Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Central pattern generator wikipedia , lookup
Synaptogenesis wikipedia , lookup
Emotional lateralization wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Executive functions wikipedia , lookup
Neurocomputational speech processing wikipedia , lookup
Affective neuroscience wikipedia , lookup
Neuroplasticity wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Human brain wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Time perception wikipedia , lookup
Aging brain wikipedia , lookup
Cortical cooling wikipedia , lookup
Neuroeconomics wikipedia , lookup
Environmental enrichment wikipedia , lookup
Synaptic gating wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Orbitofrontal cortex wikipedia , lookup
Microneurography wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Evoked potential wikipedia , lookup
Muscle memory wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Embodied language processing wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
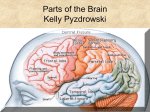
Chapter 14: Motor System Chris Rorden University of South Carolina Norman J. Arnold School of Public Health Department of Communication Sciences and Disorders University of South Carolina 1 Cortical Level Prefrontal Cortex Responsible for manipulating discrete and skilled voluntary movements through planning and innervation of muscles Refers to highly conscious planning and sequencing Site of reasoning, thinking, planning Primary Sensory (parietal) Primary Motor (frontal) Premotor (frontal) 2 Sensorimotor Cortex Areas (1) Premotor Cortex 30% of Motor Fibers Info from thalamus, cerebellum, basal ganglia Has some skilled patterns which are well learned Lesion(s) in the inferior premotor cortex in the left hemisphere is often associated with verbal apraxia 3 Sensorimotor Cortex Areas (2) Primary Motor Cortex 30% of motor fibers 2% from Betz Cells which are large to support long axons Corticospinal tract – (superior 2/3) Voluntary Movements of muscles controlled via spinal nerves. Corticobulbar tract – (inferior 1/3) Facial and Associated Muscles – project to cranial nerve nuclei. 4 Sensorimotor Cortex Areas (2) Primary Sensory Cortex 40% of motor fibers – Project through motor cortex with modulation of sensory information – Corticopontine tract (pons) 5 Physiology of Motor Cortex Highly Organized in Form of Homunculus Discovered by Penfield and Roberts who used electrical stimulation of cortex on patients in surgery 6 Cranial Nerves Spinal Nerves Corticospinal Tract – From upper two thirds of primary motor cortex, premotor cortex and sensory cortex – Through Corona Radiata to Internal Capsule and Pes Pedunculi in the Midbrain Corticobulbar Tract – From lower third of motor cortex and adjacent area to corona radiata through internal capsule, pes pedunculi across midline to lower cranial nuclei – Crossed: oculomotor, abducens, trigeminal, facial, vagus, glossopharyngeal and hypoglossal – Uncrossed: trochlear – Some duplication of tracts offers redundancy 7 Pyramidal Tract Fibers Corona Radiata (fibers tracts between IC and cortex) Internal Internal 4 3 Capsule, Capsule, Anterior 86 Posterior Limb Limb 2 Pyramid Lateral Corticospinal Tract 8 Path of upper motor neurons Lateral: Skeletal Muscle Fingers, Toes, Forearm Anterior: Axial and Girdle muscles 9 Clinical Considerations Lesions in corticospinal fibers result in spastic hemiplegia Lesions in corticobulbar fibers result in paralysis of facial, lingual, palatal and laryngeal muscles. More bilateral innervation causes less paralysis 10 Clinical Considerations Upper Motor Neuron symptoms – Flaccid followed by spastic hemiplegia – Increased Muscle Tone – + Babinski Sign – Hyperreflexias – Loss of Abdominal Reflexes – Alternating Hemiplegia (Some Fibers that are crossed and uncrossed) Normal reflex Negative Babinski Abnormal Positive Babinski 11 Clinical Considerations Lower motor neuron symptoms – Damage to LMN eliminates the function of the motor unit – Lesion affecting the LMN causes weakness of muscles and reduces tendon reflexes – Muscle tone is flaccid – Can be seen in muscular dystrophy and myasthenia gravis – Absent or greatly reduced Babinski 12