Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Embodied language processing wikipedia , lookup
Haemodynamic response wikipedia , lookup
Subventricular zone wikipedia , lookup
Executive functions wikipedia , lookup
Neuroeconomics wikipedia , lookup
Optogenetics wikipedia , lookup
Proprioception wikipedia , lookup
Perception of infrasound wikipedia , lookup
Neuroplasticity wikipedia , lookup
Metastability in the brain wikipedia , lookup
Environmental enrichment wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Synaptic gating wikipedia , lookup
Development of the nervous system wikipedia , lookup
Effects of sleep deprivation on cognitive performance wikipedia , lookup
Neuroanatomy wikipedia , lookup
Time perception wikipedia , lookup
Neuroscience in space wikipedia , lookup
Human brain wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Synaptogenesis wikipedia , lookup
Holonomic brain theory wikipedia , lookup
Aging brain wikipedia , lookup
Evoked potential wikipedia , lookup
Limbic system wikipedia , lookup
Microneurography wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Cerebral cortex wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
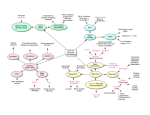
Physl important note • Function of glial cells: 1. Astrocytes • Functions 1. 2. 3. 4. 5. 6. 7. Physical support to neurons Help transfer nutrients to neurons Take up and degrade released neurotransmitter Enhance synapse formation & ↑ Synaptic transmission Maintain normal Brain ECF ion concentration Formation of blood – brain – barrier Repair of brain injuries & formation of neural scar tissue 2. Oligodendrocytes • Functions 1. Forms myelin sheath in the CNS. 3. Microglia • Functions 1. Phagocytosis [defense cells of CNS] 2. Release nerve growth factor 4. Ependymal Cells • Functions 1. Line internal cavities of brain and spinal cord 2. Formation of Cerebrospinal fluid [CSF]. 3. Work as Neural Stem Cell – to form new neurons and glial cells Basal Nuclei • Functions: – Co-ordination of movements – Muscle tone regulation – Posture maintenance Thalamus • All sensory information passes. • Crude awareness of sensation. Cerebellum Functions: – Balance of body. – Muscle tone. – Co-ordination and planning of skilled movements e.g. dance. lec2 SPINAL CORD • Function: – Conduit for Information passage To & fro Brain – Center for some reflexes REFLEXES • Examples a. b. c. Reflexes carry out the automatic actions of swallowing, sneezing, coughing, vomiting. Reflexes maintain balance and posture; e.g., spinal reflexes control trunk and limb muscles. Brain reflexes involve reflex center in brainstem; e.g., reflexes for eye movement. Polysynaptic reflex e.g. Withdrawal reflex, Abdominal reflex, Plantar reflex Stretch reflex: Sudden stretch to a muscle leads to contraction of that muscle is known as stretch reflex. Stretch Reflex is a basic spinal reflex. Example Knee jerk • The 5 components of Stretch Reflex – – – – – Sensory receptor – Muscle Spindle in skeletal muscle Afferent pathway – 1a fibers Center – spinal cord Efferent fibers – α-motor neuron Effector organ – skeletal muscle contraction Types of muscle fibers I. Extrafusal muscle fibers – Takes part in muscle contraction – Supplied by α - motor neuron II. Intrafusal muscle fibers – Also called as Muscle Spindle – Receptors for stretch reflex – supplied by γ - motor neuron Types of Nerve Fibers • Know only the major function Types of motor neuron • α - motor neuron – Supply Extrafusal fibers • γ - motor neuron – Supply Intrafusal fibers lec3 Sensory receptor • Every receptor is most sensitive to a particular modality of stimuli. That specific form of energy to which the receptor is most sensitive is called as its Adequate Stimulus. – e.g. rods & cones are stimulated by light not heat, sound etc • Know the type and the function only Difference Between • Receptor potential In the Receptor Graded Doesn’t obey all or none rule Can be summated Unpropagated • Action potential In the Sensory Nerve fiber Not Graded Obeys all or none rule Not summated Propagated Adaptation or Desensitization I. Phasic Receptors: Receptors Rapidly Adapting – E.g. pacinian corpuscles, Meissners corpusle. – For Touch, Pressure & Smell etc. II. Tonic Receptors: Slow Adapting receptors – E.g. Nociceptors, muscle spindles, Proprioceptors – For Pain, Body position etc. Receptor field • Receptor field of a sensory unit is the area from which a stimulus produces response in that unit. • Smaller the receptive field – More precise the information e.g. Finger tips • Larger the receptive field- less precise the information e.g. Back, arms, legs. Fiber type : A Number: II Origin: Muscle spindle - flower-spray ending, touch, pressure • Primary afferent sensations are – – – – fibers which carry cutaneous Large