Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
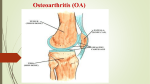
Osteoarthritis Objectives Describe prevalence, etiology & pathogenesis of ( O.A. ) . Take proper history, considering Pt.'s ICE. List the risk factors for developing O.A. Conduct knee examination . Describe the radiological findings . Identify different modalities of management for O.A. Recommend lifestyle changes & educational strategies as part of treatment . Case Scenario - Saied, healthy & active 54 years old carpenter. - C/O: Bilateral knee pain . He used Acetaminophen & local diclofenac gel. He had partial relief . - He is unable to do his job comfortably .He does his prayers sitting on a chair. - PMH: GERD & hernia repair 10 years ago. - O/E: BP = 130/85 mmHg , Temp. 36.5 °C. - Weight = 98 Kg, Height = 175 cm - Knees Examination: - X-Rays of both knees: Definition OA refers to a clinical syndrome of joint pain accompanied by varying degrees of functional limitation and reduced quality of life. OA is a common degenerative disorder of the articular cartilage associated with hypertrophic bone changes. It is characterised pathologically by localised loss of cartilage, remodelling of adjacent bone and associated inflammation. It is the most common form of arthritis, and one of the leading causes of pain and disability worldwide. The most commonly affected peripheral joints are the knees, hips and small hand joints. The pathogenesis of joint damage Articular cartilage. molecular level gradual proteolytic degradation of the matrix increased synthesis of the matrix components by the chondrocytes morphological changes cartilage surface fibrillation cleft formation loss of cartilage volume The pathogenesis of joint damage Bone :less well understood, development of osteophytes at the joint margin ossification of cartilage outgrowths major changes in the vascularity and turnover of the subchondral bone. Cytokines and other signalling molecules released from the cartilage, synovium, and bone affect chondrocyte function. Role for inflammation in O.A. , at least in some patients and in some phases of the disease. Differential diagnosis Condition Differentiating Differentiating signs/symptoms Investigations Gout More acute onset(few Hours), the affected joint is usually red, hot, and acutely tender. Commonly involves the (MTP) joint Joint fluid analysis shows leukocytes >2000, and the presence of sodium monourate crystals. RA symmetrical small joint in the hands, the MCP joints and sparing the DIP joints. More prolong morning stiffness than OA. Patients feel generally unwell, with fatigue and low mood. In RA, ESR and CRP are abnormal and RF is positive. Typical RA erosive changes are seen on x-ray, MRI, or ultrasound. Condition Psoriatic Arthritis Avascular Necrosis Differentiating signs/symptoms Differentiating Investigations often affects the DIP joints. In psoriatic arthritis, the joint involvement is usually asymmetrical x-ray shows typical erosive changes. This is common in the hip and knee joints. The onset is subacute and there is usually a risk factor such as corticosteroid use. MRI is the most sensitive test in AVN. In the early stages, localised subchondral oedema is characteristic. In 50% of all cases, accompanying joint effusion may be found. Common clinical Features that allow Bedside Diagnosis Increased age Pain Stiffness Reduces movement Swelling & Crepitus Diagnosis The diagnosis is based on a history of joint pain worsened by movement, which can lead to disability in activities of daily living. Plain radiography may help in the diagnosis, but laboratory testing usually does not. Finding in Plain X-ray Mnemonic L: loss of joint space O: osteophytes S: subchondral cysts S: subchondral sclerosis Osteophyte is the most specific radiographic marker for OA although it is indicative of relatively advanced disease. Diagnosis differentiation from 1. referred pain 2. periarticular (soft-tissue) conditions 3. somatisation (regional pain in the absence of any local pathological cause) Diagnosis Diagnose osteoarthritis clinically without investigations if a person: Is 45 or over and Has activity-related joint pain and Has either no morning joint-related stiffness or morning stiffness that lasts no longer than 30minutes,unlike