonathletes), with the athletes shifted to
higher values of LVEDV and SV than the nonathletes. Analysis of covariance could not distinguish
between the slopes of these relations, however, suggesting that the athletes had greater filling but similar
left ventricular systolic function measured as ejection
fraction compared with the nonathletes.
Pressure-Volume Curves
The mean grouped data relating LVEDV to PCW
pressure are shown in Figure 6. The curve for the
athletes is shifted downward and to the right; therefore for any given end-diastolic volume, the athletes
had a much lower PCW pressure than the nonathletes, suggesting greater chamber compliance and
distensibility. This observation is confirmed statistically by fitting the data to the exponential curve
P=aekv+b. For the athletes, the mean curve was
P=0.023e0028V+0.394; for the nonathletes it was
P=0.035eO37V-2.926. The individual chamber stiffness constant k was significantly less (reflecting
-.AA A&
20
1019
AA
JAKK
".A4
.
-
-
A'~
10
AI'ANM.MAA.M
O _
-30 mm Hg
LBNP
-15 mm Hg
LBNP
Baseline
15cc/kg
saline
30cc/kg
saline
FIGURE 2. Pressure tracings from the pulmonary capillary wedge position in one representative subject during change in central
blood volume. A and V waves are clearly seen, with the appropriate timing with the ECG, confirming placement of the catheter in
the pulmonary capillary wedge (PCW) position. LBNP, lower body negative pressure.
1020
Circulation Vol 84, No 3 September 1991
TABLE 2. Hemodynamics
Athletes
Rest
-15 mm Hg LBNP
-30 mm Hg LBNP
Repeat baseline
+15 ml/kg saline
+30 mI/kg saline
Before max LBNP test
Heart rate
Blood pressure
Stroke volume
(beats/min)
(mm Hg)
(m1)
53+3
88+1
89±1
113+4
1,204+61
95±6*
74±4t
111+4
1,399±100
55+3
79+7t
61±5
54+3
58±3
61±4
56±4
90+1
93±2
TPR
(dyne sec
130+5*
Cardiac output
Pulmonary capillary
wedge pressure
(I/min)
(mm Hg)
5.97+0.32
5.31+0.48
10.1+0.8
cm-5)
6.4±0.7t
3.4±0.7t
10.3±0.6
1.449-+172§
1,218+61
1,015±77
955±67§
1,112±55
4.33±0.19'I
7.59+0.5911
15.41.1t
8.01+0.68t
6.07+0.14
16.5 ±0.5t
10.5±0.6
5.94±0.22
84+3
131+51I
110±6
83+1
77+4
85±2
84±3
1,399+73
1,467+85
4.81±0.29
78+7
4.72+0.33
7.5±0.5t
63±6§
1,582±71§
4.30+J0.30§
84±6
1,256± 101
98+6t
1,008+721I
5.46±0.39
6.90±0.51t
7.66±0.33t
5.39±0.39
5.1 +0.7t
10.3±0.5
93±2t
Nonathietes
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
63±4
Rest
62+4
-15 mm Hg LBNP
69±5
-30 mm Hg LBNP
65+3
Repeat baseline
71±3
+15 ml/kg saline
+30 ml/kg saline
77+2t
65±4
Before max LBNP test
TPR, total peripheral resistance; LBNP,
Values are mean±SEM.
84±2
85±2
915±51t
87±2
100±4t
80±3
83±4
lower body negative pressure.
1,231±+112
15.5+0.3t
17.6±0.9t
...
*p<O.10; tp<0.01 vs. rest; tp<0.05; §p<O.O1 for comparison between -30 mm Hg LBNP and 30 ml/kg saline (if no difference from rest);
Ip<0.05.
greater chamber compliance) in the athletes compared with the nonathletes (chamber stiffness,
k=0.008±+ 0.004 versus 0.031±+ 0.004, p <0.005; chamber compliance, 1/k=449.8±283.8 versus 35.3±4.3,
p<0.05). Thus, they had larger absolute (64 versus 14
ml) and relative (30% versus 9% of baseline) changes
in end-diastolic volume over the range of central
blood volume induced by LBNP and saline loading.