myelinated fiber Aα – proprioception Large myelinated fiber Aβ – touch, pressure. Small myelinated fiber Aδ – fast pain, Temp Small unmyelinated C fibers – slow pain, Temp Sensory pathway • • Dorsal Column Medial Lemniscal system • Also called as • Posterior column Tract or • Tracts of Goll & Burdach or • Fasciculus Gracilis and Cuneatus • Carries sensations of fine touch, position, vibration, two point discrimination & stereognosis. Anterolateral system • Consists of … 1. Anterior (Ventral) spinothalamic tract • carries crude touch and pressure, 2. Lateral spinothalamic tract • carries pain and temperature. Deferent between DORSAL COLUMN PATHWAY • Carries fine touch, position, pressure, vibration, two point discrimination, stereognosis • Afferent sensory fibers aβ type. • Very fast velocity 30 – 70 m/s • ANTEROLATERAL PATHWAY • Carries pain & temperature (lat. Sp.Th) • Crude touch & pressure (vent, sp. Th) • Afferent sensory fibers aδ • 6 – 30 m/s (myelinated) fast pain • C fibers – 0.5 – 2 m/s (unmyelinated) slow pain Temperature • Afferent from cold receptors – Aδ & C fibers. • Afferent from warm receptors – C fibers. • Temperature sensation is carried via lateral spinothalamic tract. • Aδ (myelinated) : for fast pain”sharp loclized” • C fibers (unmyelinated): slow pain “ dull, diffuse” Both Aδ & C fibers terminate in dorsal horn. lec4 Brain Analgesic System • Brain has built in analgesic system. • By sending message through descending analgesic pathway to the inhibitory neuron in the Dorsal horn cell of spinal cord. • Brain descending pathways release Enkephalin which bind with opiate receptors at afferent pain fiber terminals in Dorsal horn of spinal cord and work like Morphine (powerful analgesic). • Endorphin, Enkephalin and Dynorphin are endogenous or natural analgesic system. They suppress release of substance P. Somatosensory cortex (S1 area) • It is located in post central gyrus of the cerebral cortex. • There is detailed localization of the fibers from various parts of the body. • Somatosensory cortex is a site of perception of – Somasthetic sensation [touch, pain, temperature, pressure] – Proprioception • The arrangement of thalamic fibers in S1 is such that parts of body are represented in order, along the post central gyrus with the feet on the top & head at the lower end of the gyrus. Somatosensory cortex (S1 area) • Here different body parts are not represented equally • Size of cortical receiving area for impulses from a particular part of the body is proportionate to the No. of receptors. • Thus very large area is occupied by impulses coming from lips, face, and hand (thumb) also parts of mouth concerned with speech. • Trunk & back has small area of presentation in sensory cortex. • Each side of the cortex receives information from opposite side of the body. • From here many of signals spread directly to motor cortex, play a major role in controlling motor signals that activate muscle contraction Somatosensory area II • SII is located in the superior wall of the sylvian fissure, the fissure that separate the temporal lobe from the frontal & the prietal lobe. • Face is presented anteriorly, arms centrally & legs posteriorly. • The presentation of the body parts on sylvian fissure is not as complete & detailed as in post central gyrus. • Little is known about role of somatosensory area II (SII). • Signals enter into SII from brain stem, also SI area and other areas of brain visual & auditory. • Projection from SI are required for function of SII. Somatosensory Association Area • • Located in parietal lobe behind area SI. It receives signals from ; 1. 2. 3. 4. • Somatosensory area I Thalamus Visual cortex Auditory cortex Effect of removing … – Person looses the ability to recognize objects felt on the opposite side of the body, he looses the sense of form of his own body on the opposite side also. He forget it is there. – This complex sensory deficit is called Amorphosynthesis. lec5 CORTICOSPINAL TRACTS: • It is the most important motor pathway from motor cortex • Origin: – 30% from Primary Motor Cortex – 30% from Premotor and Supplementary Motor Area – 40 % from Somatosensory Area • Course: – passes through posterior limb of internal capsule and downwards through brainstem. – Majority of fibers (80%) than cross in lower medulla to the opposite side and descend as lateral Corticospinal tracts. – 20% uncrossed continue as Anterior Corticospinal Tract. Eventually most of them also cross before termination in Spinal Cord CORTICOSPINAL TRACTS: • Termination: – Terminate principally on the Interneurons, in the intermediate region of cord grey matter , – A few terminate on sensory relay neurons in dorsal horn and – A few terminate directly on Anterior Motor Neuron. – direct innervation of alpha motor neurons by pyramidal tract axons is mainly to distal muscles and is associated with the ability to execute fine, precise movements lec6 RUBROSPINAL TRACT • Functions - Involved in movements of distal limbs (hand & feet) also regulates tone and posture. • It is excitatory to flexors and inhibitory to extensor muscles. VESTIBULOSPINAL TRACT • Function - Excitatory to ipsilateral extensor. Inhibitory to flexor muscles • Regulates muscle tone for maintaining balance in response to head movement Difference between Pyramidal and Extrapyramidal Tract PYRAMIDAL TRACTS 4. 