Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Medical Issues Affecting the Athlete:
Sudden Cardiac Death and Sickle Cell
Trait
Clifton L. Page, MD, CAQSM
Assistant Clinical Professor of Orthopaedics and Family Medicine
Fellowship Director Primary Care Sports Medicine Fellowship
Associate Medical Director University of Miami Athletics
Medical Director US Sailing
Team Physician Miami Marlins
Disclosures
• None
Sudden Cardiac Death
• Non-traumatic and unexpected
sudden cardiac arrest that occurs
within hours of a previously normal
state of health
• In athletes: usually occurs during or
shortly after training or competition,
suggesting intense physical exertion
as a precipitating factor
• This definition includes blunt trauma
to the chest wall in the absence of
cardiovascular disease
Epidemiology
• Rare event
• 1/100,000 to 1/300,000 athletes
• True incidence difficult to
determine
• 50-100 cases in the US/year
• 5 times more common in males
than in females
• Higher rates seen in football and
basketball
SCD in NCAA Athletes
• 45 cardiac-related deaths
• NCAA athletes (2003-2008) =
1,994,962
• Incidence = 1:43,000 per year
– Black 1:17,000 / White 1:58,000
– Male 1:33,000 / Female 1:76,000
– Male/black 1:13,000
– Male/basketball 1:7,000
• Harmon et al. Circulation 2011
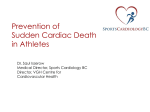
Characteristics of
sudden deaths
associated with
physical exertion or
sports in young
persons
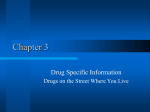
Causes of Sudden Death in NCAA
Athletes
Hypertrophic
Cardiomyopathy
• Autosomal
dominant disease
of sarcomeres;
increased
proliferation and
disorganized
arrangement
• Prevalence of 0.050.2% of the
population
Treatment Considerations
• Asymptomatic Patients
– Aggressive treatment of other cardiac risk factors
– Low impact aerobic activity
– Avoid dehydration and vasodilators
• Symptomatic Patients
– Beta blockers (verapamil second line)
– Septal myomectomy or alcohol septal ablation
• ICD placement
– with prior documented cardiac arrest, ventricular
fibrillation, or hemodynamically significant VT
– SCD in a first degree relative
– LV thickness of >30mm
– H/O syncopal episode
– NSVT
– Abnormal BP response to exercise
Myocarditis
• Inflammation of the heart muscle
• Usually following viral infection
• Presentation: chest pain,
arrhythmias, heart failure
• Physical activity should be
restricted for 6 mo
Arrhythmogenic Right Ventricular Dysplasia
• Genetic defects in desmosomes
• Fatty infiltration and fibrosis of the right
ventricle causing hypokinesis
• Rare in the US (1/10,000)
• More common in other
countries
Congenital Long QT
syndrome
• Presents with palpitations,
presyncope, syncope, seizures, or
cardiac arrest from arrhythmia. May
be associated with hearing loss.