Discussion
This study provides new information regarding
cardiovascular regulation in endurance athletes in
two important ways. First, athletes have more compliant, distensible ventricles and therefore a steeper
STARLING CURVES
DECREASE IN STROKE VOLUME
WITH A DECREASE IN PCW FROM 10 - 5 mmHg
0
40 -4
E
UJ
E
m
0
ui
30-
100 -
IUl
_i
_i
0
z
204-_
g
*
z
W
10
*
-
t
0
0
ATHLETES
Ffin
VV
A
*A
I
|
{
-- --.
-1
10
PULMONARY CAPILLARY WEDGE PRESSURE (mmHg)
FIGURE 3.
Mean
grouped
data ±-SEM,
demonstrating
the
Starling curves relating pulmonary capillary wedge pressure to
stroke volume in athletes and nonathletes. The mean curves
are representative of the individual data. Lines are computer
fits of the best polynomial regression through the data.
0
1--HX
NON-ATHLETES
FIGURE 4. Individual data points represent the decrease in
stroke volume that would be seen in each subject ifpulmonary
capillary wedge (PCW) pressure decreased from 10 to 5
mm Hg, similar to what might occur with standing. The
athletes had a significantly greater fall in stroke volume for the
same decrease in filling pressure (p <O. 05). Two athletes had
the same fall in stroke volume, and their points appear
superimposed.
Levine et al Frank-Starling Relations in Athletes
1021
.
3000 +
S
.
y = 2791 215x
(r=0.58; p=0.039)
-
n
ki
E
X
|*
ATHLETES
NON-ATHLETES
|
EiE 2000 0~~~
O
O
z
\~~
>
1000 - _
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
* ~~~~
.
._
*-
..
O~~~
\
.
...
****
*********
.*
2
4
..
...
m.
6
0~~~
...
8
SLOPE OF LINEAR PORTION OF STARLING CURVE (mi/mmHg)
FIGURE 5. Relation between the slope of the linear portion of the Starling curve relating stroke volume to pulmonary capillary
wedge pressure in each subject determined by linear regression as described in the text and lower body negative pressure x time, a
measure of orthostatic tolerance.
slope of the Frank-Starling curve relating left ventricular filling pressure to stroke volume than nonathletes. Second, the slope of the steep linear portion of
this relation is an independent predictor of orthostatic intolerance, and thus may play a role in explaining the increased prevalence of orthostatic
PRESSURE/VOLUME CURVES
,
m
20-
E
T
E
UJ
a:
0
1-LT~ ~~~
I1
m
/~~~~~
0
*
EB
N
0t
E
0
1C0
200
250
LV END-DIASTOUC VOLUME (ml)
FIGURE 6. Mean grouped data ±SEM for the pressurevolume curves relating left ventricular end-diastolic volume as
determined by two-dimensional echocardiography and pulmonary capillary wedge pressure. Lines are computer fits of the
best polynomial regression through the data. LBNP, lower
body negative pressure.
hypotension in well-trained endurance athletes with
high aerobic power.
The relation between LVEDP and SV describes
one form of Starling's law of the heart.16 In normal
sedentary supine men, the left ventricle appears to
operate near the peak or plateau of this hyperbolic
curve at an LVEDP of approximately 10 mm Hg.17
Thus, with exercise in the supine position, diastolic
reserve is limited and virtually completely utilized at
lower levels of exercise.18-20 Studies examining exercise responses in untrained subjects using radionuclide techniques suggest that in such individuals, the
Frank-Starling mechanism is important in increasing
SV and cardiac output primarily at submaximal levels
of exercise.18-20 As maximal exercise loads are approached, increasing heart rate and contractility become the predominant mechanisms for meeting further increases in metabolic demand. The upright
position, by precipitating venous pooling and decreasing central blood volume, appears to shift the
heart to the flatter portion of the diastolic pressurevolume curve and the steeper portion of the
LVEDP/SV curve, allowing a greater increase in
LVEDV and SV during submaximal exercise.18,19
However, ventricular distension is still limited at
peak exercise.