80 % of Corticospinal tracts (lateral) cross in medulla 20 % of corticospinal tract (ventral) cross in spinal cord Because of crossing cerebral cortex controls opposite side of the body 5. Function: - Lat. Corticospinal tract – fine movement of fingers eg. Writing, needle work - Ventral corticospinal tract – Axial or Postural Movement EXTRA PYRAMIDAL TRACTS Major extra pyramidal tracts, some cross and others are uncrossed Function: Control of body posture involving involuntary movements of axial and Proximal limb muscle lec7 BASAL NUCLEI - FUNCTIONS • Modulation of motor activities through neuronal circuits. • Maintain purposeful motor activity while • suppressing unwanted or useless movement. • Change the Timing and Scale the Intensity of Movements • Basal ganglia function in association with the corticospinal system to determine & control complex patterns of motor activity. BASAL NUCLEI - FUNCTIONS • Regulate muscle tone - Inhibit muscle tone throughout the body • Monitor and coordinate slow, sustained contractions related to posture and support. • Prevent abnormal involuntary movements. • Control group of movements for emotional expression. • Role in procedural learning, routine behaviors or "habits" such as bruxism. • Role in Memory, emotion, Reward Learning and other cognitive functions. BASAL NUCLEI - CONNECTIONS • Main input: Comes from the cerebral cortex (motor area) and projects to the Striatum (Caudate nucleus & Putamen) • Main output: Is from Globus Pallidus via the thalamus to the cerebral cortex (motor area) GLU GABA GABA GLU GLU GABA GABA GLU GLU GABA GLU GLU Parkinson’s Disease • Clinical symptoms • Rigidity – Cogwheel, Lead Pipe • Tremor (Resting) – Pill rolling type • Hypokinesia/Akinesia - poverty and slowness in initiating and carrying out different motor movement. • Face – expressionless, Mask like face • Blinking of eyelid is reduced • Writing becomes small – micrographic and spidery • Changes in posture – Stoop is characteristic • Gait – becomes hurrying, festinant, short and shuffling with poor arm swinging lec8 CEREBELLAR FUNCTIONS 1) Maintenance of balance 2) Enhancement of muscle tone 3) Coordination and planning of skilled voluntary muscle activity 4) Sequences the motor activities 5) Monitors and makes corrective adjustments in the activities initiated by other parts of the brain 6) Compares the actual motor movements with the intended movements and makes corrective changes. 7) The cerebellum does not initiate movement, but it contributes to coordination, precision, and accurate timing. 8) Functional imaging studies have shown cerebellar activation in relation to language, attention, and other cognitive functions. 9) Correlation studies have shown interactions between the cerebellum and non-motor areas of the cerebral cortex; and a variety of non-motor symptoms have been recognized in people with damage that appears to be confined to the cerebellum 10) functional MRI suggest that more than half of the cerebellar cortex is interconnected with association zones of the cerebral cortex. Functional Organization of the Cerebellum Functionally cerebellum can be divided into . . . • The Floculonodular lobe – Vestibulocerebellum – participates mainly in balance and spatial orientation • Intermediate zone - Spinocerebellum – Enhances muscle tone and coordinates skilled voluntary movements • Lateral zone - Cerebrocerebellum – controls sequencing movements of the muscle. Important for timing and coordination of movement. – Plays role in planning and initiating voluntary activity – Stores procedural memories Neuronal Organization of the Cerebellar Cortex Cerebellar Cortex is organized in three layers I. Granular layer – It is thick inner most layer and contains Granule cells, Golgi type II cells and other interneurons II. Purkinje cell layer – – – It is middle layer Contains Purkinje cells Output is always Inhibitory III. Molecular layer – – It is outermost layer Contains stellate and basket cells, dendrites of Purkinje and Golgi type II cells and parallel fibers (axons of granule cells) Circuit of the Cerebellum Output of the Cerebellar cortex • Purkinje cells are the only output of the cerebellar cortex which goes to Deep cerebellar