Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
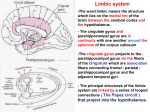
REVIEW OF LIMBIC SYSTEM, HYPOTHALAMUS, THALAMUS, CORTEX Dr. G.R. Leichnetz Hippocampus Hippocampal Formation: Hippocampus Proper + Dentate Gyrus + Subiculum The subiculum is a transition region between paleo- and archi-cortex. CA2 CA3 Hippocampus Dentate gyrus proper CA1 Fimbria of fornix Subiculum Hippocampal Formation The hippocampus proper consists of CA1-CA3 subfields. The dentate gyrus consists of CA4 plus the “dentate fascia,” ie. molecular and granular layers of the dentate gyrus. Entorhinal cortex Hippocampal Connections: Principal Afferents: Entorhinal Cortex Principal Efferents: Fornix The entorhinal cortex receives major multimodal input (somatosensory, visual, auditory) from associational cortex, and relays that information into the hippocampus for memory processing. Prefrontal assoc. cortex Temporal assoc. cortex Parieto-occipital assoc. cortex Entorhinal Afferents The precommissural fornix terminates in the septum/ basal forebrain region. The postcommissural fornix projects to hypothalamus, mammillary body, and paramedian midbrain reticular formation (midbrain limbic area, raphe). The fornix to the mammillary body is the first segment of “Papez Circuit,” followed by the mammillothalamic tract to anterior nucleus of thalamus, cingulate gyrus, and cingulum bundle to hippocampus. Cingulate gyrus cingulum Ant. Nuc. MTT Mamm. Body Hippoc. fornix Bilateral lesions of the hippocampus produce anterograde amnesia, an inability to learn new information. Past memories largely intact. The CA1 subfield (Sommer’s sector) is vulnerable to vascular injury. Wernicke’s encephalopathy (from a vitamin B1 thiamin deficiency) produces focal vascular hemorrhages in structures associated with Papez circuit (eg. mammillary bodies, anterior nucleus of thalamus) and results in Korsakoff’s syndrome with anterograde amnesia. Amygdala The amygdala is located in the ventromedial temporal lobe (rostral to the hippocampus) within the rostral parahippocampal gyrus. C The amygdala consists of numerous subnuclei, and thus is referred to as the “amygdaloid complex”. MEDIAL LATERAL AMYGDALOID AFFERENTS 1. Multimodal Sensory Inputs- via relay in adjacent temporal cortex, informs the amygdala about ongoing sensory experience 2. Direct Olfactory Input- from olfactory bulb Normal sensory “percepts” interact with the amygdala to be “tagged” with an appropriate emotional or motivational significance. AMYGDALOID EFFERENTS Cortical EfferentsThe amygdala has feedback projections to multimodal associational cortex (eg. prefrontal, parietal, temporal) to bring “emotional salience” to ongoing sensory experience (enhances attention). From: Purves et al AMYGDALOID EFFERENTS Subcortical Efferentsvia stria terminalis & ansa peduncularis to: Hypothalamus- feeding/appetite, reproductive behavior, endocrine releasing factors Mediodorsal nucleus of thalamus- relay to prefrontal cortex (for emotional effects on mood personality, social behavior, working memory) Basal forebrain (nuc. accumbens)- addiction, pleasure/ reward Brainstem autonomic nuclei- effects on autonomics (cardiac, respiratory) “Tagging” behaviors with emotion The amygdala receives direct olfactory input, and other multimodal (visual, auditory, somatosensory) input via relay in adjacent temporal cortex. Its subcortical efferents follow two paths: stria terminalis and ansa peduncularis. Noback AMYGDALOID LESION Amygdaloid stimulation produces aggression Temporal lobe lesions which involve the amygdala result in Kluver-Bucy Syndrome, producing lack of emotion, fear; inability to discriminate between food and non-food objects, hypersexuality. (fundamentally this is an inability to comprehend the emotional significance of objects, so they use them inappropriately) Septum/ Basal Forebrain The precommissural septum is a small gyrus in the caudal frontal lobe, rostral to the anterior commissure. It is a major nexus of the limbic system with the basal ganglia. Fornix AC Hypothalamus MB The precommissural septum is contiguous with the basal forebrain. The septum/basal forebrain region contains the nucleus accumbens and numerous cholinergic nuclei (Ch1-Ch4). Caudate Putamen S Ch1Ch3 Ch4 Nucleus basalis NA Basal forebrain The nucleus accumbens is the largest nucleus of the septum/basal forebrain, and is the “center for addiction.” It receives the DA mesolimbic “reward system” from the ventral tegmental area of the midbrain. C IC P ACC Basal forebrain S The mesolimbic and mesocortical tracts, which originate from the VTA (A10) traverse the medial forebrain bundle in the lateral