Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Aging brain wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Neuroscience in space wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
End-plate potential wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Electromyography wikipedia , lookup
Synaptogenesis wikipedia , lookup
Synaptic gating wikipedia , lookup
Central pattern generator wikipedia , lookup
Proprioception wikipedia , lookup
Embodied language processing wikipedia , lookup
Microneurography wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Anatomy of the cerebellum wikipedia , lookup
Basal ganglia wikipedia , lookup
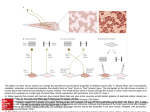
Chapter 32 Control of Motor Function by Nervous System Contents Motor Unit and Final Common Pathway Spinal Reflexes Function of Brain Stem Function of the Basal Ganglion Function of Cerebellum Function of the Cortex organization of motor subsystems Section 1. Motor Unit and Final Common Pathway •Every striated muscle has encapsulated muscle fibers scattered throughout the muscle called muscle spindles. •Extrafusal and intrafusal fibers The extrafusal muscle fibers are innervated by Alpha motor neuron The intrafusal muscle fibers are innervated by Gamma motor neurons Motor units A single motor neuron (a motor) and all (extrafusal) muscle fibers it innervates The physiological functional unit in muscle (not the cell) All cells in motor unit contract synchronously Motor units and innervation ratio Innervation ratio Fibers per motor neuron Extraocular muscle 3:1 Gastrocnemius 2000:1 Purves Fig. 16.4 •The muscle cells of a motor unit are not grouped, but are interspersed among cells from other motor units •The coordinated movement needs the activation of several motors Overview - organization of motor systems Motor Cortex Brain Stem Spinal Cord a-motor neuron Final common pathway Skeletal muscle Final common path - a-motor neuron (-) (+) muscle fibers Transmitter? Schwann cells motor nerve fiber (-) (+) axon hillock Receptors? acetylcholine esterase NM junction Final Common Pathway, a motor pathway consisting of the motor neurons by which nerve impulses from many central sources pass to a muscle in the periphery. Section 2. Spinal Reflexes Somatic reflexes mediated by the spinal cord – May occur without the involvement of higher brain centers – Was facilitated or inhibited by brain For example – Stretch reflex – Deep tendon reflex – Crossed extensor reflex – Superficial reflex Part 1 Stretch Reflex 1 Anatomy of Muscle Spindle 3-10 intrafusal muscle fibers detect change in the length of the muscle -- stretch receptors that report the stretching of the muscle to the spine. The central region and peripheral region of the intrafusal fibers Anatomy of Muscle Spindle Intrafusal fibers are wrapped by two types of afferent endings – Primary sensory endings Type Ia fibers Innervate the center of the spindle – Secondary sensory endings Type II fibers Associated with the ends of the nuclear chain fiber Components of muscle spindle Afferent axons Ia II Nuclear Bag Fiber } Primary ending Secondary } ending Nuclear Chain Fiber Anatomy of Muscle Spindle Primary sensory endings – Type Ia fibers Stimulated by both the rate and amount of stretch (dynamic response) Anatomy of Muscle Spindle Secondary sensory endings – Type II fibers stimulated only by degree of stretch (static response) Anatomy of Muscle Spindle The contractile region of the intrafusal muscle fibers are limited to their ends – only these areas contain actin and myosin filaments – are innervated by gamma () efferent fibers 2. Muscle stretch reflex Muscle stretch reflex Definition: Whenever a muscle is stretched, excitation of the spindles causes reflexive contraction of the same muscle from which the signal originated and also of closely allied synergistic muscle. The basic circuit: Spindle Ia or II nerve fiber dorsal root of the spinal cord synapses with anterior motor neurons a -motor N. F. the same M. from whence the M. spindle fiber originated. Circuit of the Strength Reflex The Stretch Reflex Exciting a muscle spindle occurs in two ways – Applying a force that lengthens the entire muscle – Activating the motor neurons that stimulate the distal ends of the intrafusal fibers to contact, thus stretching the midportion of the spindle (internal stretch) The Stretch Reflex Whatever the stimulus, when the spindles