Nuclei • Output of the Purkinje cells is always inhibitory. the neurotransmitter is γ- aminobutyrie acid (GABA) • Output of the cerebellum regulates rate, range and direction of movement. Input to the Cerebellar cortex • From Mossy fibers originating from brain stem and spinal cord and • From Climbing fibers originating from Inferior Olivary Nucleus in Medulla Lec 9 Functions of Brainstem • The nerve connections of the motor and sensory systems between the main part of the brain to the rest of the body pass through the brainstem. • Has role in Regulation of muscle reflexes involved with equilibrium and posture • Control of many stereotyped movements of the body such as suckling, yawn and stretch, cry and laugh etc. • Control of eye movements Function of brainstem • Origin of majority (10) of cranial nerves is in Brainstem • Cranial nerves arising from brain stem – Mid-brain – III, IV – Pons – V, VI, VII, VIII – Medulla – IX, X, XI, XII • The brainstem provides the main motor and sensory innervation to the face and neck via the cranial nerves. • Note only Cranial nerves I (Olfactory) & II (Optic) do not have any origin from Brainstem Function of brainstem • It also regulates the central nervous system, and is Important in . . . – Arousal and Activation of cortex, – Maintaining Consciousness and – Regulating the Sleep cycle. • Centers for Cardiovascular, Respiratory, and Digestive control are located in Brainstem • Thus basic functions controlled from Brainstem Include … – – – – – Heart Rate & Blood Pressure, Breathing including Cough & Sneezing Sleep, wakefulness, Consciousness Digestive activities including swallowing, vomiting Posture & Equilibrium Lec 10 PINEAL GLAND • Pineal gland secret melatonin that have rule in timing • central role in control of diurnal rhythms while In Humans, the pineal and melatonin do play a limited role. • Recent investigations have demonstrated a role for melatonin in sleep, tumor reduction and aging. • And damage to it cause precocious puberty THALAMUS • In general, there are three basic types of thalamic nuclei: – Relay nuclei – Association nuclei – Nonspecific nuclei. • Relay nuclei receive very well defined inputs and project this signal to functionally distinct areas of the cerebral cortex. • The association nuclei receive most of their input from the cerebral cortex and project back to the cerebral cortex in the association areas where they appear to regulate activity. • The nonspecific nuclei include many of the intralaminar and midline thalamic nuclei that project quite broadly through the cerebral cortex, may be involved in general functions such as alerting. • damage in thalamus cause coma THALAMUS – Clinical Significance • Cerebrovascular accident (stroke) can lead to the Thalamic Syndrome which involves a one-sided burning or aching sensation often accompanied by mood swings. • Damage to the thalamus can result in coma. • Fatal Familial Insomnia is a hereditary prion disease in which degeneration of the thalamus occurs, causing the patient to gradually lose his ability to sleep and progressing to a state of total insomnia, which invariably leads to death. • Korsakoff's Syndrome occurs from damage to the medial thalamus & mammillary body due to Thiamine deficiency. Hypothalamus • Have set point < diced what is the normal temperature any change in it will change the firing > autonomic nerve system < expose to all everything • Biological clock • Hyperpaxia < set point not change • Fever < set point change FUNCTIONS OF HYPOTHALAMUS Biological Functions 1. Controls body temperature 2. Controls thirst and urine output 3. Controls food intake Hunger and Satiety center 4. Participates in the sleep – wake cycle. 5. Contains the “biological clock” that regulates certain body functions that vary with time. FUNCTIONS OF HYPOTHALAMUS Endocrine Functions 1. Controls anterior pituitary hormone secretion 2. Produces posterior pituitary hormones ADH and oxytocin 3. Controls uterine contraction and milk ejection Autonomic Nervous System Function 1. Serves as major ANS coordinating center FUNCTIONS OF HYPOTHALAMUS Emotion & Behavior 1. Plays role in emotional responses and behavioral pattern including rage, fear pleasure etc. 2. Reward & Punishment center 3. Role in sexual behavior and reproduction Lec 11 Limbic system • Limbic system is motivation • Emotion > external or internal for benefit or harmful Amygdala • Perform a primary role in the processing of memory, decision-making, and emotional reactions. • There are functional differences between the right and left amygdala and also between Male and Female Amygdala. • primary role in the formation and storage of memories associated with emotional events. E.g. Fear Conditioning. • Also involved in memory consolidation - Formation of