• QT = start of Q to end of T; average
from 5 measurements and corrected
for rate
• >0.46 in children <15yo
>0.45 in men
>0.47 in women
Wolff-Parkinson-White Syndrome
• Accessory pathway between
atria and ventricle that can lead
to re-entrant SVT
• Delta waves on EKG
• Can be treated medically or with
catheter ablation
• EP testing should be done to
determine treatment before
cleared for sports participation
Brugada Syndrome
• Seen in subset of
individuals with
idiopathic ventricular
fibrillation
• Abnormality of the
SCN5A sodium channel
• Autosomal dominant
genetic transmission
• DX: 12-Lead EKG
shows incomplete
RBBB and ST segment
elevations in precordial
leads
Commotio Cordis
• Blunt, non-penetrating,
innocent-appearing blows
to the chest
• Can induce ventricular
fibrillation, complete heart
block and ST elevation
reproducibly with lowenergy blows to the chest
wall
• Most common in children &
adolescents (mean age 13)
• Most commonly: baseballs
& hockey pucks
• Survival is uncommon ~15%
Marfan’s syndrome
• At risk for aortic aneurysm and ruptures
• Genetic mutation of fibrillin gene
• Ghent criteria for diagnosis
– Dilated aorta, mitral valve prolapse, ectopic lens,
thumb or wrist sign, pneumothorax, scoliosis or
kyphosis, increased arm span to height, myopia
Isaiah Austin
Athlete’s Heart
• Cardiac hypertrophy from training
• Symmetric, usually <12mm thickness
• Associated with increase LV cavity; no LA
enlargement
• Decreases with deconditioning
Cardiac Evaluation in Athletes
• American Heart Association
– Personal history, family history, and PE
– ECG not recommended; cost, false
positives
• European Society of Cardiology, IOC
– History, PE, and ECG
– Italian screening program initiated in
1982
• Incidence of SCD from 3.6/100,000 –
0.4/100,000
• In a study of 33,735 athletes, 22 were found
to have HCM; 18 had an abnormal EKG
while only 5 had abnormalities on H and P
Maron B, et al. Circulation. 2007;115:1643-1655. Corrado D, et al. JAMA. 2006;296: 1593–1601. Corrado D, et al. N Engl J Med. 1998 Aug
6;339(6):364-9. Corrado D, et al. Eur Heart J. 2005;26:516 –524. IOC Medical Commission, December 10, 2004. Available at:
http://multimedia.olympic.org/pdf/en_report_886.pdf. Accessed December 15,2004.
History and Physical
• Chest pain or dyspnea w/ exertion,
syncope, heart murmur, HTN
• Family hx: Death or disability from
heart disease < 50yo, family
members with cardiac conditions
• PE: murmur, equal femoral pulses,
Marfan features, brachial artery BP
ECG’s in Athletes
• Normal findings:
–
–
–
–
–
–
–
–
–
–
Sinus bradycardia
Sinus arrhythmia
Ectopic atrial rhythm
Junctional escape rhythm
1° AV block (PR interval > 200 ms)
Mobitz Type I (Wenckebach) 2° AV block
Incomplete RBBB
QRS voltage criteria for LVH
Early repolarization
Convex (“domed”) ST segment elevation combined with T-wave
inversion in leads V1-V4 in black/African athletes
Riding et al; BJSM 2014
Concerning EKG Findings
•
•
•
•
•
•
•
•
•
•
•
T-wave inversion
ST depression
Pathologic Q-waves
Intra-ventricular conduction delay (QRS ≥
140ms)
≥ 2 PVCs per 10 sec
Ventricular arrhythmias
Ventricular pre-excitation
Atrial tachyarrhythmia
Long or short QT (QTc = QT/ √HR)
Brugada early repolarization
Bradycardia <30 bpm
Cardiovascular Screening
• Incidence of sudden cardiac death
in NCAA athletes.
• Harmon et al. Circulation 2011
– Case identification (2003-2008)
• NCAA Resolutions List (87%)
• Media Reports (56%)
• Catastrophic insurance claims (20%)
– SCD represented 75% of sudden
death during exercise
What is the Purpose of
Screening?
• Simply to prevent SCD?
• To identify athletes with
cardiovascular conditions at risk
for SCD?
Tenets of Pre-participation
Screening
• Detect potentially lethal CV disease
in athletes to reduce the risk of SCD
and/or disease progression
• Screening aimed to identify silent
disease in a population largely
without signs or symptoms
• Early detection allows early
intervention and management to
reduce morbidity and mortality
ECG Screening
Harmon K, et al. J Electrocardiol. 2015 May-Jun;48(3):329-38.