are activated their associated sensory neurons transmit impulses at a higher frequency to the spinal cord The Stretch Reflex The reflexive muscle contraction resists further stretching of the muscle The Stretch Reflex Branches of the afferent fibers also synapse with interneurons that inhibit motor neurons controlling the antagonistic muscles •Inhibition of the antagonistic muscles is called reciprocal inhibition •causes the antagonists to relax The types of the Stretch Flex 1) Tendon reflex (dynamic stretch reflex) Caused by rapid stretch of the muscle, as knee-jerk reflex Transmitted from the IA sensory ending of the M. S. Causes an instantaneous, strong reflexive contraction of the same muscle; Opposing sudden changes in length of the M A monosynaptic pathway being over within 0.7 ms The types of the Stretch Flex 2) Muscle tonus (static stretch reflex): Caused by a weaker and continues stretch of the muscle, Transmitted from the IA and II sensory ending of the M. S. Multiple synaptic pathway, continues for a prolonged period. Non-synchronized contraction, M. C. for at least many seconds or minutes, maintaining the posture of the body. The Stretch Reflex most important in large extensor muscles which sustain upright posture Contractions of the postural muscles of the spine are almost continuously regulated by stretch reflexes (Muscle tonus ) 3 Gamma impact on afferent response Muscle spindle: motor innervation Gamma motoneurons: – Innervate the poles of the fibers. -LOOP Descending influence (UMN) Muscle spindle 1a Activation of the -loop results in increased muscle tone a MUSCLE Functional significance of gamma impact on spindle activity The tension of intrafusal fibers is maintained during active contraction by gamma activity. The system is informed about very small changes in muscle length. Part 2. The Deep Tendon Reflex Structure and Innervation of Golgi Organ Located in the muscle tendon junction. Connective tissue encapsulating collagen fibers and nerve endings. Attached to 10-20 muscle fibers and several MUs. Ib afferent fiber. sensitive to tension Golgi tendon organ: response properties Less frequent than muscle spindle Sensitive to the change of tension caused by the passive stretch or active contraction The Deep Tendon Reflex When muscle tension increases moderately during muscle contraction or passive stretching, GTO receptors are activated and afferent impulses are transmitted to the spinal cord The Deep Tendon Reflex motor neurons in the spinal cord supplying the contracting muscle are inhibited antagonistic muscle are activated The Deep Tendon Reflex cause muscle relaxation and lengthening in response to the muscle’s contraction – opposite of those elicited by stretch reflexes help ensure smooth onset and termination of muscle contraction important in activities involving rapid switching between flexion and extension such as in running Compare spindle and golgi Compare spindle and golgi Part 3. The Crossed Extensor Reflex The reflex occur when you step on a sharp object There is a rapid lifting of the affected foot (ipsilateral withdrawal reflex ) the contralateral response activates the extensor muscles of the opposite leg (contralateral extensor reflex) – support the weight shifted to it Part 4. Superficial Reflexes elicited by gentle cutaneous stimulation dependent upon functional upper motor pathways – Babinski reflex Babinski reflex - an UMN sign Adult response - plantar flexion of the big toe and adduction of the smaller toes Pathological (Infant) response - dorsoflexion (extension) of the big toe and fanning of the other toes Indicative of upper motor neuron damage Part 5. Spinal cord transection and spinal shock Concept: When the spinal cord is suddenly transected in the upper neck, essentially all cord functions, including the cord reflexes, immediately become depressed to the point of total silence. (spinal animal) During spinal shock: complete loss of all reflexes no muscle tone, paralysis complete anesthesia, no peristalsis, bladder and rectal reflexes absent (no defecation and micturition ) no sweating arterial blood Pressure decrease(40 mmHg) the reason: The normal activity of the spinal cord neurons depends on continual tonic excitation from higher centers (the reticulospinal-, vestibulospinalcorticospinal tracts). The recovery of spinal neurons excitability. Section 3. Role of the brain stem Support of the Body Against Gravity – Roles of the Reticular and Vestibular nuclei Facilitated and inhibitory area Areas in the cat brain where stimulation produces facilitation (+) or inhibition (-) of stretch reflexes. 