Long Term Memory. • The amygdala plays a pivotal role in triggering a state of fear. • Amygdala is associated with Anxiety and panic attacks. • Studies link amygdalae to the emotional reactions of PTSD patients. • Social behavior • Stimulating the amygdala appears to increase both sexual and aggressive behavior. Hippocampus • Has important role in formation of new memory about experienced events (Episodic Memory). • Bilateral hippocampal damage results mainly in Anterograde amnesia and often also retrograde amnesia • Believed to have role in spatial memory and navigation. Behavior and its Control • Reward and punishment caused by the Limbic system are important for behavior. • Several limbic structures are concerned with sensory experience – is it pleasant or unpleasant? • Reward center located in • the lateral and ventromedial hypothalamus, • thalamus certain areas, • Amygdala • Punishment center located in • • • • Hypothalamus Thalamus Amygdala and Hippocampus Neurotransmitters associated with limbic system • Norepinephrine • Dopamine • Serotonin • Many drugs increase dopamine in pleasure pathways in limbic system, therefore, cause intense sensation of pleasure e.g. cocaine blocks re-uptake of dopamine at synapses • Amphetamine, used in depression, causes increased release of dopamine from dopamine secreting neurons Lec 12 SPEECH Speech Centers: – Broca’s area • motor speech area – Wernicke’s area • sensory speech area. Analyzing hear or written word • Understanding happen here and right response diced here. • Both connected by Arcuate Fasciculus. • • Both areas also interact with association areas. Association area remember the sequence of muscle contraction to pronounce the word Broca’s area • It is located in left frontal lobe just front of the base of the Primary motor cortex. • It is for Articulation – Word formation • Broca’s area contains motor memories — in particular, memories of the sequences of muscular movements that are needed to articulate words. • Broca's area excites Motor area which controls the muscles necessary for articulation. Wernicke’s area • It is located in the left cortex at Superior gyrus of Temporal lobe at the juncture of parietal, temporal and occipital lobes. • It is concerned with language comprehension (understanding). • It plays important role in understanding of both spoken and written messages. • Wernicke’s area receives input from visual cortex in the occipital lobe and also auditory cortex in temporal lobe. Not much important but remember is association area Arcuate Fasciculus • Is a axon pathway between Wernicke’s area and Broca’s area • Higher-Order Association Cortex • Wernicke’s area has connections with various association areas in … • Left Frontal • Left Temporal • Left Parietal • Are involved with mediating between concepts and language Lateralization: • Speech area are located in one sphere (on one side), usually the dominant hemisphere. • Left hemisphere is therefore called DOMINANT SPHERE. • 90% of left handed people have left cerebral hemisphere as dominant also. • Right hemisphere for expression and narrative selection. SPEECH DISORDERS • Thus Damage to the specific regions of brain can result in selective disturbance of speech. Damage to Brocas’s area Damage to Wernicke’s area Damage to ARCUATE FACICULUS Speech Disorders of Articulation (motor aphasia) (sensory aphasia) (Conduction aphasia) (Dysarthria) SPEECH DISORDERS • It results in failure of word formation, but patient can understand the spoken and written words. • Broca’s aphasia is much more than a deficit in pronouncing words. In general, three major speech deficits are produced by lesions in and around Broca’s area: agrammatism, anomia, and articulation difficulties. SPEECH DISORDERS Damage to Wernicke’s area: (sensory aphasia) • These patients can not understand the words they hear or see. • what they say is full of jargon and neologisms that make little sense. SPEECH DISORDERS Anomic aphasia (anomia): • is a type of aphasia characterized by problems recalling words, names, and numbers. Conduction Aphasia: • Patients may be able to understand speech as well as produce meaningful speech, but have difficulty repeating a spoken sentence. SPEECH DISORDERS Dyarthria in parkinson Lec 13 MEMORY • Memory trace > change in the synapse in the particle memory • Memories are stored in the brain at synapses by changing the basic sensitivity of synaptic transmission between neurons. • The neural change at synapses which is responsible for retention or storage of knowledge is known as memory trace. • Once memory trace are established, they can be activated by thinking mind to reproduce memory. • Memory traces occur at many regions of brain at cortical and subcortical regions. • Important areas associated with