What ECG can do
• Detect signs of HCM, long QT syndrome,
Brugada syndrome, and WPW
• Has a higher sensitivity for detection than
history or PE
What ECG can not do
• Detect all causes of SCD or prevent all
SCD
• Tell us what the outcome for a patient
would be without intervention
Things to consider
• Who is reading the ECG’s
• What will you do with a positive
test
Other Cardiac Workup
•
•
•
•
•
Echocardiogram
Holter monitor
Cardiac MRI
Exercise stress test
Electrophysiological Testing
AED’s
• AED’s are now commonly found in all
setting of athletic participation
• Use in athletic venues is not usually
for athletes in competition, but
rather spectators
• A small survey showed correction of
arrhythmia occurred in 100% of older
patients, yet only 40% of younger
patients
• AED failed to correct arrhythmia in 2
of 3 young athletes with HCM
Summary
• SCD among young athletes is rare,
but devastating
• It is often the initial presentation of a
cardiac abnormality
• Proper screening is important in
preventing these events by treating
the athletes appropriately or
restricting activity
• Controversy still exists on the most
effective and efficient screening
methods
Summary
• Screen all athletes at the PPE: Hx, PE, EKG
• Work-up all concerning symptoms in
athletes
• Ventricular arrhythmias pose a unique
problem
– Documented vs undocumented
– Structural heart disease vs. normal heart
• Only rare diagnoses will return to activities
• Be aware of the “normal” EKG changes in
well conditioned athletes
• ICD’s provide the greatest risk reduction for
sudden cardiac death in those at risk
Sickle Cell Trait
Inherited disorder in which
you have one gene for
normal hemoglobin and
one gene for sickle
hemoglobin
Exertional Sickling
Sickled red blood cells can
accumulate in the blood
stream during intense
exercise
◦ Block normal blood flow to
tissues and muscle
Sickle Cell Trait
1 in 12 African Americans have sickle cell trait
1 in 2,000 –10,000 Caucasians
3,000,000 Americans have sickle cell trait
Sickle Cell Trait
Linked to sudden death in athletes
Heat, dehydration, altitude, and asthma can
increase and worsen complications associated
with SCT
◦ Even if activity is not intense
SCT is associated with sudden
death
• “Current cumulative evidence is
convincing for associations with
hematuria, renal papillary necrosis,
hyposthenuria, splenic infarction,
exertional rhabdomyolysis, and
exercise-related sudden death.”
– Tsaras G: Complications associated
with sickle cell trait: a brief narrative
review. Am J Med.2009 Jun;122(6):50712. Epub 2009 Apr 24.
SCT and sudden death
• Military:
–Study of >450,000 military recruits (19771981)
–SST+ 30X risk sudden death: {RR 30 (11 –
84)}
Kark et al: NEJM 1987; 317:781.
• Civilian
–NCAA deaths 2004 to 2008; 5 SCT deaths.
–SST+ 15X risk of sudden death.
–DI football players alone, SCT African Americans
(AA) have an RR of 1:805 ; 37x risk AA Division I
football players without SCT.
• Harmon et al: BJSM 2012; In Press
Sickle Cell Trait (SCT)
• The National Collegiate Athletic
Association (NCAA) adopted a
policy requiring Division I
institutions to perform sickle cell
trait testing for all incoming
student athletes. (April 2010)
• Division II (2012)
Current Recommendations
Harmon KG, Drezner JA , Casa DJ: British Journal of Sports
Medicine March 2012.
•
•
•
•
•
•
•
•
•
Targeted screening of high-risk groups
Aggressive educational intervention for athletes with SCT
and those who supervise them
Allowing appropriate time and access for hydration of
athletes
Gradual acclimation to novel activity and the heat
Modification of activity in the heat and at altitude
Appropriate strength and conditioning programs
developed by qualified strength and conditioning coaches
Punitive exercise and conditioning sessions be prohibited
Early recognition of athletes who are struggling, so they
can immediately be allowed to rest and not pushed past
their physiologic limit
Adequate emergency planning for all individuals
responsible for athletes during training and conditioning
Summary
Student-athletes with SCT should not be
excluded from participation
Complications from SCT are not limited to
football
Unlike heat-related or cardiac conditions,
athletes with SCT may present as fatigued and
muscle cramps, but should not be pushed
beyond this point
◦ Can lead to fatal collapse
Thank You