Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
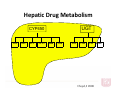
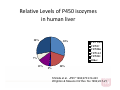
Pharmacokinetic Interactions: A Mechanistic Approach Part 1 Barry E. Gidal, PharmD Pharmacokinetic Interactions • Absorption – Adsorption – Intestinal Metabolism – Transporters • Distribution – Protein Binding – Transporters • Elimination – Renal Excretion – Hepatic Metabolism Human Drug Metabolism Cytochrome P450 Glucuronidation Conjugation Sulfation Gut & Liver Oxidation NADPH-dependent CYP450 reductase Absorption Absorption Interactions • Adsorption: – Bioavailability Absorption Interactions • Adsorption: – Bioavailability – Antacids can decrease the rate and/or extent of absorption – Need to separate out administration of antacid and drug by at least 2 hours. • atenolol ciprofloxacin enoxacin isoniazid ketoconazole norfloxacin ofloxacin tetracycline Absorption Interactions: Food effect • Large number of drugs whose absorption may be affected by food • Food can cause adsorption and/or delayed gastric emptying • Results – Increased and/or accelerated absorption – Decreased and/or delayed absorption » Singh et al. Clin Pharmacok 1999;37:213‐255 Absorption: Intestinal Metabolism • Highest concentration of enzymes is upper small intestine – duodenum and jejunum > ileum and colon • CYP3A4 – primary isozyme in GI – 10‐50% lower than in liver – Drugs with significantly intestinal metabolism • • • • Cyclosporine Midazolam Cisapride Tacrolimus Nifedipine Terfenadine Saquinavir Felodipine Simvastin Indinavir Nisoldipine Lovastatin Absorption: Intestinal Metabolism and Drug Interactions. • Inhibitors of CYP3A4 – Ketoconazole Itraconazole – Erythromycin Verapamil – Grapefruit Juice • Inducers of CYP3A4 – Phenytoin Carbamazepine Rifampin – St Johns Wort Transporters Proteins • Role of transport proteins in absorption, distribution and excretion • Control distribution of drugs across membranes • Extent of initial membrane permeability is affected by the physiochemical properties of the drug. • Transport proteins can play a key role in extrusion of drugs from organs and altering drug absorption, brain penetration, renal and hepatic elimination • Drug interactions affecting induction and inhibition of the transporters Transporters • • • • P‐glycoprotein (PgP) Multi‐drug resistance (MDR) Organic Anion Transporter (OAT) Organic Cation Transporter (OCT) » Ayrton and Morgan Xenobiotic 2001;31:469‐497 P‐Glycoprotein: History • Clinical oncologists first to recognize multi‐drug resistance – Cross resistance to other cytotoxic agents • First detected in early 1970’s in cultured cells selected for MDR • Subsequently cloned from mouse and human cells • Now one of the most extensively studied members of the ABC superfamily P‐Glycoprotein Physiological Significance of Pgp • Drug absorption, distribution, and elimination • Cytotoxic protection mechanism • Cell volume regulation by chloride transport • Steroid transport • Peptide transport P‐glycoprotein in Normal Tissues On the apical surface • • • • • • • • Intestine (jejunum, ileum, colon) Liver Blood brain barrier Kidney Testis Adrenal cortex Leukocytes and stem cells – NK cells, CD4+, CD8+, and bone marrow progenitor cells Placenta Absorption: Transporters • P‐glycoprotein (PgP) – Transmembrane Protein – Function as cellular efflux pumps • Results in absorption of drugs – Distributed throughout the body • Intestinal lumen, liver, kidney, blood brain barrier – Inducible – Close proximity to CYP3A4 with significant substrate overlap • can act synergistically to limit bioavailability of drugs CYP3A and P‐gps work together in the gut • Many substrates of P‐gps are also CYP3A4 substrates • In small intestine, P‐gps efflux compound to lumen, then compound is reabsorbed; this “shuttle” leads to increased “exposure” of compounds to CYP3A4 and maximizes their activity Intestinal Cells drug 3A4 pgp drug 3A4 pgp drug 3A4 pgp P-gps in “front”- with repeated shuttles of absorption/efflux Transporter Interactions • Interactions – Induction • Rifampin • St. John’s Wort • Garlic – Inhibition • • • • • • Verapamil Diltiazem Nifedipine Felodipine Clarithromycin Erythromycin Itraconazole Ketoconazole Cyclosporine Tacrolimus Quinidine Amiodarone Talinolol Tamoxifen Testosterone Distribution Pharmacokinetic Interactions Distribution ‐ • Distribution – Protein Binding interactions • Total blood concentrations no longer reflect unbound drug concentrations. • Only effects – a small number of highly protein bound drugs – that are monitored by total blood concentrations. Distribution: Transporter Interactions • P‐glycoprotein limits the penetration of a drugs across the blood brain barrier. • Administration of a PgP inhibitor has the potential to increase drug delivery to the brain Distribution: Transporter Interactions • Loperamide (PgP substrate) is a potent opiate that reduces GI motility; however it has no centrally mediate opiate effects (respiratory depression) alone. • Loperamide + quinidine (a PgP inhibitor) – resulted in respiratory depression – Not explained by increased loperamide plasma concentrations • Sadeque et al. CPT 2000;68:231‐7. Metabolism Cytochrome P‐450 • • A group of enzymes with are located on the endoplasmic reticulum. These enzymes are of particular importance when studying drug biotransformation and drug metabolism. • It is known that the gene for cytochrome P-450 has existed for more then 3.5 billion years. This indicates drug metabolism by the P-450 system is a new and secondary role for these enzyme systems. • The primary role for the P450 system seems to be one of metabolism and detoxification of endogenous compounds after they have been taken in by mouth. This accounts for the high concentrations of these enzymes located in the liver and small intestine. Hepatic Drug Metabolism CYP450 1A2 2E1 2C9 2C19 UGT 2D6 3A4 1A3 1A4 1A9 Cloyd, J 2000 2B7 A. di Masi et al. Molecular Aspects Medicine2009;30:297-343 Relative Levels of P450 isozymes in human liver 28% 30% 7% 13% CYP 3A4 CYP2C CYP2D6 CYP1A2 CYP2E1 Other 20% 2% Shimda et al. JPET 1994;270:414-423 Wrighton & Stevens Crit Rev Tox 1992;22:1-21 CYP’s: More Than Systemic Drug Clearance: Distribution of Brain CYP 450 Meyer RP, et al. Current Drug Metabolism 2007;8:297-306 End of Part 1