hypothalamus to reach the nucleus accumbens and prefrontal cortex. PFC ACC Mesocortical VTA Mesolimbic Traverse the medial forebrain bundle The nucleus accumbens has been called a “center for addiction.” It receives the major dopaminergic “reward system” (mesolimbic) projections from the ventral tegmental area of the midbrain. Its neurons have receptors to most chemical substances of abuse (opioids, nicotine), but also is activated by other pleasurable experiences (eg. food, even music). Amygdaloid projections to accumbens bring “emotional” component to addiction. Functional MRI studies show that the amygdala and nucleus accumbens are activated even in the absence of cocaine if the subject “imagines” the emotional high. The medial forebrain bundle carries afferents to, and efferents from, the septum/ basal forebrain. MFB LC Ascending NE projections from the locus ceruleus (A6) and cell groups A5, A7 traverse the MFB MFB CELL GROUPS A5, A7 MFB MIDBRAIN RAPHE (B7,B8) Ascending 5-HT (serotonergic) projections from the midbrain raphe traverse the MFB SEPTUM/BASAL FOREBRAIN Afferents Medial Forebrain Bundle (DA, NE, 5-HT) Fornix (from hippocampus) Stria terminalis, ansa peduncularis (from amygdala) Efferents Medial Forebrain Bundle (ACh) (to hypothalamus, and brainstem Reciprocal thru fornix (to hippocampus) and stria terminalis, ansa peduncularis (to amygdala) ACh projections (Ch4)- to cerebral cortex The medial forebrain bundle carries cholinergic projections from nuclei in the septum/basal forebrain (Ch1-Ch3) to the hypothalamus and brainstem reticular formation. Medial forebrain bundle Ch1-Ch3) From: Niewenhuys, The Human Nervous System The nucleus basalis of Meynert (Ch4), located in the basal forebrain, is the principal source of cholinergic innervation of the cerebral cortex. This nucleus shows a profound loss of neurons in Alzheimer’s disease. Ch4 Prefrontal Cortex The prefrontal cortex is the “neocortical representative of the limbic system.” It receives major limbic input from the amygdala via the MD nucleus of the thalamus. It is involved in “working memory,” and complex behavioral responses where the individual considers the consequences of his/her actions. “Strategy for behavior” Lesion: perseveration, anti-social behavior, mood & personality aberrations The prefrontal cortex receives a major input from the mediodorsal (MD) nucleus of the thalamus, which conveys limbic influence from the amygdala. PFC MD The “delayed response test” has classically been a used to evaluate prefrontal function, eg. after brief delay period, food reward changes compartments Lesions result in perseveration. Cannot alter behavioral strategy. Working memory refers to the process of actively maintaining relevant information in mind for brief periods of time. Prefrontal Functions: Executive functions- cognition, decision-making Working memory Social behavior Modified from Purves Hypothalamus Hypothalamus Anterior region Tuberal region Posterior region The hypothalamus is located in the ventral diencephalon, and is a collection of subnuclei involved in higher-level (the most complex) autonomic, visceroendocrine functions. The anterior region (preoptic area) merges into the basal forebrain. The tuberal region are nuclei grouped over the tuber cinereum (median meinence). The posterior region includes the mammillary nuclei. The principal afferents of the hypothalamus come from the hippocampus (fornix), amygdala (stria terminalis and ansa peduncularis), and septum/basal forebrain (medial forebrain bundle). Stria terminalis Fornix Medial forebrain bundle Septum/ Basal Forebrain Amygdala Hippocampus The hypothalamus receives major input from the amygdala thru the stria terminalis and ansa peduncularis through which emotion affects hypothalamic functions. Noradrenergic (NE) cell groups (A1-A5, A7) in the lateral pontine and medullary reticular formation project to the hypothalamus. Hypothalamus A1-A5, A7 Hypothalamus: Function of Particular Nuclei Direct projections from the retina to the hypothalamus; to the suprachiasmatic nucleus, the “biological clock” responsible for the brain’s circadian rhythmicity. It receives direct retinal input. Suprachiasmatic nucleus Optic Chiasm The supraoptic and paraventricular nuclei of the hypothalamus produce vasopressin (ADH) and oxytocin which are transported through the axons of the hypothalamohypophyseal tract to be released in the posterior lobe of the pituitary (neurohypophysis). PV SO Paraventricular nucleus Supraoptic nucleus RF-producing cell groups end in the arcuate nucleus Intrinsic hypothalamic neurons that synthesize “releasing factors” terminate in the arcuate