On the other hand, elite athletes appear to have an
increased capacity to utilize the Frank-Starling mechanism to increase SV during exercise.2122 This increase in SV during upright exercise is due primarily
1022
Circulation Vol 84, No 3 September 1991
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
to an increase in end-diastolic volume, which in
athletes is accompanied by an increase in myocardial
mass to maintain a normal relation between cavity
size and wall thickness.8 There is little evidence that
human intrinsic ventricular systolic performance is
altered by endurance training.8
The present study extends these observations by
demonstrating a general physiological mechanism for
enhancing cardiac pump performance. By functioning on the steep portion of the Starling curve, endurance athletes have increased diastolic reserve and a
greater change in SV for a given change in filling
pressure than untrained individuals. This difference
results from increases in chamber compliance or
distensibility as reflected by the dP/dV of the diastolic pressure-volume relation in the athletes.
How might this adaptation occur? Numerous studies have shown a consistent linear relation between
Vo2 and cardiac output.8 Furthermore, Ekelund and
Holmgren23 demonstrated a linear relation between
cardiac output and PCW pressure both in athletes
and sedentary individuals. While such cross-sectional
studies do not allow a clear distinction between an
innate characteristic of successful athletes and the
end result of long-term, intensive endurance training,
it seems likely that exercise in athletes, who train at
high Vo2 and cardiac output, imposes a prominent
volume load on the heart, causing elevated filling
pressures during training and resulting in an increase
in end-diastolic volume.
Acutely, the limit to ventricular dilation is probably
dependent on both the compliance characteristics of
the myocardium and pericardial or pulmonary mechanical restraint. In fact, removing the pericardium
in dogs increases end-diastolic volume during exercise, increases maximal cardiac output, and therefore
increases maximal aerobic power.24 It is difficult to
sort out the relative contributions of myocardial
compliance and pericardial restraint to limiting ventricular filling during exercise. However, the present
study strongly suggests that the chronic volume loading of endurance training results in increased effective ventricular compliance and alters the pressurevolume relation and therefore Starling (SV/LVEDP)
relation of the athlete's heart. Such an increased
chamber compliance and steep Starling curve is
teleologically very beneficial to an athlete, facilitating
the delivery of large volumes of blood to exercising
skeletal muscle. However, it may be a distinct disadvantage during orthostasis, resulting in a large decrease in SV when filling pressure is reduced. In the
present study, this hypothesis is supported by the
observation that the steepness of the LVEDP/SV
curve correlates significantly with tolerance to LBNP.
The issue of orthostatic intolerance in endurance
athletes has been a controversial one since Stegemann et a125 first described depressed carotid baroreflex sensitivity in a group of trained athletes. Subsequent work has focused almost exclusively on the
baroreflex regulation of heart rate (HR) and peripheral resistance (TPR), and has recently been re-
viewed.1,2 In our laboratory,7 we have recently emphasized the equal importance of SV in the "triple
product" of blood pressure control (HRxSVxTPR).
We demonstrated a large decrease in SV during
LBNP in individuals with orthostatic intolerance
(primarily athletes) and suggested that SV might be
an important independent factor not under the exclusive control of the autonomic nervous system. The
present study does not exclude autonomic influences
on ventricular filling and contractility but does show
that adaptations affecting mechanical diastolic properties of the athlete's heart can explain a significant
component of the orthostatic intolerance seen in this
group. Furthermore, this ventricular adaptation
would tend to magnify the effects of any impairment
of baroreflex control of heart rate and peripheral
resistance.
There are potential limitations to the present study
that must be considered in interpreting the results.