memory are: • • • • • • • cerebral cortex (motor, sensory, visual & auditory) prefrontal cortex hippocampus & medial temporal lobe Amygdala limbic system thalamus Cerebellum+ basal ganglion > skill and movment MEMORY - STAGES MEMORY - TYPES • Declarative (Explicit) memory: • Memory of experiences factual knowledge & personal • Semantic Memory: • Impersonal facts and everyday knowledge • Episodic Memory: • Personal experiences linked with specific times and places • Procedural (Implicit) Memory: • Long-term memories of conditioned responses and learned skills, e.g., driving MEMORY – IMP. REGIONS IN BRAIN Major regions in brain which play role in a particular type of memory include: • Short Term Memory – – Hippocampus, Medial Temporal Lobe • Long Term Memory – – Neocortex • Declarative Or Explicit Memory – – Hippocampus • Skill Or Implicit Memory – – Cerebellum, Basal Ganglia. • Working Memory – – Prefrontal Cortex Note took in lec • Senile dementia > with old age • Dementia > memory lose with some intelligence and personality • Learning > repeat the circle < that will make the synapse strong • Reticular > that keep you awake be stimulation neural circle and aware of self, thought and associated with emotion • Consdilation memory > formation memory for long time lec14 Electroencephalogram - EEG • Based on frequency and amplitude waves of EEG can be: – Beta: >14 Hz, activated cortex – Alpha: 8-13 Hz, quiet, waking state (eyes close) – Theta: 4-7 Hz, some sleep states – Delta: < 4 Hz, deep sleep – Gamma: 30-70 • Deep Sleep – High synchrony, high EEG amplitude EEG Alpha Waves: • rhythmic, 8-13 Hz • most common in adults. • Most marked in the parieto-occipital area. • Occur with closed eyes , relaxation, wondering mind. • Alpha block when you open your eye Also called Desynchronization EEG Beta Waves: • mostly on temporal and frontal lobe • Recorded during mental activity, awake person (eyes open). EEG Theta Waves: • Stage II and Stage III sleep. • Theta and delta waves are known collectively as slow waves. Delta waves: • Children • In adult abnormal • In deep sleep EEG • Montage: pattern of 10/20% system of EEG electrode placement Sleep • Sleep is a readily reversible state of reduced awareness and responsiveness of a person to environment. • Sleep is an active process, not just the absence of wakefulness. • Coma is a state of unconsciousness from which a subject cannot be aroused • It consist of two alternating periods of. – Non-Rapid Eye Movement (NREM) sleep – Rapid Eye Movement (REM) sleep • Petimal : spike and dom pattern Sleep stages • Classified on the basis of EEG Features 1. NREM Sleep : Slow Wave Sleep – It Is divided into 4 stages : – Stage 1 NREM • when a person is initially falling asleep . • Characterized by low-amplitude, fast activity (α-waves). – Stage 2 NREM • Marked by appearance of Sleep Spindles. • These are bursts of alpha-like 10-14 z , 50 uV waves . – Stage 3 NREM • Lower frequency (mainly theta) ,higher amplitude EEG waves. – Stage 4 NREM • Still slower frequency (mainly delta) & higher amplitude waves . 2. REM Sleep : Paradoxical Sleep – Low-voltage , fast activity (β-waves) Sleep sages Non-REM Sleep (NREM): Slow-wave sleep • 75% of sleep time. • Further divided into four stages • this is the deep, restful sleep . • Decrease in vascular tone. • Decrease in BP (10-30%) • Decrease in Resp. rate. • Decrease in BMR • Not associated with rapid eye movement. • EEG: Theta + delta waves. • Dreams may occur but are not remembered as they are not consolidated in memory. Sleep stages Stage N1: Stage 1 NREM Sleep • It refers to the transition of the brain from alpha waves (of Awake state) having a frequency of 8–13 Hz to theta waves having a frequency of 4–7 Hz. • This stage is sometimes referred to as somnolence or drowsy sleep. • During N1, the subject loses some muscle tone and most conscious awareness of the external environment • Sudden twitches and jerks, also known as positive myoclonus, may be associated with the onset of sleep during N1 Sleep stages Stage N2: Stage 2 NREM Sleep • Stage N2 is characterized by sleep spindles ranging from 11–16 Hz and K-complexes. • During this stage, muscular activity as measured by EMG decreases, and conscious awareness of the external environment disappears. • This stage occupies 45–55% of total sleep in adults. Sleep disorder **defention I. Dyssomnias: – Sleep disorders that are characterized by disturbances in the amount, quality or timing of sleep. – E.g.: • • • • Insomnia Hypersomnia Sleep apnea Narcolepsy II. Parasomnias: – Dysfunctions or episodic events occurring with sleep. – E.g.: • • • • Sleep-walking (somnambulism) Sleep-related enuresis (bedwetting) Sleep-talking (somniloquy) Sleep-terrors and nightmares Sleep Disorders lec15 The eye The Fibrous