nucleus of the median eminence, and RF’s reach the anterior lobe of the pituitary (adenohypophysis) via the hypothalamohypophyseal portal system. The ventromedial nucleus of the hypothalamus functions as a “satiety center.” VMH Lesion of the ventromedial nucleus of the hypothalamus results in hypothalamic obesity. Hypothalamic obesity Thalamus The internal medullary lamina of the thalamus divides the thalamus into medial and lateral nuclear groups. The lateral nuclear group is subdivided into dorsal and ventral tiers (containing specific relay nuclei). The thalamus is the principal source of cortical afferents (corticopetal projections). All thalamocorticals are glutamatergic (excitatory). The ventral tier of the lateral group contains the specific relay nuclei. VA- from GP; to SMA (area 6) VLfrom cerebellum to area 4 VPfrom SL, ML; to area 3,1,2 LGNfrom OT; to area 17 MGN- from IC, br. IC to areas 41, 42 A- from MTT; to cingulate gyrus MD- from amygdala to PFC Basic Pattern Of Thalamic Connections Thalamocorticals Corticothalamics Thalamus All thalamic nuclei (except the thalamic reticular nucleus) have reciprocal connections with the cerebral cortex. Thalamocorticals project to lamina IV of the cortex. Corticothalamics that project back to the thalamus originate in lamina VI of the cortex. Thalamic Pain Syndrome Central neurogenic pain (not caused by activity in peripheral sensory fibers) can be caused by lesions that interrupt the somatosensory pathway at any level. A destructive lesion that involves the ventral posterior nucleus of the thalamus may result in the thalamic pain syndrome characterized by exaggerated and exceptionally disagreeable responses to cutaneous stimulation. Cerebral Cortex There is a complete representation of the body on the pre- and post-central gyri, called the motor and sensory homunculus. The leg is represented on the medial aspect of the hemisphere in the paracentral lobule. Brodmann (1909) identified about 50 cytoarchitecturally distinct regions in the cerebral cortex: Brodmann’s areas. These numbers have become synonymous with the regions. From Wilkinson Associational fibers originate in lamina III pyramidal cells. Short associational fibers (U-fibers) interconnect adjacent gyri. Long associational bundles interconnect distant lobes. Commissural fibers originate from lamina III pyramidal cells. There are three major cerebral commissures: corpus callosum, anterior commissure, and hippocampal commissure. The corpus callosum interconnects regions above the superior temporal gyrus. The anterior commissure interconnects lower temporal regions. The principal source of cortical afferents is the thalamus. Corticopetal projectional fibers (thalamocorticals) traverse the internal capsule to reach the cortex. Corticofugal projections originate from layer V pyramidal neurons, including corticospinals, corticobulbars, corticopontines, corticostriates. Only corticothalamics originate in layer VI. Associational Corticostriate Commissural Corticopontine Corticospinal Corticobulbar Corticothalamic Descending projectional fibers traverse the internal capsule en route to the brainstem. Frontal corticofugals traverse the anterior limb, while parietal & occipital corticofugals traverse the posterior limb. The superior parietal lobule provides essential information on body image to the premotor cortex. Lesions of the SPL result in apraxia (inability to perform learned movements in the absence of paralysis). The left hemisphere is dominant for language in about 98% of the population. Broca’s motor speech area is in the inferior frontal gyrus. Wernicke’s area for language comprehension is in the parieto-occipito-temporal region. The arcuate fasciculus (associational fibers) connects Wernicke’s area to Broca’s area. Broca’s Area Wernicke’s Area Aphasias= language dysfunctions Receptive Aphasias: lesions of Wernicke’s area; difficulties with language comprehension, recognition of symbols of language (visual, auditory, somatosensory) 1. Tactile Agnosias (astereognosis)- supramarginal gyrus 2. Visual Agnosias (word blindness)- angular gyrus 3. Auditory Agnosias (word deafness)- caudal part of superior temporal gyrus Expressive Aphasias: lesions of Broca’s area; disruption of speech production; poor syntax; word omissions; normal comprehension of language, but speech is labored. When asked to make drawings, the patient with a parietal lesion (unilateral neglect) draws all the numbers on a clock face on the ipsilateral side, or only draws the ipsilateral side of the body in a stick figure. Attention Lesion of the posterior parietal cortex can produce hemi-inattention syndrome