As has been pointed out by Nobel,16 the Starling
curve relating LVEDP to SV may not actually describe a pressure-volume relation and may more
precisely reflect the constancy of end-systolic volume
for a given end-ejection pressure. However, the
shape of this form of the Starling ventricular function
curve depends critically on the configuration of the
diastolic pressure-volume relation, which in turn is a
function of the length-tension relation of individual
sarcomeres.17 Furthermore, SV remains an almost
constant fraction of end-diastolic volume throughout
a wide range of left ventricular filling pressures.26 In
the present study, we constructed both curves - SV as
a function of PCW pressure using an acetylene
rebreathing method to measure cardiac output, and
PCW pressure as a function of LVEDV using twodimensional echocardiography. The confirmation of
the same phenomenon - that athletes have large
changes in end-diastolic volume and SV with changes
in left ventricular filling -by two independent techniques (echocardiography and C2H2 rebreathing) argues strongly that we are identifying a true physiological characteristic of endurance athletes.
We must emphasize that the maintenance of blood
pressure during orthostatic stress depends on multiple components of cardiovascular regulation, including baroreflex control of heart rate and peripheral
resistance. The relatively weak though statistically
significant negative relation between the slope of the
linear portion of the end-diastolic pressure/SV curve
and LBNP tolerance argues for the importance of
these other variables in predicting individual orthostatic tolerance. The present study thus provides one
piece of the puzzle and complements previous investigations of blood pressure control in athletes by
identifying nonautonomic control of SV as an important variable.
We have demonstrated that endurance athletes
have greater effective left ventricular diastolic chamber compliance and distensibility than nonathletes
and thus have a steeper slope of their Starling curve
relating left ventricular filling pressure to SV. The
Levine et al Frank-Starling Relations in Athletes
slope of this relation correlated significantly with
LBNP tolerance, suggesting an important role for
mechanical, nonautonomic factors in the orthostatic
intolerance observed in endurance athletes.
Acknowledgments
We gratefully acknowledge the technical assistance
of Mr. Willie Moore and the secretarial assistance of
Mrs. Carolyn Donahue. We also must thank Dr. Jim
Stray-Gundersen, Ms. Andrea Katz, and Mr. Wyman
Schultz for performing the exercise tests and Ms.
Debra Epstein and Ms. Margaret Morin for analyzing the echocardiograms. Rick Risser provided invaluable statistical consultation. We are indebted to
Drs. Michael Zile and Eric Eichorn for their insight
into the analysis of our diastolic pressure-volume
curves and Drs. Ron Victor and F. Andrew Gaffney
for their thoughtful reviews of the manuscript.
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Convertino VA: Aerobic fitness, endurance training, and
orthostatic intolerance. Exerc Sport Sci Rev 1987;15:223-260
Harrison MH: Athletes, astronauts, and orthostatic intolerance. Sports Med 1986;3:428-435
Blomqvist CG: Orthostatic hypotension, in Parmley WW,
Chaterjee K (eds): Cardiology. Philadelphia, JB Lippincott,
1990, pp 1-20
Smith ML, Raven PB: Cardiovascular response to lower body
negative pressure in endurance and static exercise-trained
men. Med Sci Sports Exerc 1986;18:545-550
Smith ML, Hudson DL, Graitzer HM, Raven PB: Blood
pressure regulation during cardiac autonomic blockade: Effect
of fitness. JAppl Physiol 1988;65:1789-1795
Mack GW, Shi X, Nose H, Tripathi A, Nadel ER: Diminished
baroreflex contol of forearm vascular resistance in physically
fit humans. JAppl Physiol 1987;63:105-110
Levine BD, Buckey JC, Fritsch JM, Yancy Jr CW, Watenpaugh DE, Snell PG, Lane LD, Eckberg DL, Blomqvist CG:
Physical fitness and cardiovascular regulation: Mechanisms of
orthostatic intolerance. JAppl Physiol 1991;70:112-122