Tunic – Sclera/Cornea: • Most External Layer of Eyeball • White, opaque, tough, fibrous tissue covering majority of the eyeball posteriorly is Sclera. • The thin transparent anterior continuation is eye Internal Chambers and Fluids: The lens & Suspensory Ligaments divide the eye I. Anterior segment – Further divided into • Anterior chamber – between the cornea and iris • Posterior chamber – between the iris and lens – Filled with aqueous humor II. Posterior segment – Filled with vitreous humor *lens can change due to muscle OPTICS OF VISION • Accommodation: – It is the ability to adjust the refractory strength of lens (curvature of the lens) to focus nearby objects on retina OPTICS OF VISION • Astigmatism – Uneven curvature of Cornea • Cataract – Decreased transparency of Lens • Myopia – Better near vision than far vision – Due to either the eyeball is too long or lens too strong – Corrected by Concave lens • Hyperopia – Better far vision than near vision – Due to either the eyeball is too short or lens too weak – Corrected by Convex lens RETINA-FUNDOSCOPY • Major function of eye is to focus light on Rods & Cones of retina. • Macula lutea – contains mostly cones • Fovea centralis – contains only cones – Region of highest visual acuity • Optic disc – blind spot • Retina receives blood from two sources – Outer third of the retina – supplied by capillaries in the choroid – Inner two-thirds of the retina – supplied by central artery and vein of the retina – Outer most : photo reseptor – Inner most: nerve and red and cons, nuclular RETINAL LAYERS RETINA Major types of neurons/cells in retina: I. Photoreceptors – Rods & Cones II. Bipolar Cells Connect Photoreceptor cells with Ganglion cells III. Horizontal cells Interconnect Photoreceptor cells IV. Amacrine cells Interconnect Ganglion cells & also to Bipolar cells V. Ganglion cells Are only output of retina, axons form optic nerve. PHOTORECEPTORS • Photopigment in Rods is called as Rhodopsin • And cons called photospin PHOTOTRANSDUCTION • It is the process of converting light stimuli into electrical signals. • Rods and Cones on stimulation by light respond by Hyperpolarization. • Steps: – The only light dependent step in entire process of phototransduction is conversion of 11-cis retinal to all-trans retinal on light exposure This causes opsin activation activates transducin activates Phosphodiesterase decreases cGMP which were keeping the Na leak channels open in outer segments of Rods Na channels close and hyperpolarization occurs decrease in secretion of Glutamate by rods at synapse with bipolar cells. – Further processing occur in subsequent layers of Retina PROCESSING IN RETINA • Axons of Ganglion cells form the optic nerve which transmit information to brain as Action Potentials. VISUAL PATHWAY • Axons of ganglion cells exit eye as the optic nerve • Fibers from the Nasal halves of Retina cross to opposte side in the Optic Chiasma while the fibers from the temporal side of retina do not cross. • Thus together Nasal side fibers of opposite side and Temporal side fibers of same side continue as Optic Tract • Optic tracts terminates in Lateral geniculate nucleus (LGB) of the thalamus. • From the LGB Fibers of the optic radiation reach the primary visual cortex Note took in lec • • • • • • • Analysis start at retina sclera and cornea : visible Choroid: cillary body and iris all called uvea Choroid: blood vessels Cillary: cillary muscle Retina : 10 layers , there’s ant and post champers Presbyopia : decrease in accommodation in old age lec16 VISUAL PATHWAY Branches at Subcortical level: • Branch to midbrain • Superior colliculi • Pretectal nuclei • Branch to SCN (suprachiasmatic nucleus) VISUAL PATHWAY LESIONS A. Unilateral Blindness B. Bitemporal Hemianopia C. Homonymous Hemianopia D. Homonymous Hemianopia with Macular Sparing LATERAL GENICULATE BODY • The magnocellular pathway, from layers 1 and 2, carries signals for detection of movement, depth, and flicker. • The parvocellular pathway, from layers 3–6, carries signals for color vision, texture, shape, and fine detail. VISUAL CORTEX • Columns for Color are called BLOBS. • Every type of visual info is processed simultaneously by the vertical and horizontal cortical systems. COLOR VISION Examples of Color Perception: • %Cone Stimulation: R G B Blue 0 0 100 yellow 83 83 0 • The extent to which each of the cone types is excited is coded and transmitted in separate parallel pathways to the brain. • These pathways project to the ‘color’ blobs and the deep portion of layer 4C of V1 cortex. • Distinct color vision center in the visual cortex combines and processes these inputs to generate the perception of color. • ^^ not important COLOR BLINDNESS Ishehara Chart lec17 sound • Sound that is perceptible by humans has