Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Urban legends about drugs wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Dextropropoxyphene wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
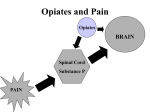
Opiates Opiate Overview • Opiates are derived from the poppy plant (Papaver somniferum) first cultivated in Mesopotamia (the ‘joy plant’) • Opium = crude resinous exudate, often dried and powdered, can be used unprocessed • Used for medicinal purposes (pain relief, diarrhea, etc.) and for recreation • Active ingredients include over 25 alkaloids, most importantly morphine (10% of opium), codeine (3% of opium), and thebaine Continued • Opiates include opium, morphine, codeine, derivatives (e.g. diacetylmorphine or heroin) and synthetics (e.g. methadone) • Refinement of opium – Morphine made from opium - increased strength 10X – Heroin refined from morphine (more lipid soluble), made it even stronger (3X) – Codeine 1/5 the strength of morphine Use and Abuse Pain medication is the second most common type of drug abuse in adolescents and adults behind marijuana. Use and Abuse (cont) Generation RX According to the Partnership for a Drug Free America, the most popular prescription drug abused by teens is Vicodin followed by Oxycontin. Common Pharmacokinetics • Opiates administered by various routes – – – – Oral: 20-30 min to reach brain Insufflated: 5-8 min IV: 15-30 seconds Smoked: 7-10 seconds • Metabolized into active and inactive components by kidneys • Eliminated mostly in urine Opiate Effects • Opiates inhibit brain centers (depress CNS activity) controlling: – pain, coughing, breathing, heart rate and intestinal motility. • Opiates depress nerve transmission in sensory pathways of the spinal cord and brain that signal pain. • Widening of blood vessels (vasodilation - produces a warm feeling, sweating, reduces bowel activity) • Overall lethargy and lack of motivation • At high doses, sedation occurs (overdose results in coma, unconsciousness, death) • Combined with other depressants (e.g., alcohol) can be deadly (>50% of overdose cases involve alcohol) Transmission of Pain • Stimulus Nocioceptors • Nocioceptors are ~ 80% C fibers (unmyelinated – slow pain) and 20% A delta fibers (cold/pressure/fast pain). • About 50% of sensory fibers have nocioceptive functions. • C fibers are blocked in the presence of opiates. • A delta fibers are unaffected by opiates Acute/Chronic Effects SYSTEM ACUTE CHRONIC CNS Analgesia Euphoria Sedation Cough suppression Dependence Peripheral Neuropathy Spinal disease Visual impairment Mood instability Respiratory Respiratory depression Respiratory disease (pneumonia, TB) Gastrointestinal Decreased propulsions Decreased digestive secretions Constipation Eyes Pupillary contraction Kidneys Inhibition of urinary voiding reflex Kidney disease Sexual Reduced libido Irregular menstruation Pharmacodynamics • Opiates bind to opioid receptors, including the – mu, delta, epsilon, kappa receptors • These G-proteincoupled receptors are involved in the transmission of pain signals. Neurotransmitters Endorphins, Dynorphins, Enkephalins,… • Called natural opiates • Involved in glucose regulation • natural neural peptides that bind to opioid receptors to produce euphoric effects • Released by brain when exposed to opiates Neurotransmitters GABA • Affects dopaminergic cells • Opiates and opioid NTS’s activate the presynaptic opioid receptors on GABA neurons • This inhibits the release of GABA in the VTA • Inhibiting GABA allows the dopaminergic neurons to fire faster Morphine first isolated in 1804 by Friedrich Serturner • Direct/indirect agonist • Most often administered subcutaneously; also smoked, taken orally, or via mucosa • Not very lipid soluble, doesn’t cross BBB easily "Oh, jab me with your needle a hundred times And a hundred times I will bless you, Saint Morphine" Jules Verne (1828 - 1905) Codeine (methylated morphine) • Direct/indirect agonist • Alkaloid found naturally in opium in low concentrations (0.1-2%); usually synthesized from morphine • Usually administered orally • 0.1 times as potent as morphine • Converted into morphine after crossing BBB • Used for cough suppression, diarrhea, moderate pain Heroin (diacetylmorphine) • Direct/indirect agonist • Synthesized from morphine • Administered IV, SC, snorted or smoked • IV and smoked lead to fast onset and “rush” • 3 times as potent as morphine • Not directly an efficacious mu agonist, but more lipid soluble than morphine • Enters brain quickly, converted into morphine for action Methadone (methadone hydrochloride) • Partial agonist • Completely synthetic • Orally administrated • Mild/moderate effects over long time period (days) • Used in treatment of opiate addiction to prevent withdrawal and craving • Minimizes effects of short-term opiates taken under influence