Blomqvist CG, Saltin B: Cardiovascular adaptations to physical training. Annu Rev Physiol 1983;45:169-189
Nielsen MH, Nielsen NC: Spectrophotometric determination
of Evans Blue dye in plasma with individual correction for
blank density by a modified Gaeblers method. Scand J Clin
Lab Invest 1962;14:605-617
Triebwasser JH, Johnson RL, Burpo RP, Campbell JC, Reardon WC, Blomqvist CG: Noninvasive determination of cardiac
output by a modified acetylene rebreathing procedure utilizing
mass spectrometer measurements. Aviat Space Environ Med
1977;48:203-209
1023
11. Kallay MC, Hyde RW, Smith RJ, Rothbard RL, Schreiner BF:
Cardiac output by rebreathing in patients with cardiopulmonary diseases. JAppl Physiol 1987;63:201-210
12. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R,
Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I,
Silverman NH, Tajik AJ: Recommendations for quantitation
of the left ventricle by two-dimensional echocardiography. J
Am Soc Echo 1989;2:358-367
13. Mark AL, Mancia G: Cardiopulmonary baroreflexes in
humans, in Handbook of Physiology, Shepherd JT and Abboud
FM (eds), Section 2, The Cardiovascular System 1983;III(2):
795-813
14. Beck L, Blomqvist CG, Arbeille PH, Baisch F, Buckey JC,
Gaffney FA, Hillerbrecht A, Karemaker J, Patat F, Schulz H,
Ten Harkel DJ: Effect of a 10-day HDT on the hemodynamic
response to LBNP. Physiologist 1990;33(suppl l):s173-s174
15. Mirsky I: Assessment of diastolic funtion: Suggested methods
and future considerations. Circulation 1984;69:836-841
16. Nobel MIM: The Frank-Starling curve. Clin Sci Mol Med
1978;54:1-7
17. Parker JO, Case RB: Normal left ventricular function. Circulation 1979;1:4-12
18. Poliner LR, Dehmer GJ, Lewis SE, Parkey RW, Blomqvist
CG, Willerson JT: Left ventricular performance in normal
subjects: A comparison of the response to exercise in the
upright and supine positions. Circulation 1980;62:528-534
19. Steingart RM, Wexler J, Slagle S, Scheuer J: Radionuclide
ventriculographic responses to graded supine and upright
exercise: Critical role of the Frank-Starling mechanism at
submaximal exercise. Am J Cardiol 1984;53:1671-1677
20. Plotnick GD, Becker LC, Fisher ML, Gerstenblith G, Renlund DG, Fleg JL, Weisfeldt ML, Lakatta EG: Use of the
Frank-Starling mechanism during submaximal versus maximal
upright exercise. Am J Physiol 1986;251:H1101-H1105
21. Rerych SK, Scholz PM, Sabiston DC, Jones RH: Effects of
exercise training on left ventricular function in normal subjects: A longitudinal study by radionuclide angiography. Am J
Cardiol 1980;45:244-252
22. Crawford MH, Petru MA, Rabinowitz C: Effect of isotonic
exercise training on left ventricular volume during upright
exercise. Circulation 1985;72:1237-1243
23. Ekelund LG, Holmgren A: Central hemodynamics during
exercise. Circ Res 1967;20(suppl I):I-33-I-43
24. Stray-Gundersen J, Musch TI, Haidet GC, Swain DP, Ordway
GA, Mitchell JH: The effect of pericardiectomy on maximal
oxygen consumption and maximal cardiac output in untrained
dogs. Circ Res 1986;58:523-530
25. Stegemann J, Busert A, Brock D: Influence of fitness on the
blood pressure control system in man. Aerospace Med 1974;45:
45-48
26. Nixon JV, Murray RG, Leonard JH, Mitchell JH, Blomqvist
CG: Effects of large variation in pre-load on ventricular
performance characteristics in normal subjects. Circulation
1982;65:698-703
KEY WORDS
* athletes
compliance
Frank-Starling relation * orthostatic intolerance
pressure-volume relation * chamber stiffness,
Left ventricular pressure-volume and Frank-Starling relations in endurance athletes.
Implications for orthostatic tolerance and exercise performance.
B D Levine, L D Lane, J C Buckey, D B Friedman and C G Blomqvist
Downloaded from http://circ.ahajournals.org/ by guest on April 29, 2017
Circulation. 1991;84:1016-1023
doi: 10.1161/01.CIR.84.3.1016
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1991 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/84/3/1016
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/