1. motor cortex; 2. Basal ganglia; 3. Cerebellum; 4. Reticular inhibitory area; 5. Reticular facilitated area; 6. Vestibular nuclei. 1. Facilitated area—roles of the reticular and vestibular nuclei.: (1) The pontine reticular nuclei Located slightly posteriorly and laterally in the pons and extending to the mesencephalon Transmit excitatory signals downward into the cord (the pontine reticulospinal tract) 1. motor cortex; 2. Basal ganglia; 3. Cerebellum; 4. Reticular inhibitory area; 5. Reticular facilitated area; 6. Vestibular nuclei. (2) The vestibular nuclei selectively control the excitatory signals to the different antigravity muscle to maintain equilibrium in response to signals from the vestibular apparatus. 1. motor cortex; 2. Basal ganglia; 3. Cerebellum; 4. Reticular inhibitory area; 5. Reticular facilitated area; 6. Vestibular nuclei. MOTOR TRACTS & LOWER MOTOR NEURON MOTOR CORTEX MIDBRAIN & RED NUCLEUS (Rubrospinal Tract) UPPER MOTOR NEURON (Corticospinal Tracts) VESTIBULAR NUCLEI (Vestibulospinal Tract) PONS & MEDULLA RETICULAR FORMATION (Reticulospinal Tracts) LOWER (ALPHA) MOTOR NEURON THE FINAL COMMON PATHWAY SKELETAL MUSCLE Properties of the Facilitated Area Terminate on the motor neurons that exciting antigravity muscle of the body (the muscle of vertebral column and the extensor muscle of the limbs). Have a high degree of natural (spontaneous) excitability. Receive especially strong excitatory signals from vestibular nuclei and the deep nuclei of the cerebellum. Cause powerful excitation of the antigravity muscle throughout the body (facilitate a standing position), supporting the body against gravity. 1. motor cortex; 2. Basal ganglia; 3. Cerebellum; 4. Reticular inhibitory area; 5. Reticular facilitated area; 6. Vestibular nuclei. 2. Inhibitory area –medullary reticular system (1) Extend the entire extent to the medulla, lying ventrally and medially near the middle. (2) Transmit inhibitory signals to the same antigravity anterior motor neurons (medullary reticulospinal tract). 1. motor cortex 2. Basal ganglia 3. Cerebellum 4. Reticular inhibitory area 5. Reticular facilitated area 6. Vestibular nuclei. MOTOR TRACTS & LOWER MOTOR NEURON MOTOR CORTEX MIDBRAIN & RED NUCLEUS (Rubrospinal Tract) UPPER MOTOR NEURON (Corticospinal Tracts) VESTIBULAR NUCLEI (Vestibulospinal Tract) PONS & MEDULLA RETICULAR FORMATION (Reticulospinal Tracts) LOWER (ALPHA) MOTOR NEURON THE FINAL COMMON PATHWAY SKELETAL MUSCLE (3) Receive collaterals from the corticospinal tract, the rubrospinal tracts, and other motor pathways. These collaterals activate the medullary reticular inhibitory system to balance the excitatory signals from the pontine reticular system. 1. motor cortex 2. Basal ganglia 3. Cerebellum 4. Reticular inhibitory area 5. Reticular facilitated area 6. Vestibular nuclei. Areas in the cat brain where stimulation produces facilitation (+) or inhibition (-) of stretch reflexes. 1. motor cortex; 2. Basal ganglia; 3. Cerebellum; 4. Reticular inhibitory area; 5. Reticular facilitated area; 6. Vestibular nuclei. Decerebrate Rigidity • Decerebrate Rigidity: transection of the brainstem at midbrain level (above vestibular nuclei and below red nucleus) • Symptoms include: – extensor rigidity or posturing in both upper and lower limbs •Results from: –loss of input from inhibitory medullary reticular formation (activity of this center is dependent on input from higher centers). –active facilitation from pontine reticular formation (intrinsically active, and receives afferent input from spinal cord). •The extensor rigidity is -loop dependent –section the dorsal roots interrupts the -loop, and the rigidity is relieved. This is -rigidity. THE -LOOP? Descending influence (UMN) Muscle spindle 1a Activation of the -loop results in increased muscle tone a MUSCLE Section 4. The Cerebellum and its Motor Functions Cerebellar Input/Output Circuit Function of the cerebellum Based on cerebral intent and external conditions – tracks and modifies millisecond-to-millisecond muscle contractions – produce smooth, reproducible movements Without normal cerebellar function, movements appear jerky and uncontrolled Functional Divisions-cerebellum • Vestibulocerebellum (flocculonodular lobe) The vestibulocerebellum input-vestibular nuclei output-vestibular nuclei Function 1: Control of the equilibrium and postural movements. controlling the balance between agonist and antagonist M. contractions of the spine, hips, and shoulders during rapid changes in body positions. Function 1: Control of the equilibrium and postural movements. (Cont.) During running Receive the signals from the periphery how rapidly and in which directions the body parts are moving Calculate the rates and direction where the different parts of body will be during the next few ms. anticipatory correction (feed-forward control) the key to the brain’s progression to the next sequential movement. Function 2 regulate the eye movement – Through vestibulo-ocular reflex keep the eyes still in space when the head moves – Damage of the flocculonofular lobe result in positional nystagmus (位置性眼震颤) The VOR: Definition A eye movement reflex Stimulated by head movements Moves the eyes opposite of the head Helps keep the retinal image stabilized The VOR contributes to clear vision during head movements Cerebellar Nystagmus Horizontal oscillating eye movement •Spinocerebellum (vermis & intermediate) •Spinocerebellum (vermis & intermediate) –input–somatic sensory information via spinocerebellar tracts –Branch from corticospinal tract –Output –Thamalus – motor cortex –-fastigial (顶) and interposed(中间 核) nuclei → vestibular nuclei, reticular formation and red nucleus → vestibulospinal tract, reticulospinal tract and rubrospinal tract → motor neurons of anterior horn Function of spinocerebellum Provide the circuitry for coordinating the movements of the distal portions of the limbs, especially the hands and fingers – Compared the “intentions ” from the motor cortex and red nucleus, with the “performance” from the peripheral parts of the limbs – Send corrective output signals to the motor neurons – Provides smooth, coordinate movements – Feedback control •Cerebrocerebellum (lateral zone) input- from the cerebral cortex via a relay in pontine nuclei output- to dentate nucleus → dorsal thalamus and red nucleus→ primary motor cortex → corticospinal tract → motor neurons of anterior horn Cerebrocerebellum (functions) Planning and programming of sequential movements – Panning (计划形成): begins in the sensory and promotor area of the cortex and transmitted to the cerebrocerebellum – Programming (运动程序编制): what will be happening during the next sequential movement a fraction of the second later…. •Vestibulocerebellum (flocculonodular lobe) Balance and body equilibrium •Spinocerebellum (vermis & intermediate) Rectify voluntary movement •Cerebrocerebellum (lateral zone) Plan voluntary movement Clinical Abnormalities of the Cerebellum Dysmetria (辨距障碍) and Ataxia (共济失调) Past pointing: (过指) Failure of progression – Dysdiadochokinesia (轮替运动障碍) – Dysarthria (构音障碍) Intention tremor Dysmetria (辨距障碍) and Ataxia (共济失调) Past Pointing Dysdiadochokinesia (轮替运动障碍) Intention Tremor Present during reaching movement Not at rest Section 5 The motor functions of basal ganglia Components of Basal Ganglia Caudate Putamen GPe GPi 1. Corpus Striatum(纹状体) Caudate Nucleus (尾状核) Putamen (壳核) Globus Pallidus (苍白球,GP) Components of Basal Ganglia 2. Substantia Nigra (SN) Pars Compacta (SNc) Pars Reticulata (SNr) STN 3. Subthalamic Nucleus (STN) SN (r & c) Basal Ganglia Connections •Circuit of connections –cortex to basal ganglia to thalamus to cortex –Helps to program automatic movement sequences (walking and arm swinging or laughing at a joke) •Output from basal ganglia to reticular formation –reduces muscle tone –damage produces rigidity of Parkinson’s disease cortex to basal ganglia to thalamus to cortex somatosensory cortices motor cortices excitation D1 Putamen inhibition D1 & D2 GPe Dopamine receptors D2 GPi Thalamus STN GPe/i: Globus pallidus internal/external STN: Subthalamus Nucleus SNc: Pars Compacta SNc (part of substantia Nigra) • Direct Pathway: – Disinhibition of the thalamus facilitates cortically mediated behaviors somatosensory cortices motor cortices excitation inhibition D1 Putamen D1 & D2 Dopamine receptors GPe D2 GPi Thalamus GPe/i: Globus pallidus internal/external STN: Subthalamus Nucleus STN SNc: Pars Compacta (part of substantia nigra)) SNc •Indirect pathway: –Inhibition of the thalamus inhibits cortically mediated behaviors somatosensory