frequencies from about 20 Hz to 20,000 Hz. • Impedance : resistance • Impedance: matching intensity of sounds • Amplitude: 10 micro sec Sound Transmission External Ear: • Air transmitted sound waves are directed toward the Tympanic Membrane • Functions of External Air: – Sound collection – Increasing pressure on the tympanic membrane in a frequency sensitive way. – Sound localization • Function of middle ear: • Trans sound from external to internal – Maintains resting air pressure on both sides of TM equal – Transfers movements of the tympanic membrane to the inner ear – Impedance matching – Attenuation • Protect ear from large sounds Attenuation Reflex • Function: – To protect the cochlea from damaging vibrations caused by excessive sound – To mask background noise in loud environments. Sound Transmission Inner Ear: • Motion along the basilar membrane excites frequency specific areas of the Organ of Corti, which in turn stimulates a series of nerve endings. • Basilar membrane have apex and base • Apex: low frequency, Base: high frequency • Organ of hearing is corti body • Receptor of hearing : hair cell • Hair cell is 2 A-inner: actual receptor of hearing • B-outer: increase or decrease sensitivity of hearing Place Principle • The method used by nervous system to detect different sound frequencies is to determine the position along the basilar membrane that are most stimulated. This is called the “place principle Different between them • Fluid in perlymph : no cell • Endolymph : rich in K+ • Specialty of basilar membrane ? • For frequency Function of Inner & Outer Hair cells • Inner Hair Cells: • They transform the mechanical forces of sound into electrical impulses. • Outer Hair cell: • Increases the sensitivity of inner hair cells for different frequency and intensity. • Hair cell generate action potinal > transmit it by cerebral ganglion > then to superior olivary from opposite side > to inferior coccli in medbrain > MGN > auditory cortex in temporal • Tonotopic map : different frequency Sound Ananlysis Perceiving Pitch (Frequency): • location of vibration on the basilar membrane Appreciation Of Loudness Of Sound: by ampitude If increase in action potinal increase in loudness • Intensity or loudness of sound correlates with two factors: 1. Rate of discharge from the individual fibers of auditory nerve 2. Total number of nerve fibers discharging. Pathophysiology of hearing • Conduction deafness – – • That caused by impairment of the physical structures of the ear that conduct sound to cochlea like outer ear and middle ear. Ex: wax, osteosclrosis Sensorineural deafness – – – It is the deafness caused from impairment of the Hair cells, auditory nerve etc. Ex: presbyacusis < old age “ damage in higher frequency fiber” Meneres disease lec17 Taste (Gustation) • Taste receptors have life span of about 10 days Anatomy of Taste Buds. • 10,000 taste buds found on tongue, soft palate & pharynx • Taste buds consist of: – ~50 receptor cells – Basal cells cells (type 3) (type 1 &2) surrounded by supporting cells develop into supporting cells then receptor • Gustatory hairs project through the taste pore • Life span of 10 days Taste – Salty • Stimulated by chemical salts, especially NaCl – Sour • Caused by acids which contain a free hydrogen ion, H+ Sensation of Taste Discrimination of intensity of taste: Discrimination in intensity of taste: – Poor (like smell) – Requires 30% change to allow discrimination of intensity Clinical considerations • • • • Ageusia: Absence of sense of taste Dysgeusia: Disturbed sense of taste Hypogeusia: Diminshed sense of taste Hypergeusia: increased sense of taste lec19 Smell (Olfaction) Olfactory mucosa contains 3 cell types • Olfactory receptor cell • Supporting cells – Secrete mucus • Basal cells – Precursors of new olfactory receptor cells (replaced about every two months) Physiology of Olfaction only important in red • Odorant binds to the receptor of an olfactory hair→ G-protein activation→ activation of adenylate cyclase→ production of cAMP→ opening of Na+ channels→ inflow of Na+ →generator potential→ nerve impulse through olfactory nerves→ olfactory bulbs→ olfactory tract→ primary olfactory area of the cerebral cortex. Olfactory pathway • Fibers originating in olfactory bulb travel in two different routes – Subcortical route, to limbic system – close coordination between smell and behavioral reactions, associated with eating , etc. – Route to primary olfactory cortex (piriform cortex) Abnormalities Anosmia (absence of sense of smell), Hyposmia (diminished olfactory sensitivity) dysosmia (distorted sense of smell) Several dozens different anosmias have been detected in humans. They are presumably due to absence or disrupted functions of one of the many members of odorant receptor family