Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuroplasticity wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Donald O. Hebb wikipedia , lookup
Apical dendrite wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Human brain wikipedia , lookup
Neuroeconomics wikipedia , lookup
Optogenetics wikipedia , lookup
Environmental enrichment wikipedia , lookup
Memory consolidation wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Reconstructive memory wikipedia , lookup
Affective neuroscience wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Time perception wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Basal ganglia wikipedia , lookup
Aging brain wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Orbitofrontal cortex wikipedia , lookup
Spike-and-wave wikipedia , lookup
Hypothalamus wikipedia , lookup
Hippocampus wikipedia , lookup
Synaptic gating wikipedia , lookup
Emotional lateralization wikipedia , lookup
Temporal lobe epilepsy wikipedia , lookup
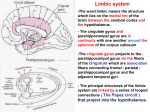
Chapter 18; pp. 820-838 Limbic System 1. Mesocortex = limbic cortex Cingulate gyrus, parahippocampal gyrus, temporal pole Transition from 3- to 6-layered cortex Allocortex (Archicortex and Paleocortex) Hippocampus, 3-layered 2. 3. Corticoid Areas Amygdala, no consistent layering i. There are four parts to the amygdala, including bed nucleus of stria terminalis 4. Review MRI sections!!! (don’t worry about gross vertical slices) 5. Pathways by which the hippocampus talks to the thalamus: fornix Pathways by which the amygdala communicates with hypothalamus: Stria terminalis & ventral amygdalofugal pathways Olfaction pathway: Olfactory nerve => mitral and tufted cells => primary olfactory cortex (piriform & amygdaloid cortices) and amygdala => orbitofrontal olfactory area Components of the hippocampal formation: Dentate gyrus, hippocampus, and subiculum 6. 7. 8. 9. Intrinsic Hippocampal formation circuit: Entorhinal cortex =perforant pathway=> i. Also E.C. =alvear pathway=> CA1 & CA3 Dentate gyrus (granule cell layer) =mossy fibers=> CA3 =Schaffer collaterals=> i. Also CA3 => fornix CA1 => Subiculum => i. Also subiculum => fornix Entorhinal cortex In which part of the above circuit does long-term potentiation occur? LTP occurs in the perforant pathway and Schaffer collaterals What is the Hebb Rule? The Hebb Rule can be paraphrased as: “Fire together, wire together” ---synaptic strength increases due to a growth change or metabolic process occurs in neurons when a presynaptic cell repeatedly stimulates the postsynaptic neuron What kind of neurons from the medial septal nucleus and diagonal band nucleus are modulatory inputs to the hippocampus? These neurons release acetylcholine 10. 11. 12. 13. Inputs to hippocampus: frontal, parieto-occipital, temporal association cortices Output from hippocampus via entorhinal cortex: Multimodal association cortex Output from hippocampus via subiculum (and then fornix): Diencephalon and septal nuclei 14. 15. 16. 17. [emotional end of the line] Parts of fornix, inferior/~anterior to superior/posterior: Hipppocampal formation => fimbria => crura =(commissure)=> body=> columns => => postcommisural fornix => medial and lateral mamillary nuclei, => precommisural fornix => lateral septal nuclues, => or anterior thalamic nucleus Papez Circuit: Fornix => => Anterior thalamic nucleus =internal capsule=> cingulate gyrus => back to hippocampal formation Holguin sez: Know CT/MRI, but not vertical slice Doesn’t really test olfaction Star hippocampus and dementia Hebb Rule Choline modulates memory Memory Disorders 18. Although unilateral lesions of the medial temporal or diencephalic lobes do not produce severe amnesia, what happens after a lesion in the dominant side? Nondominant? Verbal memory defecits [think Wernicke’s and Broca’s areas] Visual-spatial memory [remember hemineglect from nondominant lesion in Ch. 10] 19. What part of the brain is important for habit learning? Caudate nucleus 20. How is information consolidated in the neocortex? (Through rehearsal?) by the medial temporal and diencephalic strucures (thalamus) i. Gradually shifts location to neocortex over the course of years 21. What arteries suply the medial thalami? PCA branches: paramedian thalamoperforator arteries i. Sometimes there is only one: “artery of Percheron” So lesions at the top of the basilar artery cause bilateral or unilateral infarcts 22. Describe transient global amnesia: Lasts 4-12 hours, abrupt global amnesia, afterwards permanent loss of memory for a few hours before and after the event, usually nevere happens again 23. Which nucleus of the amygdala has direct and indirect connections all over the brain? Which is connected to the olfacotry bulb and forebrain areas controlling appetite? Which is important in autonomic control (hypothalamus and brainstem)? Basolateral Corticomedial [think: mead-ial] Central 24. What syndrome appears after bilateral lesions of the amygdala? Kluver-Bucy syndrome 25. How does the amygdala connect to the medial orbitofrontal and cingulate cortices? Via the uncinate fasciculus 26. What are the two pathways from the amygdala to subcortical regions? What do they transmit? How does the amygdala talk to the brainstem? Stria terminalis – transmits olfactory information to hypothalamus in order to modulate appetite ventral amygdalofugal pathway – emotion, motivation, cognitive function, homeostasis i. connects nucleus basalis, septal nuclei, ventral striatum, and thalamus medial forebrain bundle – amygdala & hypothalamus brainstem 27. How does an auditory cortex seizure manifest? Auditory association cortex? Differences btw. Sides? Positive or negative signs, contralateral Voices or music, sometimes speech Musical hallucinations are more common in nondominant hemisphere seizure 28. Todd’s paresis = Focal weakness post-ictal 29. Frontal motor association cortex seizure can cause: Fencing posture or other complex posturing 30. What is a complex partial seizure? Loss of conciousness, plus the motor/somatosensory/autonomic/psychic symptoms of a simple partial seizure Or secondary generalization 31. How do you localize a temporal lobe partial seizure, with side 1 exhibiting automatisms (repetetive behaviours), and side 2 showing dystonia or immobility? Side 1 (movement) is ipsilateral to focus The basal ganglia contralateral to paralysis get fried 32. Absence seizure EEG shows: 3-4 hertz spike and wave discharges 33. What are the three top causes of seizure in the elderly? What electrolyte abnormalities cause seizure? Cerebrovascular disease, tumors, and neurodegenerative disorders Hypoglycemia, hyponatremia, hypernatremia, hypocalcemia, and hypomagnesmia 34. How can a febrile seizure cause temporal lobe epilepsy? How does it develop in time? Complex febrile seizure (longer than 15 minutes or multiple in a day) cause medial temporal sclerosis or hippocampal sclerosis Latent period of up to a few years before onset of complex partial seizures 35. What is Rolandic epilepsy? What appears on EEG? Focal, nocturnal seizures in children, remits by 15 years, AD inheritance EEG shows centrotemporal spikes 36. What is a Wada test? Injection of sodium amytal is used to sedate one half of the brain, after which language skills are tested in order to determine the dominant hemisphere In patients with a nonfunctional medial temporal lobe, injection of the good side causes severe memory difficulties i. Since common carotid is injected (and PCA continues to supply the medial temporal lobe) we think loss of input causes memory issues 37. When is callosotomy done? To stop generalization from occuring during a seizure, used to prevent falls in injury-prone patients 38. Defects associated with Schizophrenia? OCD? Depression? Small amygdala, hippocampus, parahyppocampal gyrus ,and basal ganglia; low DA neurotransmission Increased activity in the caudate nucleus, low 5-HT Decreased noradrenaline and 5-HT; increased cortisol, some other NTs