Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
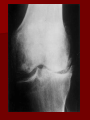
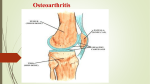
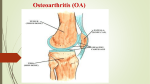
Osteoarthritis Background: Osteoarthritis, the most common type of joint disease, is a heterogeneous group of conditions resulting in common histopathologic and radiologic changes. It is a Degenerative Disorder resulting from the biochemical breakdown of articular cartilage in the synovial joints. Although osteoarthritis is thought to be largely due to excessive wear and tear, secondary nonspecific inflammatory changes may also affect the joints. Mortality/Morbidity: Osteoarthritis typically develops slowly and progresses over several years. Usually, the pain slowly worsens over time, but it may stabilize in some patients. Osteoarthritis of the knee is a leading cause of disability in elderly persons. Osteoarthritis also causes millions of Americans to miss work because of back pain. Race: Primary osteoarthritis affects all races, although the prevalence and patterns of the disease appear to differ. The disorder is more prevalent in Native Americans than in the general population. In persons older than 65 years, osteoarthritis is more common in whites than in blacks. Sex: In individuals older than 55 years, the prevalence of osteoarthritis is higher among women than men. Age: Osteoarthritis occurrence appears to increase with patient age, in a nonlinear fashion Signs and symptoms Primary osteoarthritis is a common disorder of the elderly, and patients are often asymptomatic. Patients with symptoms usually do not notice them until after they are aged 50 years. Deep, achy, joint pain exacerbated by extensive use is the primary symptom. Also, reduced range of motion and crepitus are frequently present. Joint malalignment may be visible. Heberden nodes, which represent palpable osteophytes in the distal interphalangeal joints, are characteristic in women but not men. Inflammatory changes are typically absent or at least not pronounced. Physical: Early in the disease process, physical examination findings include the following: – Joints may appear normal. – Gait may be antalgic if weight-bearing joints are involved. Later in the disease process, physical examination findings include the following: – – – – – Visible osteophytes may be noted. Joints may be warm to palpation. Palpable osteophytes frequently are noted. Joint effusion frequently is evidenced in superficial joints. Range-of-motion limitations, because of bony restrictions and/or soft tissue contractures, are characteristic. – Crepitus with range of motion is not uncommon. Causes: Primary OA, which can be either localized or generalized, is most often idiopathic, except in rare cases where a defective gene has been found to cause a familial form of OA. Secondary OA can be caused by the following: – Obesity (increases mechanical stress) – Repetitive use (ie, jobs requiring heavy labor and bending) – Previous trauma (ie, posttraumatic OA) – Infection – Crystal deposition – Acromegaly – Previous rheumatoid arthritis (ie, burnt-out rheumatoid arthritis) – Heritable metabolic causes (eg, alkaptonuria, hemochromatosis, Wilson disease) – Hemoglobinopathies (eg, sickle cell disease, thalassemia) – Neuropathic disorder leading to a Charcot joint (eg, syringomyelia, tabes dorsalis, diabetes) – Underlying orthopedic disorders (eg, congenital hip dislocation, slipped femoral capital epiphysis) – Disorders of bone (eg, Paget disease, avascular necrosis) Lab Studies: Researchers have looked at monoclonal antibodies, synovial fluid markers, and urinary pyridinium cross-links (ie, breakdown products of cartilage). (ESR) is not usually elevated, but it may be slightly elevated in cases of erosive inflammatory arthritis. Imaging Studies: Plain radiographs – Joint space narrowing – Osteophytes – Subchondral sclerosis – Subchondral cysts MRI Treatment To effectively manage the condition Exercise regularly. Exercise can strengthen muscles, increase range of motion, improve balance and help reduce stress. Good exercises include walking, stationary bicycle riding, water exercises Control weight. Excess body weight adds stress on joints in back, hips, knees and feet Eat a healthy diet. Eating a diet high in vegetables, whole grains and fruits helps maintain a proper weight and good health. Treatment There's no known cure for osteoarthritis, but treatments can help to reduce pain and maintain joint movement. treatments may include medication, self-care, physical therapy and occupational therapy. In some cases, surgical may be necessary. Topical pain relievers. Over-the-counter creams, gels, ointments and sprays can temporarily relieve arthritis pain and reduce inflammation in joints close to the surface of the skin, such as fingers, knees and elbows. Topical pain relievers include trolamine salicylate , methyl salicylate, menthol and camphor, Eucalyptamint, or capsaicin from the seeds of hot chili peppers. Nonsteroidal anti-inflammatory drugs (NSAIDs). These both relieve pain and reduce inflammation. NSAIDs range from aspirin, ibuprofen , ketoprofen , and naproxen sodium. Corticosteroids Intra –Articular can relieve some pain for four to six months. Joint replacement Neutripharmaceticals (( Chondroprotectives )) Glucosamine Chondroitin Sulfate Omega 3 Vit. D + Cal.