of methadone Methadone treatment • • • • • Safer, less contaminated Taken orally - avoids injection No worries about where next hit is coming from Lasts longer in the body (taken once a day) Allows withdrawal from drug use with less discomfort • Reduces criminal activity • Cuts connection with drug scene • It’s cheaper Oxycodone • Opioid Analgesic • Synthesized from opium-derived thebaine; structurally similar to codeine • Ingested orally in tablet form • Schedule II controlled substance • Can only be legally obtained by prescription • OxyContin is time release oral oxydodone. Vicodin • Narcotic Analgesic • Hydrocodone bitartrate (opioid analgesic) and Acetaminophen (non-opiate analgesic) • Ingested orally in tablet form • Schedule III controlled substance • Can only be legally obtained by prescription Naloxone (Narcan) • Synthetic direct antagonist • Administered IV; onset = 2 min • Few low-dose effects on normal persons • Rapidly precipitates withdrawal in opiate-dependent persons • Elicits tobacco craving in dependent individuals • Used to reverse respiratory depression from overdoses Naltrexone (Trexan) • Direct antagonist • Administered orally • Works like naloxone but since oral more useful for long-term • Used after recovery from withdrawal period (also used to treat alcoholism) • Prevents opiate agonists from having an effect Tolerance • Develops to respiratory depression, analgesia, euphoria, sedation • Little tolerance to pupil-constriction and constipation • Profound behavioral/associative tolerance • Cross-tolerance develops between different opiates and between opiates and opioids Mechanisms for Tolerance • Downregulation (conversely, antagonists upregulate) • Decreased receptor sensitivity • Reduced synthesis of opioid peptides • Also, another possible mechanism, based on synthesis... Change in Opioid Synthesis 1) POMC yields two major species of betaendorphins, “normal” longer form and shorter form; in brains of normal rats ratio between 1:1 and 1.5:1 (normal:short) 2) Hammonds et al. (1984) showed short version seems to be an antagonist capable of reversing many of the effects of the “normal” long version 3) Bronstein et al. (1990) showed rats made tolerant to morphine (3 days with subcutaneous pellets) have ratio of almost 1:2 (in favor of short version) “normal” (agonist) “short” acts as antagonist Opiate Withdrawal (5-10 days) A. Either of the following: (1) Cessation of (or reduction in) opiate use that has been heavy and prolonged (several weeks or longer) (2) Administration of an opioid antagonist after a period of opioid use (rapid vs slow abstinence) B. Three or more of the following, developing within minutes to days after Criterion A: (1) Dysphoric mood, depression (2) Nausea or vomiting (3) Muscle aches, cramps, tremors (4) Watery eyes or runny nose (5) Dilated pupils, goosebumps, or sweating (6) Diarrhea (7) Yawning (8) Fever (9) Insomnia C. Symptoms in Criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning. Protracted Abstinence Syndrome • Can last up to 6-7 months after withdrawal • Vague sense of feeling abnormal • Depression (increased propensity to sleep) • Abnormal response to stress • Abnormal respiration and temperature • Decreased self-esteem • Anxiety • Craving • Confounded by high comorbidity with other psychiatric disorders Additional Problems • Neonatal Effects: cross the placental barrier giving large doses to unborn fetus • Overdose: occurs when so much of the drug enters the brain the nervous system shuts down. Blood pressure drops, heart becomes to weak to pump blood, lungs labor & fill with fluid • Dirty & Shared Needles: Hepatitis B & C, HIV, flesh eating bacteria, gangrene, endocarditis, malaria, syphilis Polydrug Use • Mixing: Opioid users often mix cocaine or amphetamine, “speedball” - combine heroin & marijuana to give it more kick. Alcohol & benzodiazepines create synergistic effects increase potential for overdose, respiratory depression & death • Cycling: Addicts go on & off their drug of choice. Lowers tolerance & tissue dependence so the body can attempt to return to normal. Switch to alcohol, marijuana, barbiturates, benzodiazepines Treatment • Conventional Detox Centers – Buprenorphine, Subutex • Opioid partial agonist – Once abstinence begins, buprenorphine minimizes discomfort – When fully detoxed, buprenorphine is phased out. – Lasts 10-14 days. Treatment (cont) • Rapid Opiate Detox – Lasts 4-6 hours, released 24-48 hours after – Patient is anesthetized so that the patient does not experience withdrawal – Naltrexone • opioid blocker – Naloxone • counteracts effects of opioid Treatment (cont) • Detox is only the beginning – Continuing programs are needed to prevent relapse • Methadone-based programs exist… – But not as popular – Methadone is only a replacement • Cognitive therapy, 12-steps, meditation/hypnosis, etc