rheumatoid arthritis, which causes stiffness for 45 minutes or more. Risk Factors Genetics, Female sex, Past trauma, Advancing age, and Obesity. Involve Joints The joints most commonly affected are The hands, Knees, Hips, and Spine, - But almost any joint can be involved. The pathogenesis of joint pain Synovitis Subchondral bone changes Peripheral pain sensitisation Central pain sensitisation Finally, the experience of pain will be modulated by psychological, social, and other contextual factors Signs and Symptoms of OA Hand Pain on range of motion Hypertrophic changes at distal and proximal interphalangeal joints (Heberden nodes and Bouchard nodes) Tenderness over carpometacarpal joint of thumb Typical findings Heberden’s nodes 1 2 2 Bouchard’s nodes Hand affected by osteoarthritis. (1) Heberden nodes. (2) Bouchard nodes. Radiograph of a hand affected by OA (1) joint space narrowing, (2) osteophytes, and (3) joint destruction. Also note changes at carpometacarpal joint (4), which are very common in osteoarthritis. 2 3 1 4 Shoulder Pain on range of motion Limitation of range of motion, especially external rotation Crepitus on range of motion Knee Pain on range of motion Joint effusion Crepitus on range of motion Presence of popliteal cyst (Baker cyst) Lateral instability Valgus or varus deformity KNEE/(1) joint space narrowing and (2) osteophyte formation. Hip Pain on range of motion Pain in buttock Limitation of range of motion, especially internal rotation Radiograph of the hips showing (1) joint space narrowing and (2) osteophyte formation. Foot Pain on ambulation, especially at first metatarsophalangeal joint Limited range of motion of first metatarsophalangeal joint, hallux rigidus Hallux valgus deformity Spine Pain on range of motion Limitation of range of motion Lower extremity sensory loss, reflex loss, motor weakness caused by nerve root impingement Pseudoclaudication caused by spinal stenosis Physical examination Important in making the diagnosis. Pain and limitation of range of motion are common Each joint has unique physical examination findings Laboratory testing Usually is not required to make the diagnosis. ESR & CRP are typically normal. Immunologic tests, such as ANA & RF (only if evidence of joint inflammation or synovitis) uric acid level (only if gout is suspected). Holistic approach to OA assessment and management Offer advice on the following core treatments to all people with clinical osteoarthritis. Access to appropriate information. Activity and exercise. Interventions to achieve weight loss if the person is overweight or obese Treatment Treatment Four main categories: Nonpharmacologic, Pharmacologic, Complementary and alternative, and Surgical. Begin with the safest and least invasive therapies All patients with OA should receive at least some treatment from the first two categories. NONPHARMACOLOGIC Exercise: Muscle strengthening and range-of-motion exercises. Thermotherapy: local heat or cold should be considered as an adjunct to core treatments. Swimming, elliptical training, and cycling are exercise options for patients with osteoarthritis in weight-bearing joints. Weight reduction Bracing and splinting to help support painful or unstable joints. PHARMACOLOGIC Acetaminophen NSAIDs Opoids Intra-articular injections of corticosteroids or hyaluronic acid combination of glucosamine and chondroitin COMPLEMENTARY AND ALTERNATIVE MEDICINE Acupuncture – LBP glucosamine and chondroitin (GAIT). Balneotherapy (spa therapy or mineral baths). Capsaicin cream S-adenosylmethionine (SAM-e) SURGICAL Indication is continued pain and disability despite conservative treatment. The most effective is total joint replacement. Excellent outcomes for hip, knee, and shoulder. Follow-up and review Monitoring the symptoms and the ongoing impact of the condition on everyday activities and quality of life. Monitoring the long-term course of the condition Discussing person's knowledge & concerns Personal preferences and ability to access services Reviewing effectiveness & tolerability of all treatments Support for self-management. Annual Review For any person with one or more of the following: troublesome joint pain more than one joint with symptoms more than one comorbidity taking regular medication for their osteoarthritis.