cortices motor cortices excitation D1 Putamen inhibition D1 & D2 GPe Dopamine receptors D2 GPi Thalamus STN SNc GPe/i: Globus pallidus internal/external STN: Subthalamus Nucleus SNc: Pars Compacta (part of substantia nigra) Medical Remarks • Hypokinetic disorders result from overactivity in the indirect pathway. example: Decreased level of dopamine supply in nigrostriatal pathway results in akinesia, bradykinesia, and rigidity in Parkinson’s disease (PD). somatosensory cortices motor cortices excitation inhibition Putamen D1 D1 & D2 Dopamine receptors GPe D2 GPi GPe/i: Globus pallidus internal/external Thalamus STN SNc STN: Subthalamus Nucleus SNc: Pars Compacta (part of substantia nigra) Parkinson’s Disease PD Disease of mesostriatal dopaminergic system Muhammad Ali in Alanta Olympic normal Parkinson’s Disease Substantia Nigra, Pars Compacta (SNc) DOPAminergic Neuron Clinical Feature (1) Slowness of Movement - Difficulty in Initiation and Cessation of Movement Parkinson’s Disease Clinical Feature (2) Resting Tremor Parkinsonian Posture Rigidity-Cogwheel Rigidity •Hyperkinetic disorders result from underactivity in the indirect pathway. example: Lesions of STN result in Ballism. Damage to the pathway from Putamen to GPe results in Chorea, both of them are involuntary limb movements. somatosensory cortices motor cortices excitation D1 Putamen inhibition D1 & D2 GPe Dopamine receptors D2 GPi Thalamus STN GPe/i: Globus pallidus internal/external STN: Subthalamus Nucleus SNc: Pars Compacta SNc (part of substantia nigra) SYDENHAM’S CHOREA (风湿性舞蹈病) Clinical Feature - Fine, disorganized , and random movements of extremities, face and tongue - Accompanied by Muscular Hypotonia - Typical exaggeration of associated movements during voluntary activity - Usually recovers spontaneously in 1 to 4 months Principal Pathologic Lesion: Corpus Striatum HUNTINGTON’S CHOREA 亨廷顿舞蹈症 Clinical Feature - Predominantly autosomal dominantly inherited chronic fatal disease (Gene: chromosome 4) - Insidious onset: Usually 40-50 - Choreic movements in onset - Frequently associated with emotional disturbances - Ultimately, grotesque gait and sever dysarthria, progressive dementia ensues. Principal Pathologic Lesion: Corpus Striatum (esp. caudate nucleus) and Cerebral Cortex HEMIBALLISM (半侧投掷症) Clinical Feature Lesion: Subthalamic - Usually results from CVA (Cerebrovascular Accident) involving subthalamic nucleus - sudden onset - Violent, writhing, involuntary movements of wide excursion confined to one half of the body - The movements are continuous and often exhausting but cease during sleep - Sometimes fatal due to exhaustion - Could be controlled by phenothiazines and stereotaxic Nucleus surgery Section VI Control of muscle function by the motor cortex •Two principal components –Primary Motor Cortex –Premotor Areas The primary motor cortex The topographical representations of the different muscle areas of the body in the primary motor cortex Characteristics of the PMC: 1, It has predominant influence on the opposite side of the body (except some portions of the face) 2. It is organized in a homunculus pattern with inversed order 3. The degree of representation is proportional to the discreteness (number of motor unit) of movement required of the respective part of the body. (Face and fingers have large representative) 4. Stimulation of a certain part of PMC can cause very specific muscle contractions but not coordinate movement. •Projects directly –to the spinal cord to regulate movement –Via the Corticospinal Tract –The pyramidal system •Projects indirectly –Via the Brain stem to regulate movement –extrapyramidal system Descending Spinal Pathways pyramidal system Direct Control muscle tone and conscious skilled movements Direct synapse of upper motor neurons of cerebral cortex with lower motor neurons in brainstem or spinal cord Descending Spinal Pathways extrapyramidal system Indirect coordination of head & eye movements coordinated function of trunk & extremity musculature to maintaining posture and balance Synapse in some intermediate nucleus rather than directly with lower motor neurons • Premotor area composed of supplementary motor area and lateral Premotor area Premotor Areas •Receive information from parietal (顶) and prefrontal (前) areas •Project to primary motor cortex and spinal cord •For planning and coordination of complex planned movements